Corticobasal degeneration (CBD) is a rare neurodegenerative dementia that illustrates the use of functional imaging in geriatric psychiatry. There have been numerous publications related to the more common dementias (such as Alzheimer’s disease [AD]) and functional imaging. Fewer reports are available regarding CBD; functional imaging may be cardinal in differentiating this clinical entity from other dementias and/or movement disorders. CBD typically presents with asymmetric parkinsonism, dystonia or focal myoclonus and specific cognitive-behavioral changes.
1 These include one or more of the following signs: ideomotor apraxia, cortical sensory loss or alien hand phenomenon,
2,3 frontal executive deficits,
4,5 and, less often, dementia.
6 Although first described in 1968, it was not until the early 1990s that this disorder became a focus of clinical and research interest.
7 Investigators have previously referred to CBD as corticodentatonigral degeneration with neuronal achromasia, corticonigral degeneration, corticobasal ganglionic degeneration, or progressive asymmetrical rigidity and apraxia syndrome.
7 Some authors have suggested using the term corticobasal syndrome for the constellation of clinical features considered as defining characteristics of corticobasal degeneration, reserving the term CBD for the histopathological disorder.
8 CBD is now recognized as part of the spectrum of frontotemporal lobar degeneration.
2The prevalence of this disorder is not clear. CBD is less common than other mid- and late-life basal ganglia disorders. In an autopsy series of 226 elderly demented patients, CBD accounted for 1.3% of cases.
9 The mean age at onset is 63 years (SD=7.7), although the disease may occur as young as 28.
2,10 The disease has an insidious onset and is steadily progressive, with a mean duration of 7.9 years (SD=2.6).
2 The clinical diagnosis of CBD is challenging. This disorder may be markedly underdiagnosed, as one report indicates initial recognition to be as low as 35%.
