Throughout the world several million people are affected by war every year. Posttraumatic stress disorder (PTSD) is a frequent consequence of war experience (
1,
2 ), although exact prevalence rates vary and may be context dependent. People with ongoing PTSD pose a challenge to health care services in war-affected areas (
3 ), and there has been some debate on the most effective way to treat them. One approach is to establish specialized treatment centers after the conflict subsides where people with PTSD receive psychiatric treatment from experts who are both clinically qualified and familiar with the local context. However, questions arise about what outcomes the centers achieve in practice, which patients are likely to benefit more or less, and how much treatment costs. So far, there is little research evidence that can be used to answer these questions.
An extensive literature on psychological and pharmacological treatment of PTSD has provided sound evidence that treatment can be effective in reducing symptoms (
4,
5 ). However, most of this evidence is related to survivors of single traumatic events in nonwar settings. Only a few randomized controlled trials have recruited patients with PTSD after protracted war experience (
6,
7,
8,
9 ). To our knowledge, no experimental study on the effectiveness of treatment has been conducted in a war-affected area with patients who have suffered from PTSD for several years.
Such research is difficult for several reasons. In postwar situations, neither the infrastructure nor the funding to conduct appropriate trials usually exists, and societal priorities may not include implementation of research studies with rigorous designs. Therefore, studies of the treatment of PTSD in postwar regions are scarce, and most of the published research on treatment of war-related PTSD has been conducted with people from war-affected areas who sought refuge in Western countries.
During and after the war in former Yugoslavia in the 1990s, specialized treatment centers for patients with PTSD were established in Bosnia-Herzegovina, Croatia, and Serbia. During that time these centers received funding, guidance, and training from a number of national and international bodies and aimed to provide the best possible treatment in the given context. With respect to specific treatment modalities and components, there were commonalities as well as differences across centers. However, all centers have seen several thousand patients, and they accumulated extensive experience in the treatment of patients with PTSD in war-affected areas. At a time when these centers were already well established, we conducted an observational study in four prominent centers in Bosnia-Herzegovina, Croatia, and Serbia and assessed treatment outcomes and costs.
The study addressed three research questions: What are the treatment outcomes in the specialized centers for patients with PTSD after war experience—that is, how many patients recover from PTSD 12 months after the beginning of treatment, and what changes occur in PTSD symptoms and subjective quality of life? What are the costs of treatment, and are they linked to outcomes? What patient characteristics are associated with more or less favorable outcomes?
Methods
This was an exploratory prospective study funded by the European Commission. The study used an observational and longitudinal design to assess patients in specialized treatment centers at baseline and follow-up interviews over one year. Details of the background, rationale, and approach of the study have been published elsewhere (
10 ).
Settings and participants
The study was conducted in four specialized centers in three countries, Bosnia-Herzegovina (Sarajevo), Croatia (Rijeka and Zagreb), and Serbia (Belgrade). At the time of the study each of the centers had been in existence for more than six years and operated under established policies. Each center had a leading national role in the care of people with war-related PTSD.
All patients consecutively entering a new treatment at the participating centers between the end of 2002 and mid-2004 were considered for eligibility for the study. To be included, patients had to have been born in former Yugoslavia, to be between the ages of 18 and 65, to have had direct exposure to potentially traumatic events during the war in former Yugoslavia in the 1990s, and to have a current diagnosis of PTSD established with the Clinician-Administered PTSD Scale for DSM-IV (CAPS) (
11 ). We used no other criteria and also included some patients who were beginning treatment but who had already had psychiatric treatment in the past for PTSD or another psychiatric disorder. This inclusive approach was intended to reflect the clinical reality at the participating centers, which received referrals of patients with varying characteristics.
