Neuroimaging studies have shown a greater temporal lobe and cingulate gyrus hypometabolism in patients with AD who have major depression,
3,4 and neuropathological studies have shown that AD patients with depression also have a greater neuronal loss in the central superior raphe nucleus, locus ceruleus, and substantia nigra.
5–7 Frontal cortical circuits are particularly important in terms of aggression, psychosis, and agitation. Neuropsychological studies have found greater frontal lobe dysfunction in patients with delusions
8 and greater temporal-parietal lobe dysfunction in patients with psychosis (e.g., delusions, visual and auditory hallucinations).
9 Frontal-temporal hypometabolism is greater in patients with delusions;
10,11 and in patients with hallucinations, parietal hypometabolism is greater.
10,11 Similarly, the presence of aggressive behavior
11,12 and psychomotor agitation
12 has been associated with increased frontal lobe dysfunction. In AD patients with agitation, neuropathological studies have found greater neurofibrillary tangle burden in the orbitofrontal cortex.
13Psychiatric symptoms tend to occur within a context of other behavioral syndromes, which indicates a specific system dysfunction. For example, the presence of aggression is associated with psychosis,
9,14 depression,
15 and agitation.
16 Furthermore, the development of psychiatric symptomatology can be influenced by personal characteristics, such as level of education;
17,18 age;
19 gender (male), in cases with physical aggression
16 and agitation;
20,21 and race (African Americans), particularly in cases with psychosis.
18 Although the prevalence of psychiatric symptoms increases as disease progresses,
22 studies have examined the relationship among them at different stages of disease.
This descriptive study was conducted to examine the relationships among major depression, agitation, aggression, and psychosis as they occur within the context of the constellation of psychiatric symptoms and syndromes that are commonly present in AD patients as a function of dementia severity. In addition, we examine how constitutional and personal factors influence the manifestation of psychiatric symptoms at different stages of the disease.
MATERIAL AND METHODS
We analyzed the psychiatric symptoms of 1155 patients who were diagnosed with probable AD
23 at the time of their entry at the Alzheimer's Disease Research Center (ADRC) at the University of Pittsburgh. Each patient received an extensive neuropsychiatric evaluation, including medical history and physical examination, neurologic history and examination, semi-structured psychiatric interview, and neuropsychological assessment.
24 Informed consent was obtained from all ADRC participants. At the conclusion of these studies, each individual set of results was reviewed by the study team (e.g., neurologists, neuropsychologists, and psychiatrists) at a consensus conference. The diagnosis of probable AD was made following the NINCDS-ADRDA criteria
23 and required that patients show gradual cognitive decline without history or evidence of illness other than AD that could cause mental impairment. The inclusion and exclusion criteria have been published previously.
24 In this cohort, the sensitivity for AD was 98%, and specificity was 88%.
24 For the purpose of this study, the severity of the cognitive deficits was graded according to the Mini-Mental State Examination (MMSE)
25 scores: mild (MMSE score ≥20), moderate (MMSE scores between 19 and 10), and severe (MMSE scores ≤9). The patients' demographic characteristics and neurological and psychiatric measures are shown in
Table 1.
Psychiatric Examination
Psychiatric evaluations were conducted by geriatric psychiatrists using a semi-structured interview.
26 From 1991 to the present, all subjects were assessed with the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) Behavioral Rating Scale.
27 The CERAD Behavioral Rating Scale is a psychopathologic scale that reviews relevant signs and symptoms of demented patients and rates symptomatology from 0 to 8 based on the frequency of occurrence. For the purpose of this study, signs and symptoms were recorded as either present or absent. Additionally, the Hamilton Depression Rating Scale (HDRS)
28 and the Blessed Dementia Rating Scale for activities of daily living
29 interviews were completed by the psychiatrist on the basis of data from each patient and primary caregiver. Following psychiatric assessments, diagnoses of psychiatric symptoms are currently made according to the DSM-IV.
30 Patients examined before the publication of the DSM-IV were classified according to the DSM-III
31 and DSM-III-R.