11 CBD may be difficult to differentiate in its early course from Parkinson’s disease (PD) or other parkinsonian disorders, like progressive supranuclear palsy (PSP) or multiple system atrophy (MSA). A lack of initial response to
l-dopa therapy, although nonspecific, helps differentiate CBD from PD. Despite recommended diagnostic criteria for probable CBD, a definitive diagnosis requires neuropathological confirmation.
3Functional Imaging Studies
In recent years, investigators have proposed functional imaging studies as diagnostic tests to help differentiate CBD from other pathologic entities. In the last 10 years, functional imaging studies in CBD have included positron emission tomography (PET), single-photon emission computed tomography (SPECT), functional magnetic resonance imaging (fMRI), and magnetic resonance spectroscopy (MRS). Although the CBD diagnoses were rarely pathologically proven, these studies used established diagnostic criteria. Some compared CBD patients with healthy control subjects, while others contrasted them with patients with other parkinsonian or dementing disorders.
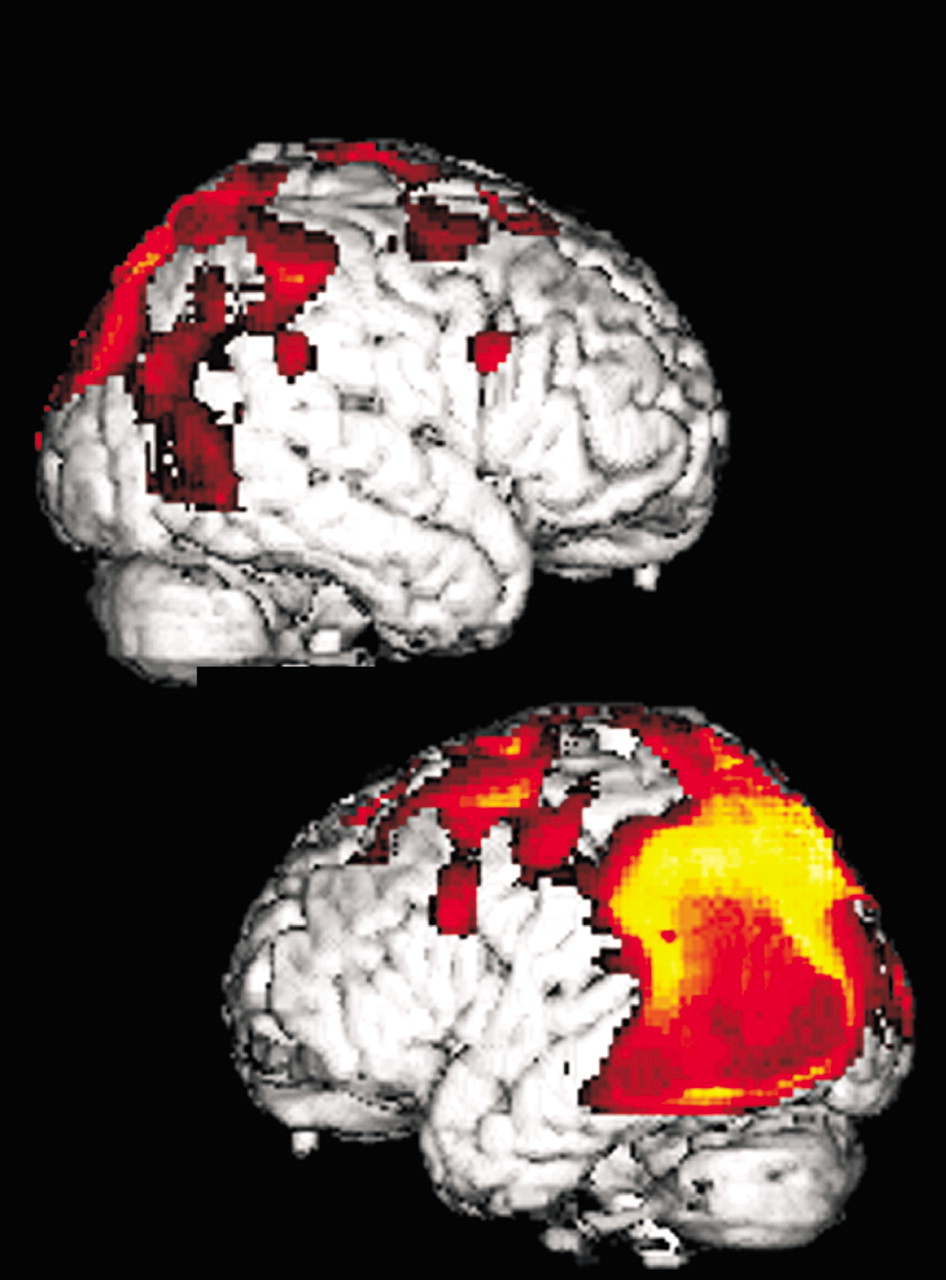
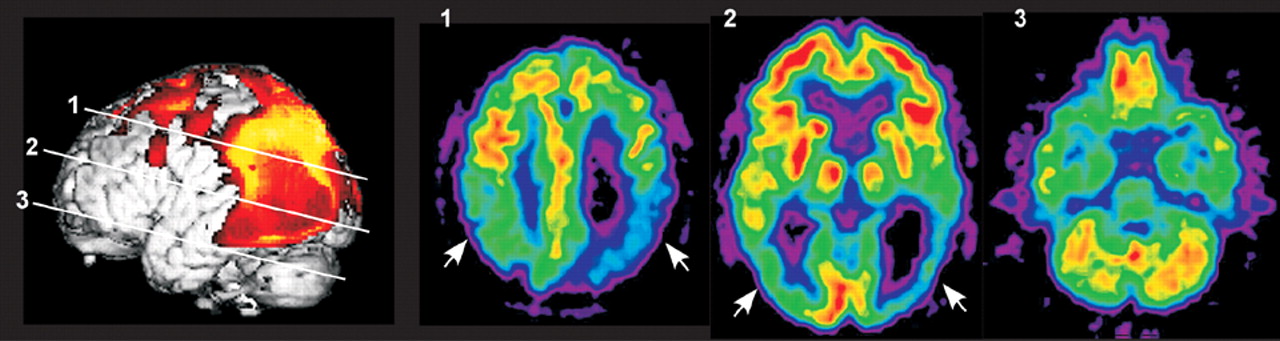
In studies utilizing
18F-fluorodeoxyglucose (FDG) PET, regional cerebral metabolic rate (rCMR) was decreased most commonly in areas of frontal and parietal cortex as well as thalamus and basal ganglia (
Cover and
Figure 1).
24,27–34 Although individual patients varied considerably in the exact location and extent of deficits, primary sensorimotor cortex may be particularly affected in CBD.
30,32,34 Regional asymmetries were consistently found, with more severe hypometabolism contralateral to the more affected side of the body.
24,27–34 However, some studies have reported symmetrical hypometabolism in the presence of asymmetrical clinical deficits or a reversed asymmetry in a few patients.
27,29,32Two studies have compared FDG PET metabolic patterns between patients with PSP, CBD and control subjects.