Measurements
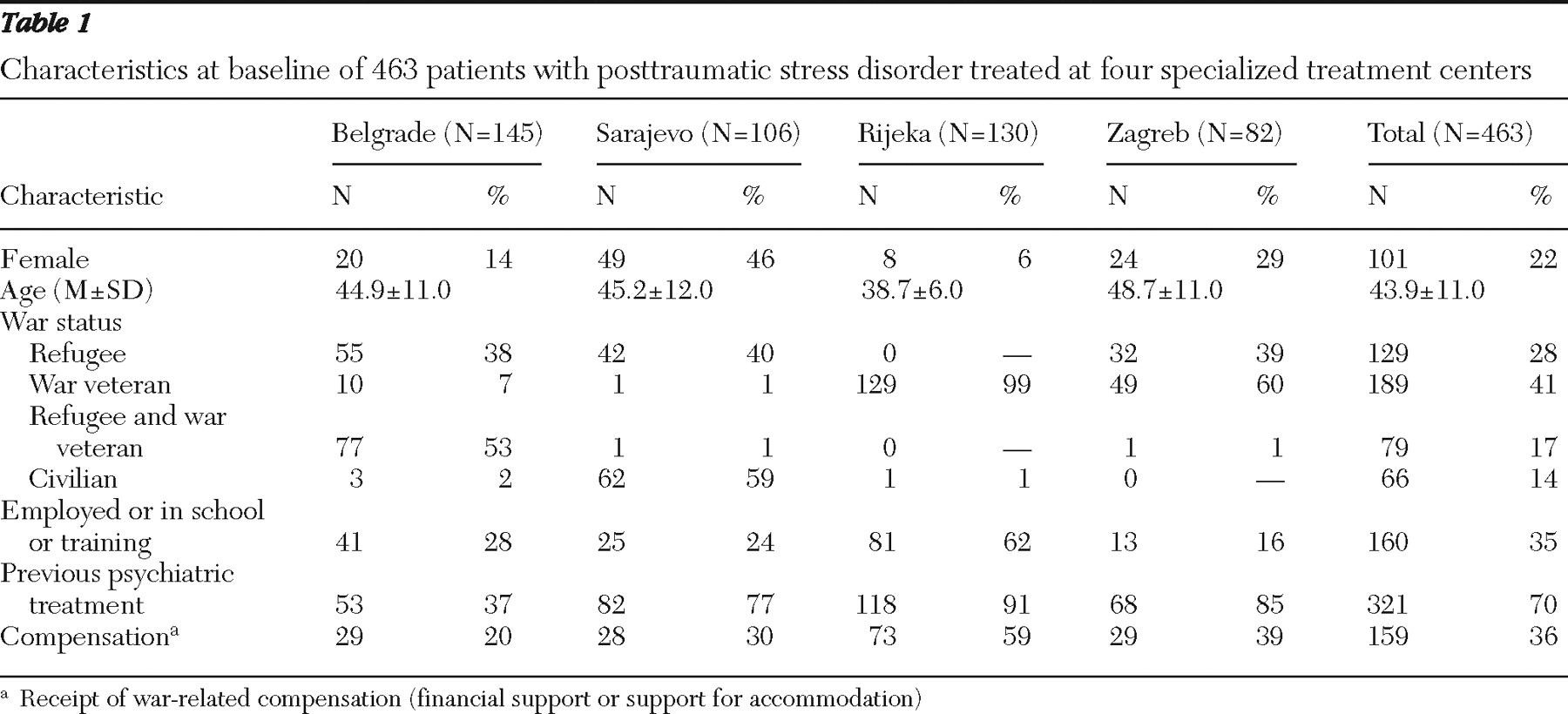
Before treatment began, sociodemographic and clinical characteristics were obtained, including patients' age, gender, war status (war veteran, refugee, both war veteran and refugee, and civilian), receipt of any psychiatric treatment since the war (yes or no), current employment (yes or no), and receipt of war-related compensation (financial support or support for accommodation).
The CAPS (
11 ) was used to determine whether the patient had a current diagnosis of PTSD and the level of PTSD symptoms. It is a structured clinical interview designed to assess the symptoms of PTSD outlined in
DSM-IV. We used the original scoring of Blake and colleagues (
12 ), which considers a PTSD symptom to be present if the frequency of the corresponding CAPS item is 1 or higher and the intensity is 2 or higher. Symptoms of posttraumatic stress were also assessed on the Impact of Event Scale Revised (IES-R) (
13 ). The scale assesses 22 symptoms on 5-point Likert scales (from 0 to 4). Subjective quality of life was assessed with the Manchester Short Assessment of Quality of Life (MANSA) (
14 ), which has been used in studies of patients with PTSD (
15 ). It contains 12 items for rating satisfaction with different life domains on Likert scales ranging from 1, worst satisfaction, to 7, highest satisfaction. The mean score of these 12 items was taken as a measure of subjective quality of life.