32 These diagnoses are reviewed annually on each patient and, when necessary, modified according to the DSM-IV. Reliability of each item of the CERAD Behavioral scale ranged from kappa .60 to .85 (substantial to near-perfect agreement) among the psychiatrists.
24 One neurologist (O.L.L.) and one psychiatrist (M.H.) reviewed the psychiatrist characteristics of the patients examined before 1991 to confirm homogeneity of the psychiatric symptoms selected for this study.
Agitation occurred when patients showed signs of emotional distress with increased motor activity. Aggression occurred when patients displayed verbal or physically aggressive behavior. Wandering was considered present when patients attempted to leave home and actually walked away. Sundowning was present when patients exhibited increased confusion at dusk or early night hours. Delusions were defined in accordance with the DSM-IV criteria
30 and distinguished from confabulations, disorientation, and amnesia in that a patient had to present persistent false beliefs, despite contrary evidence, in order to be considered delusional. Hallucinations were displayed if the patient spontaneously reported a sensory perception with no concomitant external stimulus.
Statistical Analysis
Chi-square and t tests were used to analyze contingency tables. A logistic regression analysis, controlling for age, race, gender, duration of the symptoms of dementia, MMSE scores, and the use of psychiatric medication (e.g., antidepressants, sedatives/hypnotics/anxiolytics, antipsychotics) was conducted in order to identify psychiatric symptoms associated with the presence of agitation, aggression, and psychosis at different levels of dementia severity.
DISCUSSION
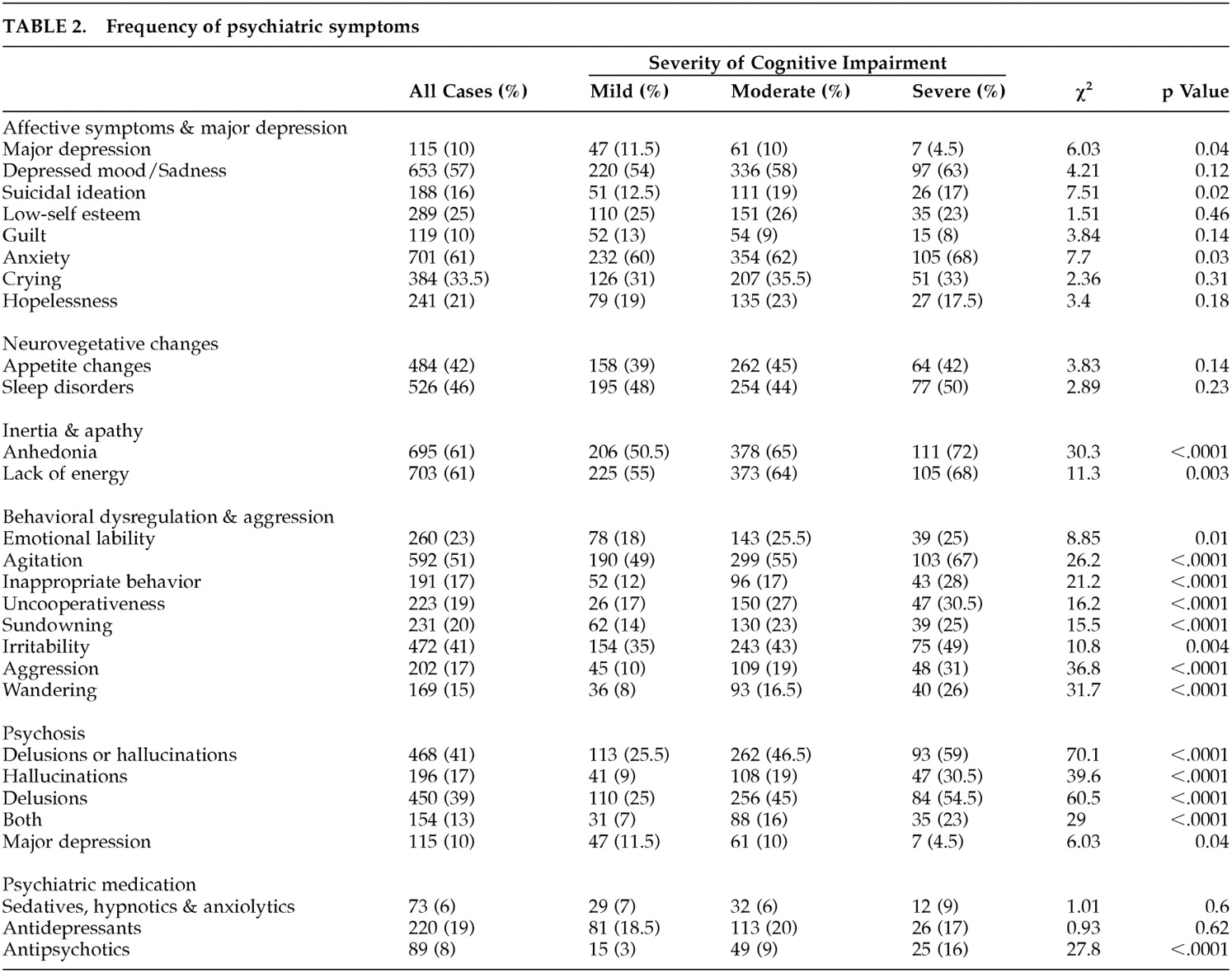