27,32 Both used statistical parametric mapping, an image analysis technique that allows voxel by voxel comparison of groups of images after they are normalized to a standardized space. Images from the CBD groups were mirrored when necessary so that the most affected side was always the same in order to adjust for the characteristic asymmetry, thus allowing group-wise comparisons. Both studies found that metabolic asymmetry was present in most patients with CBD but not in patients with PSP. In one study, comparison between the CBD (
n=12) and PSP (
n=12) groups revealed a lower metabolism in the inferior parietal lobule, precuneus, and lateral occipital cortex of the more affected hemisphere in the CBD group and a lower metabolism in the anterior cingulate and medial frontal gyri of both hemispheres and the midbrain in the PSP group.
27 In the other study, comparison between PSP (
n=21) and CBD (
n=22) groups indicated more metabolic impairment in sensorimotor, supplementary motor, and parietal cortices in the CBD group and lower metabolism in the midbrain, anterior cingulate, and orbitofrontal regions in the PSP group.
32 These studies suggest that FDG PET may be useful in the differential diagnosis due to the more posterior cortical findings in CBD as compared to the more anterior cortical and midbrain findings in PSP.
Regional cerebral blood flow (rCBF) has been measured by SPECT in patients with CBD using several tracers including
99mTc-hexamethylpropyleneamine oxime (HMPAO),
99mTc-ethylene cysteinate dimer, and N-isopropyl-p[
123I]-iodoamphetamine. The most common findings have been marked perfusion asymmetry in the posterior frontal and parietal regions, with hypoperfusion contralateral to the most affected side.
22,23,35–40 Other commonly affected areas are temporal cortex, basal ganglia, thalamus and pontocerebellar regions.
22,36–40 One study reported that CBD patients with dementia had significant reductions of relative rCBF in the inferior prefrontal region of the more affected hemisphere, compared to CBD patients without dementia.
40 Another found widespread decreases in absolute rCBF in patients with CBD (
n=13), compared to control subjects (
n=10), indicating that use of relative measures may not be fully informative in this group.
36Three studies have utilized SPECT to compare rCBF between patients with CBD and other parkinsonian or dementing disorders.
37–39 All three measured predetermined regions of interest. Although most regions of interest were placed in roughly similar areas (frontal, parietal, temporal, and occipital cortices, basal ganglia, thalamus, and cerebellum) in both studies comparing patients with CBD and with PSP, the results were quite different. In a study measuring absolute rCBF, values did not differ significantly between PSP (
n=12) and CBD (
n=12).
37 In a study measuring relative rCBF, values were significantly lower in inferior frontal, sensorimotor, and posterior parietal cortices in patients with CBD (
n=6) compared to patients with PSP (
n=5).
39 Technique differences as well as differences in patient samples (e.g., illness duration, clinical presentation, inclusion of cognitive deficits) may be reasons why these findings are not consistent. Both studies found significantly higher asymmetry indices in CBD particularly in posterior frontal and parietal regions, similar to the differences in rCMR described previously. The third study found that rCBF was significantly lower in anterior cingulate cortex, sensorimotor cortex, basal ganglia and thalamus in patients with CBD compared to patients with AD. In contrast, rCBF was significantly lower in posterior parietal cortex in patients with AD compared to patients with CBD.
38 Patients with CBD also had significantly higher asymmetry indices in inferior prefrontal and sensorimotor cortices, whereas patients with AD had significantly higher asymmetry indices in lateral and medial prefrontal cortex and posterior parietal cortex.
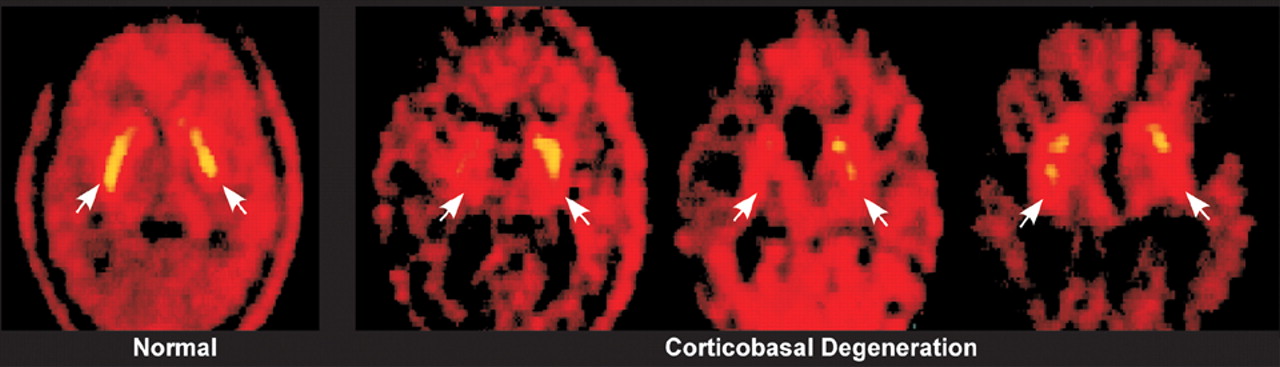
Several methods have been used to image the dopamine system in CBD. Two studies utilized fluorodopa (FDOPA) PET to assess functional integrity of dopaminergic neurons in the striatum.