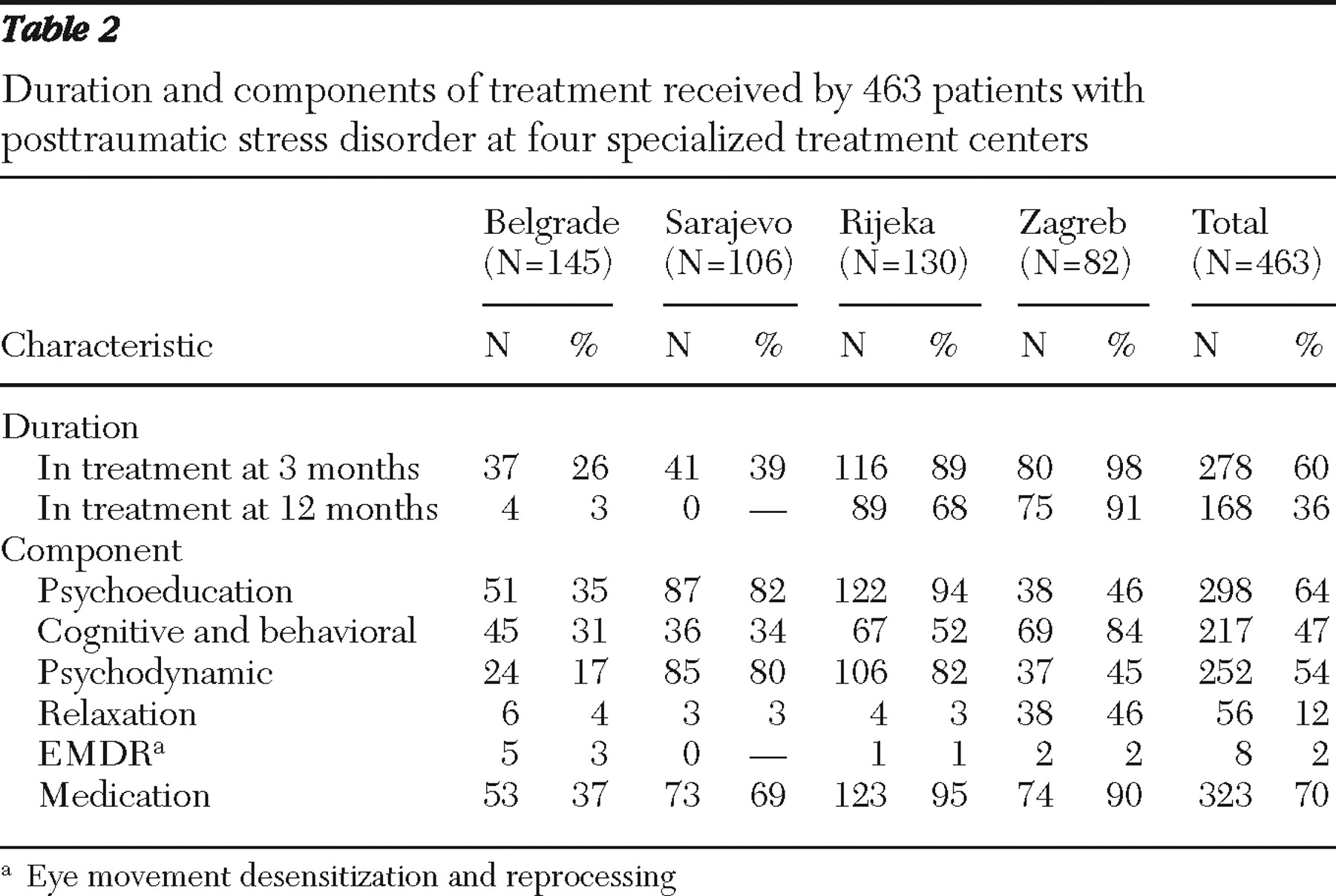
At each center the components of treatment were recorded by using a list developed by the research team with input from clinical experts from each center. Use of health services and receipt of other support were measured on the Client Service Receipt Inventory over the 12-month follow-up period (
16 ). The instrument captured use of services in the treatment center and in associated psychiatric hospital units and day hospitals. Service use was combined with unit costs to generate costs of services per patient.
The primary outcome was a diagnosis of PTSD on CAPS as assessed 12 months after the beginning of treatment. The same time period was used across all centers for a consistent analysis, although actual treatments were expected to vary and to frequently be much shorter or longer than 12 months.
All study measures were translated into Bosnian, Serbian, and Croatian. Back translation was used to check the wording.