This descriptive study sets the stage for future research. Prior to implementing hypotheses test studies, intervention trials, or neuropathological correlates of psychiatric symptoms, it is first necessary to understand the behavioral context in which these symptoms occur. This study showed that psychiatric symptoms, except major depression, become more frequent in more severe stages of the disease and similar behaviors can occur within the context of different behavioral syndromes. In addition, gender, race, and level of education seem to contribute to the development of specific psychiatric symptoms in AD.
The overall frequency of major depression was 10% in this cohort of probable AD patients, which is within the expected range from referral clinics.
33 However, the frequency of depression varied as a function of the severity of dementia. The lower frequency of major depression in late stages suggests progression of AD pathology that gradually encompasses all cortical structures, thus limiting the patients' insight and ability to communicate depressive symptoms. Consequently, severely impaired patients may not be able to report symptoms of depression. Additionally, these patients may have more abnormal behaviors (e.g., agitation, aggression, anxiety), which may preclude the identification of syndromal major depression.
22,34 Nevertheless, in the opinion of the examining psychiatrists, there was a small group of patients who exhibited major depression. As noted here, the presence of major depression was associated with a clear constellation of depressive symptomatology in mild/moderate stages but not in severe stages. Although some studies have found a relationship between depression and aggression in demented subjects,
15 we did not find any relationship between these two syndromes in probable AD patients (see below).
The frequency of depressive symptoms (e.g., depressed mood, hopelessness, guilt, low-self esteem, crying) did not differ statistically across the levels of increasing cognitive impairment, and anxiety and suicidal ideation were more frequent in late stages. Although the frequency of syndromal major depression decreased in late stages, most of the individual mood-related symptoms appear to have remained stable during the course of the disease. Devanand et al.