33,34 Normally, uptake is uniform throughout caudate and putamen bilaterally. Both studies found that uptake was decreased in patients with CBD (total
n=10) compared to control subjects (total
n=18), particularly contralateral to the more affected side of the body (
Figure 2). There was considerable variability in the distribution, with some individuals showing symmetrical decreases.
33 Compared to patients with PD (
n=15), patients with CBD (
n=6) had more uptake (less decrease).
33 A third study utilized [
123I]-2β-carbomethoxy-3-β-(iodophenyl)tropane ([
123I]β-CIT) SPECT, a cocaine derivative with high affinity for dopamine transporters and thus another marker of presynaptic dopaminergic neurons.
41 Patients with MSA (
n=18), PSP (
n=8), PD (
n=48), and CBD (
n=4) were compared to control subjects (
n=14) and each other. Overall β-CIT striatal binding was significantly reduced in all patient groups compared to control subjects, with the CBD group least affected. Asymmetry of striatal β-CIT binding was greatest in patients with CBD, but was found only in 2 of the 4. The authors concluded that β-CIT SPECT was a reliable tool for visualizing presynaptic dopaminergic lesions in patients with MSA, PSP and CBD, however it was inferior to other imaging modalities in differentiating these disorders from PD. Another SPECT tracer that binds to the dopamine transporter is [2-[[2-[[[3-(4-chlorophenyl)-8-methyl-8-azabicyclo[3.2.1]oct-2-yl] methyl](2-mercaptoethyl)amino]ethyl]amino]ethanethi olato(3-)-
N2,N2′,S2,S2′]oxo-[1R-(exo-exo]-[
99mTc]technetium ([
99mTc]TRODAT-1). It has been used to compare striatal function in patients with CBD (
n=5) and idiopathic PD (
n=10) to control subjects (
n=10) and each other.
42 As was found in previously discussed studies, striatal binding was significantly reduced in both patient groups compared to control subjects. Unlike previous studies, there was no significant difference in striatal binding between the CBD and PD groups and both exhibited asymmetry. Regional analysis revealed that binding was reduced similarly in both caudate and putamen in the patients with CBD, whereas binding was relatively preserved in the caudate and decreased in the putamen in the PD patients. Postsynaptic dopaminergic D2 receptors were measured in an individual with CBD utilizing
123mI-iodobenzamide (IBZM) SPECT.
35 Tracer uptake was severely reduced in the basal ganglia contralateral to the symptoms. Overall these studies indicate that the striatal dopaminergic system is impaired in CBD, but probably less severely than in other parkinsonian disorders.
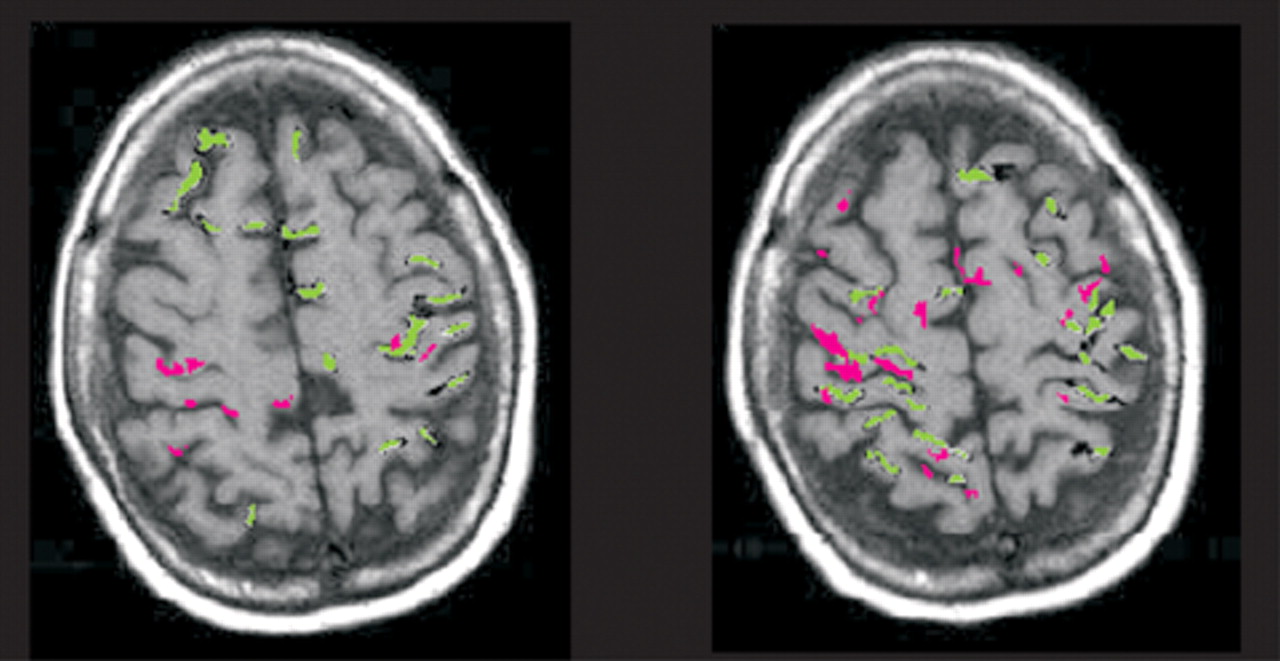
One group has used fMRI to probe cortical function in patients with CBD (total
n=8).