Procedure
Patients were first informed about the study by their clinician, who asked for their consent to be approached by a researcher for an interview. If they consented, a researcher who was not involved in the treatment of the patient arranged a baseline interview and obtained written informed consent. All interviewers were qualified psychologists or physicians who received additional training in administering the study instruments.
Across all centers, follow-up interviews were conducted three and 12 months after the start of treatment. At three months costs were assessed for the first three-month period, and at 12 months costs were assessed for the subsequent nine months before the one-year follow-up. Ethics approval was obtained for the relevant committees at all centers.
Data analysis
Descriptive statistics were used for analysis of the sample characteristics. Univariate statistics were used to explore differences between patients who dropped out and those who did not and to test changes in continuous CAPS, IES-R, and MANSA scores between baseline and follow-up. Tests of statistical significance were applied to the total sample, not to the samples at the separate centers, to address the research question about improvements that are generally achieved in such centers and also to reduce problems of multiple testing with different sample sizes.
Univariate and multivariate logistic regression analyses were applied to explore the associations between potential predictor variables (age, gender, being employed or in school or training, previous treatment, compensation, war status, and level of PTSD symptoms at baseline) and PTSD at follow-up. Missing variables were imputed for the multivariate logistic regression. Given the colinearity between center and war status, we chose war status (war veteran versus other war status) rather than center as a predictor.
Information on the use of interventions was combined with unit costs to assess treatment costs. The relationship between PTSD status at 12 months and costs was examined. The confidence interval around the cost difference for those with and without PTSD was produced by using a bootstrapped regression model.
Results
Sample at baseline and follow-up
In the four centers 617 patients were identified as potentially eligible for participation and contacted (Belgrade, 190; Sarajevo, 176; Rijeka, 133; and Zagreb, 118). Of these, 91 were not interviewed: 18 did not consent (Belgrade, four; Sarajevo, 14) and 73 did not meet the inclusion criteria (Belgrade, 11; Sarajevo, 51; and Zagreb, 11).
Of 526 patients who were interviewed (Belgrade, 175; Sarajevo, 111; Rijeka, 133; Zagreb, 107), 463 (88%) met diagnostic criteria for PTSD at baseline and were included in the study (Belgrade, 145; Sarajevo, 106; Rijeka, 130; and Zagreb, 82). Of the 463 patients, 380 (82%) were interviewed at 12 months (Belgrade, 100; Sarajevo, 99; Rijeka, 105; and Zagreb, 76). The 380 participants who were reinterviewed at 12 months and the 83 who were not did not differ significantly on any of the study variables.
Samples and treatments in the centers
Except for six patients in Belgrade whose first war-related traumatic experience occurred in 1999 and was linked to the conflict in Kosovo, all patients had experienced traumatic events associated with the war between 1992 and 1995. Thus the time period between the war-related traumatic event and the beginning of treatment was seven years or more for almost all patients. Sociodemographic and clinical baseline characteristics of patients at the four centers are shown in
Table 1, and duration of treatment and treatment components are listed in
Table 2 . Characteristics of patients varied across centers, and treatment methods were inconsistent both within and across centers.