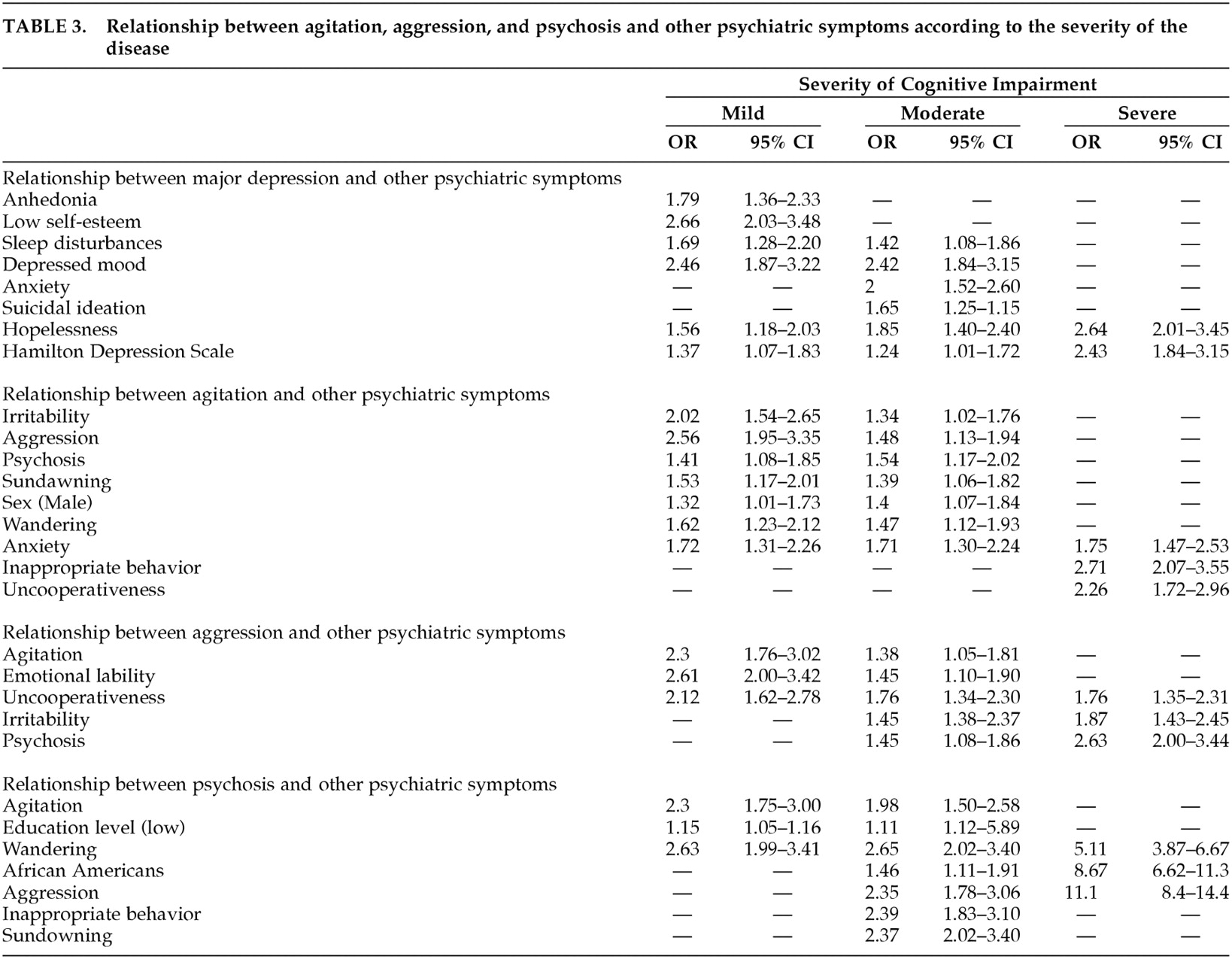
35 followed a group of patients with probable AD and found that the likelihood of a new symptom developing over time was greatest for behavioral problems (e.g., wandering, aggression, agitation, delusions) and least for depressive symptoms. This suggests that the severity of symptoms leads to the diagnosis of major depression. Indeed, in this cohort, patients with major depression had higher Hamilton Depression Scale scores than those without depression (Mild: 11.4 vs. 5.3; moderate: 12.7 vs. 6.0; severe: 19.7 vs. 6.4), and these scores were associated with the presence of depression in the multivariate analysis in all dementia stages.
The association of psychosis with specific psychiatric syndromes depends on the severity of the disease. In mild stages, psychosis was associated with agitation, which includes psychomotor agitation and wandering, and seemed to be the earliest psychiatric symptomatology that accompanied psychosis in AD. In moderate stages, these patients manifested aggression and inappropriate behavior. These results converge with neuropsychological and neuroimaging studies that found a greater limbic (frontal-temporal lobe) dysfunction in AD patients with psychosis and with descriptive studies that revealed an association between psychosis and aggression.