22,23 Two finger opposition tasks of differing difficulty were used. In the simple task, each finger in order (starting with digit 2, the index finger) was touched to the thumb (digit 1). In the complex task a specified sequence was followed (1–2, 1–4, 1–3, 1–5). Activation of the contralateral sensorimotor, supplementary motor, and parietal cortex and of the ipsilateral prefrontal cortices occurred during the execution of the simple motor task with the unaffected hand. In contrast, decreased activation of the contralateral sensorimotor and parietal cortices and supplementary motor area occurred during performance of the same task with the affected hand (
Figure 3). During performance of the complex motor task with the unaffected hand, there was bilateral activation of the sensorimotor and parietal cortices and activation of the contralateral frontal cortex. During performance of the same task with the affected hand, there was bilateral activation of the sensorimotor cortex and supplementary motor area, but only modest bilateral activation of the parietal cortex, particularly contralaterally (Figure 3). These results suggest parietal lobe dysfunction contralateral to the affected hand. The authors comment that the parietal lobe participates in the motor control of movements in the intrapersonal space. There are connections between the inferior parietal lobe and inferior premotor area (which may store elementary motor programs). Thus, parietal lobe dysfunction can disconnect the supplementary motor, premotor, and sensorimotor areas. The authors propose that fMRI can provide evidence of asymmetrical disorganization of the hierarchical cortical motor program, before structural and even SPECT changes become evident.
Magnetic resonance spectroscopy provides a relative measure of particular metabolites, most commonly presented as spectra of the amount of signal produced by each from a volume of interest (voxel) rather than as images. Three studies have utilized proton (
1H) MRS to examine patients with CBD and related diseases (PSP, PD, MSA, vascular parkinsonism, primary progressive aphasia, frontotemporal dementia).
43–45 With
1H MRS the metabolites of interest are
N-acetyl aspartate, choline, and creatine.
N-Acetyl aspartate is present almost exclusively within neurons and indicates neuronal/axonal density. Choline is mostly present within membrane constituents and can be elevated both as a result of increased synthesis and destruction. Creatine is present alone and as part of phosphocreatinine, both of which are important for energy metabolism. While this peak is normally quite stable and commonly used as a reference standard, it does change in some conditions. The only region included in all 3 studies was the basal ganglia. Although the voxel placement varied, all reported either decreased
N-acetyl aspartate/creatine or decreased
N-acetyl aspartate/choline.
43–45 Two studies found decreased
N-acetyl aspartate/creatine in frontal cortex.
44,45 Other areas reported to be affected include the centrum semiovale, parietal cortex, and perisylvian cortex. The factors that differentiated CBD from other entities (e.g., PSP, MSA, frontotemporal dementia) were marked asymmetry and perhaps involvement of parietal cortex.
In summary, the most salient findings in these functional imaging studies are asymmetrical hypoperfusion on SPECT and asymmetrical hypometabolism on PET involving the parietofrontal cortex, basal ganglia and thalamus. These findings suggest that multiple components of neural networks related to both movement execution and production of skilled movements are disturbed in CBD.
32 The functional imaging results may confirm a clinical diagnosis of probable CBD and support the diagnosis in patients who do not fulfill sufficient clinical criteria.
46 The few reports looking at CBD using fMRI and MRS appear to support the presence of hemispheric asymmetry early in the disease.