Outcomes
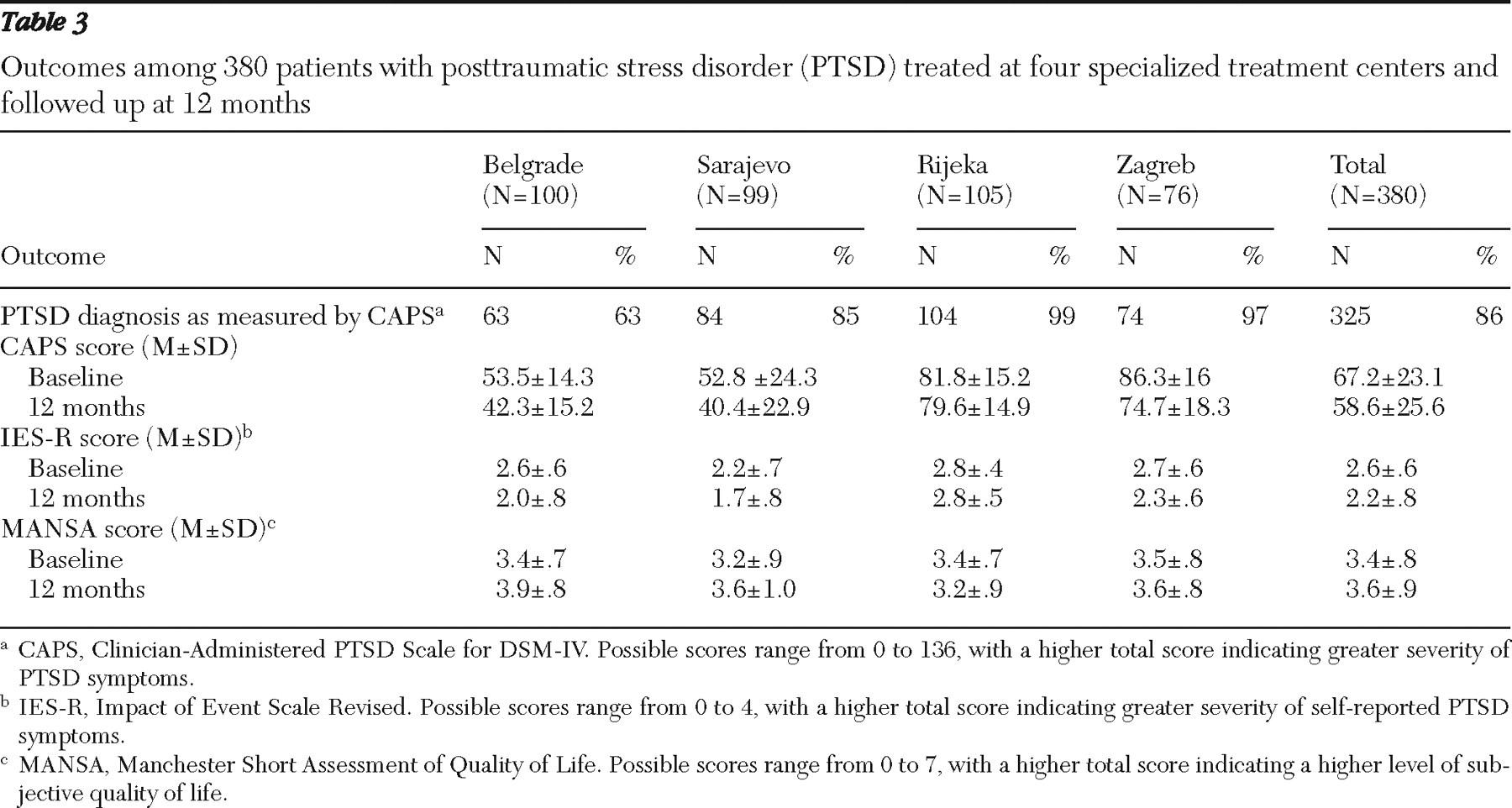
Patient outcomes are shown in
Table 3 . Of the 380 participants interviewed at 12 months, 55 (14%) no longer met criteria for PTSD, whereas 325 (86%) patients did.
CAPS, IES-R, and MANSA scores showed small improvements at each center, except for Rijeka where IES-R scores remained unchanged and MANSA scores indicated slight deterioration in quality of life. For the total sample, improvements were statistically significant (CAPS: Wilcoxon signed rank test, z=–9.64, N=370, p<.001; IES-R: Wilcoxon signed rank test, z=–9.78, N=379, p<.001; and MANSA: t=–4.68, df=374, p<.001). However, MANSA scores at baseline and follow-up were both below the neutral midpoint of 4, indicating overall dissatisfaction with life.