9,10,11,14 Indeed, recent PET studies found that psychosis was associated with dorsolateral prefrontal and medial temporal cortices hypometabolism, while patients with both psychosis and aggression also had a greater hypometabolism in the orbitofrontal cortex.
11 Wandering is part of the agitatation component that accompanies psychosis, and it may also represent the loss of control of limbic frontal functions.
13Anxiety constitutes one of the most common psychiatric symptoms in AD,
22,36 and it has been associated with increased health care utilization and disability in AD patients.
36 Our findings suggest that anxiety can occur in the context of agitation and abnormal behavior or in the context of depression. Teri et al.
36 reported that the presence of anxiety was linked to behavioral disturbances, psychosis, and aggression. Mack et al.
37 conducted a factor analysis of the CERAD Behavioral Rating Scale and observed that anxiety was within the depressive symptom domain.
Aggression was associated with agitation, uncooperativeness, and emotional lability in mild/moderate stages, and psychosis, uncooperativeness, and irritability in moderate/severe stages. These findings suggest a greater compromise of frontal-temporal limbic circuits.
11,14 Although some studies have reported a relationship between aggression and depression in an unselected group of demented patients,
15 our findings suggest that there is no relationship between these two syndromes in probable AD patients.
38 It is possible that the presence of cerebrovascular disease or other neurodegenarative disorders may have accounted for this relationship. As with aggression, agitation was also associated with frontal lobe symptoms in all stages of the disease, although this was more evident in mild/moderate stages. As the disease progresses, patients develop more cognitive deficits that make it difficult for them to verbally manifest psychiatric symptoms, but they can express abnormal behaviors by other means (e.g., inappropriate behavior, uncooperativeness).
Several studies have found that low-level education is associated with psychosis in AD.
17,18 However, our results showed that education was linked to psychosis only in mild and moderate stages of the disease. This finding suggests that low educational attainment (along with early life environmental factors) lowers the threshold for the psychiatric symptomatology of the disease as well as its cognitive manifestation.
39,40 Difficulty in language acquisition or poor linguistic ability as a young adult
41 may increase the risk of the development of psychosis in AD. This appears to be supported by several studies that reported a relationship between language (verbal fluency and receptive language) and psychosis.
8,9,17 Other studies have not reported a relationship between psychosis and education level,
42 although those results are difficult to compare with ours, since the authors did not control for the use of psychiatric medication or other psychiatric symptoms that commonly occur in AD.
Race (African Americans) was associated with psychosis in AD,
18 after controlling for duration of the disease, gender, level of education, and psychiatric treatment. The fact that this relationship only occurred in moderate/severe stages of the disease may be explained by the cohort characteristics. Because this study was conducted in a referral sample, it is possible that African Americans sought medical attention when the disease was more advanced, and thus were more likely to manifest behavioral problems. Indeed, the mean MMSE score at study entry was 13.9 ± 6.4 in African Americans and 16.8 ± 5.8 in whites (
p < .001). Whether genetic markers, environmental factors, medical comorbidities, or cerebrovascular disease contribute to this finding requires further assessment.
Gender (males) was associated with agitation,
16,21 and we did not observe any association between males and psychosis.
20 However, as noted here, agitation occurred in the context of multiple abnormal behaviors, which are interrelated. Cohen et al. found an association between agitation and psychosis only in men while in women, agitation was associated with multiple psychiatric symptoms.
43 The association between gender and abnormal behaviors in AD requires additional studies.
In summary, although affective symptoms are common in AD, syndromal major depression occurs in a small proportion of patients, and its frequency decreases in more severe disease. In contrast, aggression, agitation, and psychosis are more frequent in moderate/severe stages, and they occur within a context of symptoms that indicate a greater frontotemporal lobe involvement of AD pathology.