Research suggests that a significant proportion of jail and prison inmates have a serious mental illness (
1). A quarter of all local jail inmates in 2002 had at least one previously diagnosed mental health condition when arrested, and almost 46% of jail inmates with previous diagnoses had taken a psychotherapeutic medication while incarcerated (
2).
Many refer to this phenomenon as the criminalization of mental illness and point to deinstitutionalization of the mental health system between the 1950s and 1990s as a primary cause (
3). Among the causes of deinstitutionalization were the limits that the Supreme Court placed on the authority of the state to confine individuals involuntarily in the 1970s. In one case in particular,
O'Connor v. Donaldson, the court ruled that individuals could not be institutionalized without treatment when they were not dangerous and were capable of living by themselves or with the aid of family (
4). This ruling prevented states from confining individuals with mental illnesses merely for custodial care.
In Florida, the response to the legal issues associated with involuntary examination was addressed by the passage of the Baker Act (Ch 394, Part 1, Florida Statutes) in 1971 (
5). Like statutes in most states, the Baker Act created different criteria and processes for short-term involuntary examination and longer-term involuntary placements. Individuals who appear to have a mental illness, who are not competent to or not willing to consent to voluntary treatment, and who appear without treatment either to be unable to care for themselves or to present a substantial likelihood of bodily harm to themselves or others can be committed to receiving facilities that have been designated under the statute to perform emergency psychiatric examinations (
5,
6). Designated receiving facilities may be located in general hospitals with psychiatric units, in psychiatric hospitals, or in community mental health centers with inpatient capacity. The examinations can be initiated by selected mental health professionals, law enforcement officials, or judges and authorize receiving facilities to hold individuals involuntarily for up to 72 hours for examination and treatment. After 72 hours, the individual must be released or a petition for court-ordered involuntary treatment must be filed with the court, which, when granted, authorizes local treatment facilities or state hospitals to treat the patient on an involuntary basis for up to six months.
Individuals with serious mental illness and criminal justice involvement tend to have high rates of involuntary examinations. For example, in a study of arrestees in Pinellas County, Florida, 44% of those with a serious mental illness had experienced an involuntary examination over the four-year study period from 2002 to 2006 (
7). We do not know from this prior study, however, what the temporal relationship is between involuntary examinations and arrests. The purpose of this study was to use individual fixed-effects models to examine the association between the occurrence of an involuntary examination and the risk of arrest during the next quarter. Individual fixed-effects models were used to examine the timing of events and whether an examination signaled that an individual was at risk of arrest in the near future.
Methods
This project was approved by the University of South Florida Institutional Review Board.
Data
The Pinellas County Criminal Justice Information System contains information for all individuals incarcerated in the Pinellas County jail and was used to identify all adults less than 65 years of age who were in the Pinellas County jail during the 2003–2004 period. The Pinellas County Criminal Justice Information System did not contain diagnostic information for arrestees. Therefore, to determine which arrestees had a serious mental illness, we accessed and linked a number of statewide and county-specific service event data sets, which identified and described all individuals who had received publicly funded mental health services and supports in the county during the four-year study period. The statewide data sets included Medicaid claims and the service event data set maintained by the State Mental Health and Substance Abuse Authority.
In addition, statewide data on the occurrence and timing of involuntary examinations were obtained. We used county-specific data sets that included systems documenting health and social services, homeless services, and emergency medical services paid for by the county. The merging of the statewide and the county-specific services data sets produced a list of all individuals who received a publicly funded service in the county during the four-year period and who had a serious mental illness diagnosis in one of the databases. DSM-IV diagnoses used as indicators of serious mental illness included schizophrenia (code 295), schizoaffective disorder (295.7), delusional disorders (297.1), other psychotic disorders (293.81 and 293.82), bipolar I disorder (296), major depressive disorder (296.3), and other bipolar and mood disorders (296.90). When more than one diagnosis appeared, the most frequently occurring diagnosis was used.
Using these data and statewide arrest records between July 1, 2002, and June 10, 2006, we identified for the sample all arrests; involuntary examinations; and mental health emergency room, inpatient, and outpatient contacts. Mental health services were defined on the basis of the primary diagnosis and procedure codes. Given that most involuntary examinations are performed on an inpatient basis, an inpatient stay or emergency room visit was counted only if it was not associated with an involuntary examination. We divided the period between July 1, 2002, and June 10, 2006, into 16 periods of 90 days and aggregated all arrest, service, and involuntary examination events into one of these periods on the basis of the dates they occurred.