Service costs
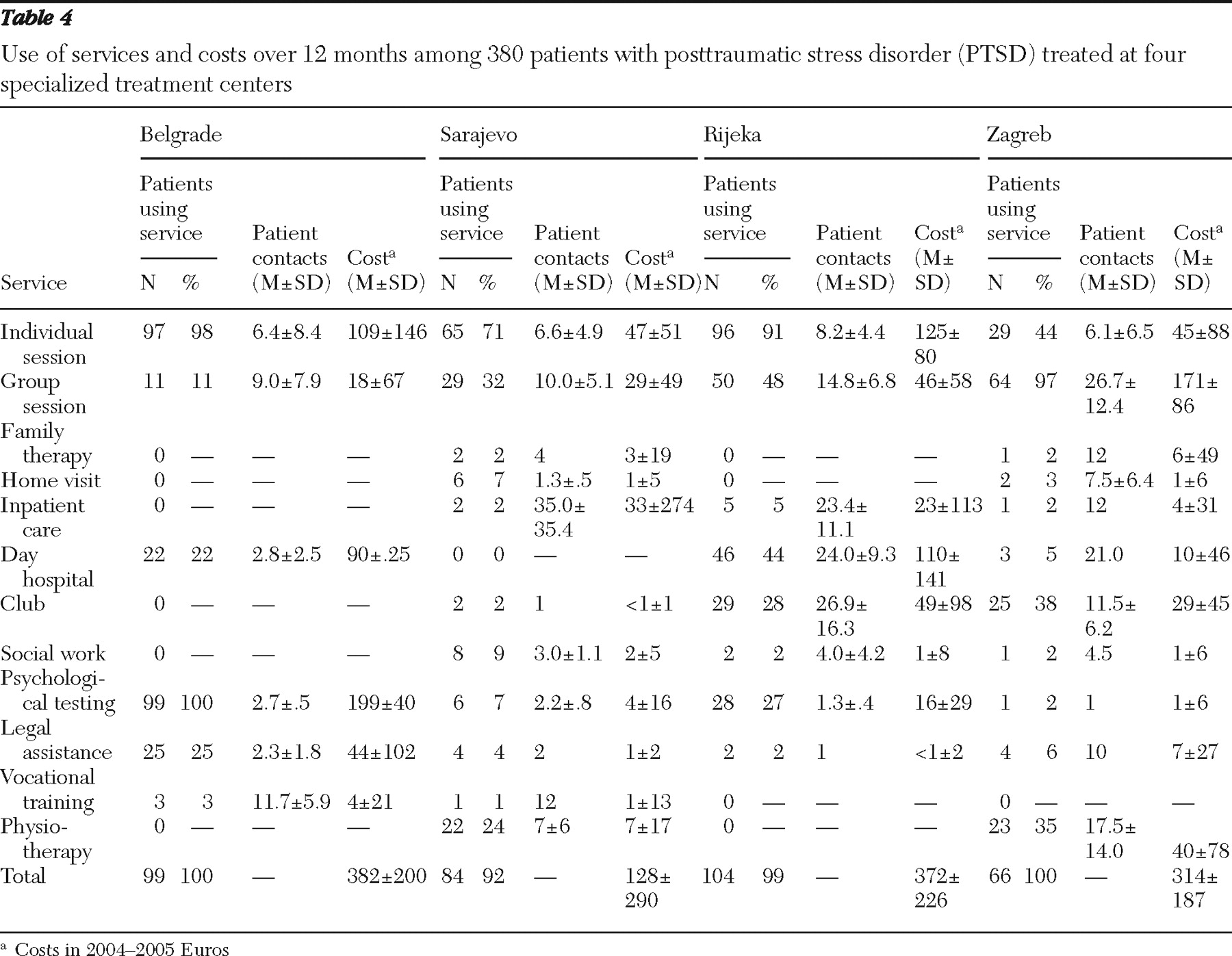
Table 4 provides data on the services patients used during the 12-month period and on the costs for use of the services at the treatment centers and associated psychiatric hospital units and day hospitals (in 2004–2005 Euros). Pharmacological and psychological treatment components and other interventions varied between centers, as did intervention costs. In Zagreb the most costly intervention was group therapy sessions, in Belgrade it was psychological testing, and in Sarajevo and Rijeka it was individual sessions. Total costs in Zagreb, Belgrade, and Rijeka were relatively similar (between €314 and €382 per person). Total costs in Sarajevo were substantially lower (€128).
The mean±SD 12-month costs for those who met criteria for PTSD at 12 months was €307±€260. For those without PTSD the figure was €284±€218. The difference of €23 was not statistically significant (bootstrapped 95% confidence interval=–€46 to €88).
Factors associated with recovery from PTSD
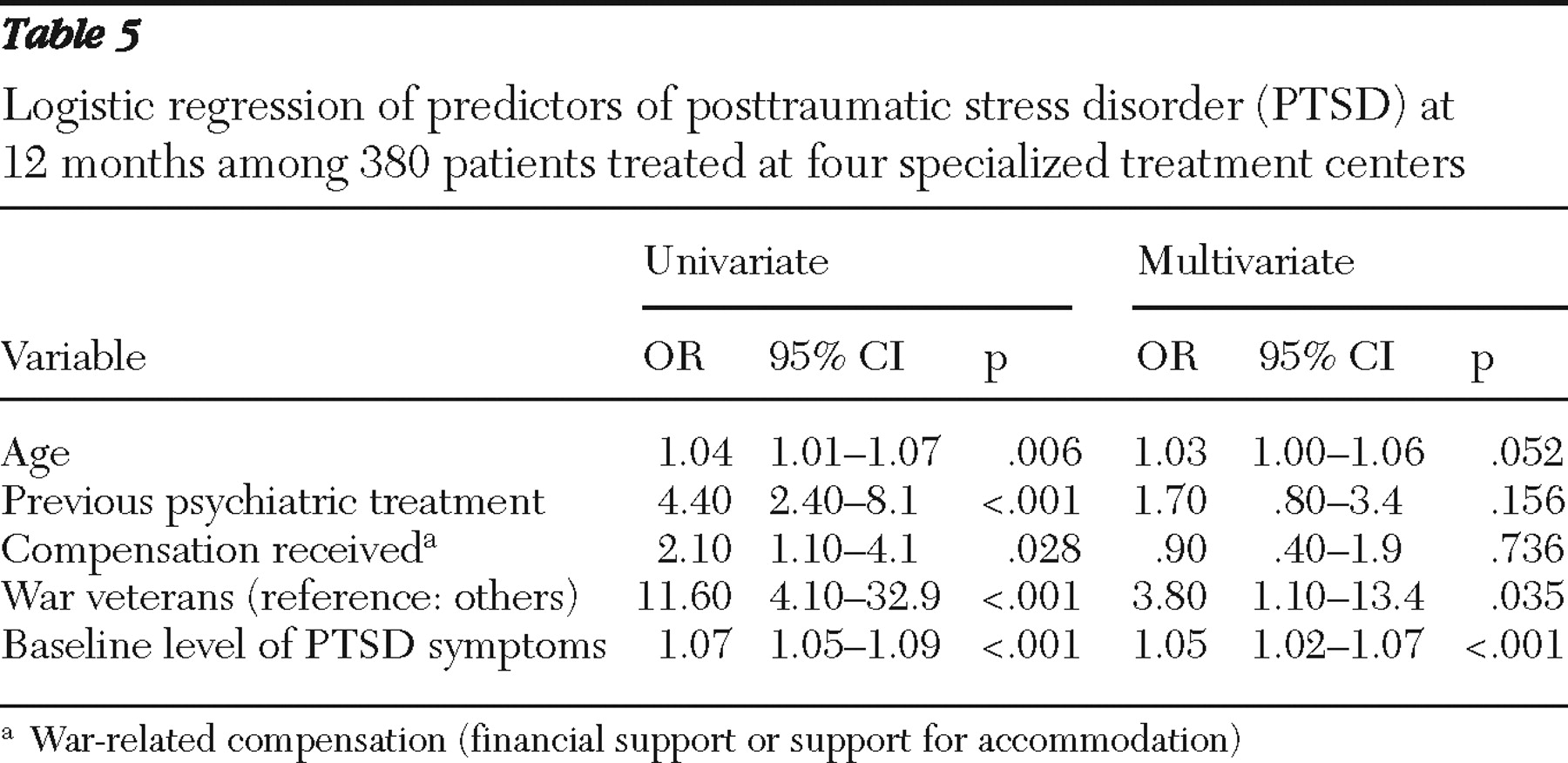
Results of the univariate and multivariate logistic regression analyses to identify factors associated with recovery from PTSD are shown in
Table 5 . In the univariate analysis, not being a war veteran, younger age, not receiving previous psychiatric treatment, not receiving compensation, and lower baseline PTSD symptoms were significantly associated with a positive outcome at 12 months. In the multivariate analysis, lower baseline level of PTSD symptoms and not being a war veteran remained significantly associated with a positive outcome, whereas younger age was of borderline significance (p=.052).
Discussion
Both the characteristics of patients and the forms of treatment varied at specialized centers for the treatment of war-related PTSD that were set up after the war in former Yugoslavia. The overall success rate was low, and 86% of patients still met the criteria for PTSD one year after the beginning of treatment. For the entire sample, reductions in symptom severity and the improvements in subjective quality of life were small, although statistically significant. Treatment outcome was particularly unfavorable for war veterans and those with higher levels of PTSD symptoms at baseline. Treatment costs were not linked to outcomes.