These data have been used in prior research to assess the relationship between individual characteristics and arrests (
7) and public sector expenditures (
8). Arrests were more common among individuals who were younger, male, or homeless or who had a diagnosed substance use disorder, involuntary examination, or psychiatric inpatient stay. Arrests were less common among blacks (relative to whites) and among those receiving outpatient mental health treatment. However, these studies were cross-sectional analyses and thus did not focus on the timing of events.
Analysis
Descriptive statistics examined arrest rates for two groups of individuals: those who did not have an involuntary examination during the sample period and those that had an involuntary examination during the sample period. For those who had an examination, arrest rates were examined for quarters preceded by an examination and for quarters that were not preceded by an examination. Statistical significance in arrest rates was assessed with generalized estimating equations (PROC GENMOD in SAS) to account for the repeated observations for each individual.
Given that the purpose of this study was to examine the temporal relationship between an involuntary examination and the risk of arrest, within-person models were used to examine the relationship between receiving an involuntary examination in one quarter and the risk of arrest in the next quarter. Within-person models included individual-specific intercepts in the regression specification that could be estimated as random effects or as nonrandom fixed effects. The individual-specific intercepts control for the effects of time-invariant individual characteristics that are observed (gender, race) or unobserved in administrative data. Examples of potentially relevant unobserved characteristics that may be time invariant include antisocial attitudes, antisocial cognition, weak self-control, and IQ. Random effects models are more efficient than nonrandom fixed-effects models when the unobserved differences across individuals are uncorrelated with the included explanatory variables. However, the Hausman test indicated that the unobserved individual factors were correlated with the explanatory variables (
9). Consequently, individual fixed-effects models were used to assess the relationship between involuntary examinations and arrests.
Generalized estimating equations using Poisson regression (arrests are count data that are not normally distributed) were used to estimate the associations between the independent and dependent variables for each person across time: Arrestsi,t+1=Xitβ+µi+Qtα+ϵit, where X contains time-varying variables including a categorical variable denoting an involuntary examination in period t, µi denotes the individual-specific intercepts, and Q is a vector of categorical variables denoting each of the quarters. Given that we examined arrests in the next quarter, the 16 quarters of data provided up to 15 quarterly observations for each person. The within-person model was used to determine whether quarters with an involuntary examination were more likely to be followed by an arrest in the next quarter than quarters without an involuntary examination. Three different regression specifications were estimated with the dependent variable denoting the number of arrests, felony arrests, and misdemeanor arrests. In addition, the regressions were estimated for the entire sample and for a restricted sample that included only individuals who experienced an involuntary examination at least once during the four years.
Several important variables were not available on a time-varying basis. For example, we knew whether a person was homeless at some point in the four years, but we did not know the exact dates. In addition, each individual was assigned a single mental health diagnosis. Similarly, we defined substance dependence or abuse on the basis of whether a person received such a diagnosis at some point in the four years. This decision was made because substance use may occur for long periods before and after a diagnosis. In addition, Florida Medicaid outpatient claims contain only a single diagnosis, making the analysis of comorbid diagnoses challenging. Although age varies over time, we did not include it in the specification because it of course changed by the same amount for each person in each quarter.
Given that an individual must be in the community (that is, not incarcerated) to be arrested or subject to an involuntary examination, individuals were required to be in the community for at least 45 days in period t to provide sufficient opportunity for an involuntary examination to occur, and at least one day in period t+1 for an arrest to occur. Thus the individual could not be incarcerated a majority of the base period or for the entire follow-up quarter. We explored different cutoffs (0, 15, and 30 days) for period t and also removed all minimum time requirements, but the results were invariant to this decision.