The study had two major limitations. First, it was an observational study and did not employ an experimental design, which would have permitted us to determine the effectiveness of treatment. Second, sample characteristics and treatment methods varied widely across centers, and the statistical analyses could not adjust for this variation. A naturalistic design was used in order to take an inclusive approach and reflect as much as possible the actual clientele and service provision at these centers along with the variation between them.
One can only speculate about what the one-year outcome would have been if the patients had not received treatment. A previous study of persons with untreated PTSD after the war in former Yugoslavia also suggests a low percentage of recovery over time (
17 ). However, the one-year recovery rate of 14% is low and likely to be disappointing to those who funded, established, and operate the specialized treatment centers. The finding of poor outcomes is consistent with the results of a similar prospective study that found no improvement in PTSD symptoms and quality-of-life scores among 70 Croatian veterans after eight months of psychological treatment (
18 ). It is not known whether the small changes in symptom levels and subjective quality of life should be seen as a statistical regression to the mean, a minor effect with little clinical significance, or a relevant improvement.
There are at least two explanations for the marked difference between outcomes in experimental trials and in this observational study. The samples in experimental trials are likely to include patients with characteristics different from those in this study. Seventy percent of patients in this study had received psychiatric treatment after the war and before they entered treatment in the specialized centers, and 36% were receiving compensation for ongoing distress resulting from PTSD. Previous receipt of treatment and current receipt of compensation are exclusion criteria in some treatment trials. Patients who still suffered from PTSD several years after the war and who often had one or more failed psychiatric treatments for PTSD may have represented a group of difficult-to-treat patients. Many patients had combat experience. The recovery rate for war veterans was even lower than for others, and the poorer prognosis for this group held true when the influence of other variables was adjusted for in a multivariate analysis. Limited treatment outcomes in samples with chronic combat-related PTSD have been documented in other studies (
19,
20,
21,
22 ), and a review of psychological treatments for chronic PTSD suggested that veterans might be a particularly difficult population to treat (
23 ). A substantial number of patients in our study were displaced refugees, and poor outcomes of PTSD treatment for refugees have also been reported in other studies (
24,
25 ). One might argue that significant improvements are unlikely to be achieved with any established treatment for patients with the characteristics seen in this study.
It is possible that the centers did not use manuals for the treatments that were applied in effectiveness trials or that fidelity to the manuals was not monitored with sufficient rigor. The treatment methods used may also have been inappropriate, and outcome might have been significantly better with different treatment methods, evidence based or not. One can only speculate about this, but it should be kept in mind that the centers employed experienced therapists and were already well established.
It is difficult to determine whether the differences in recovery rates between centers are relevant. Even at the center with the most positive results (Belgrade), 63% of patients had PTSD a year after entering treatment, and patients at the center differed from those in other centers. Belgrade patients had lower CAPS baseline scores than those at other centers, fewer previous psychiatric treatments, and the highest rate of study dropout. All these factors may have contributed to the more favorable outcomes. Belgrade patients also had shorter treatments, which makes it unlikely that the low overall recovery rate is attributable to the brevity of treatment at the other centers or that one year is too short a time to capture relevant improvements.
Conclusions
Recovery from PTSD was not associated with service costs, and the low recovery rate cannot be seen merely as a result of underinvestment in service provision. Caution should be used in generalizing these findings to other institutions and other postwar contexts. For instance, a study in an African refugee camp identified positive effects of narrative exposure therapy and trauma counseling for patients with PTSD (
26 ). However, the sample was identified in a survey and did not consist of people actively seeking treatment many years after the war.
The findings call for more research focused on specialized treatment centers for war-related PTSD and for challenges of their rationale and approach. One option would be revising the treatment programs, possibly with a stronger focus on one or two treatment methods in each center to support training, supervision, and quality control. A case can also be made for developing and testing new therapeutic approaches, particularly for war veterans, who had an especially unfavorable treatment prognosis in this study. Such new treatment approaches might be less trauma focused and more solution and resource oriented (
22 ). Alternatively, provision of treatment and support in other settings, such as primary care, or use of social interventions might be considered. However, these alternative approaches would be based on as little evidence of effectiveness as there is for the specialized treatment centers.
Acknowledgments and disclosures
The study was supported by a grant from the European Commission Framework Programme 5 (contract ICA2-CT-2002-10002).
The authors report no competing interests.