Results
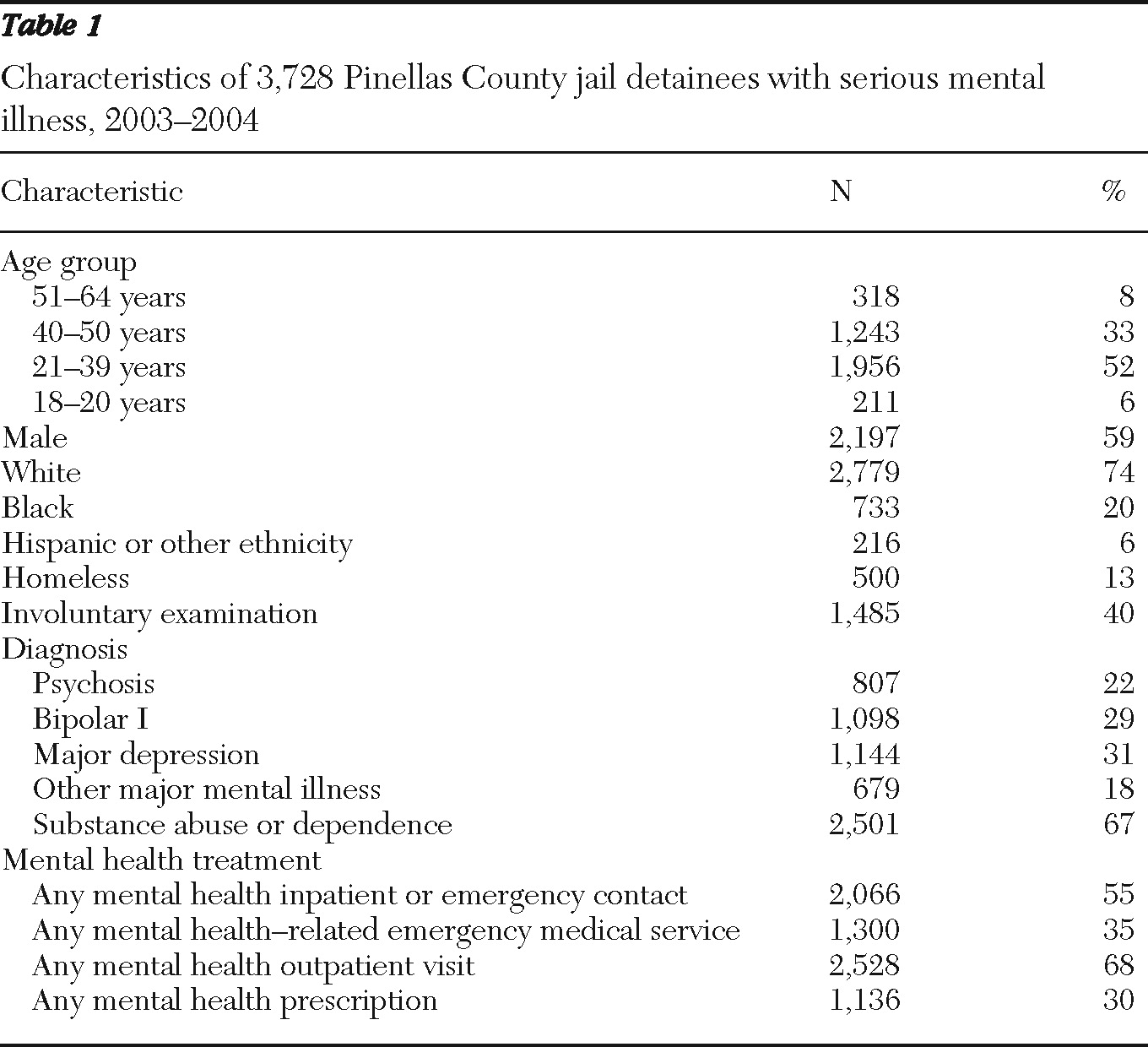
A total of 3,728 persons with a serious mental illness diagnosis were identified in the Pinellas County jail population, which represented 10% of all arrestees for the period between July 1, 2003, and June 30, 2004.
Table 1 contains descriptive statistics for the sample. Persons included in the study were on average 36±10 years of age and were predominantly male and white. The most common mental illness diagnoses were bipolar I disorder (29%), major depressive disorder (31%), and psychotic disorders (22%). Sixty-seven percent had a substance dependence or abuse diagnosis; 40% experienced one or more involuntary psychiatric examinations, and 13% experienced homelessness at some time during the study period. With respect to contacts with the mental health treatment system, 68% had one or more outpatient mental health contacts, 55% had at least one emergency room or inpatient mental health contact, and 30% received prescription medications as indicated by Medicaid claims, although the actual number of individuals receiving prescription medications was undoubtedly higher. Thirty-five percent of individuals had contact with emergency medical services.
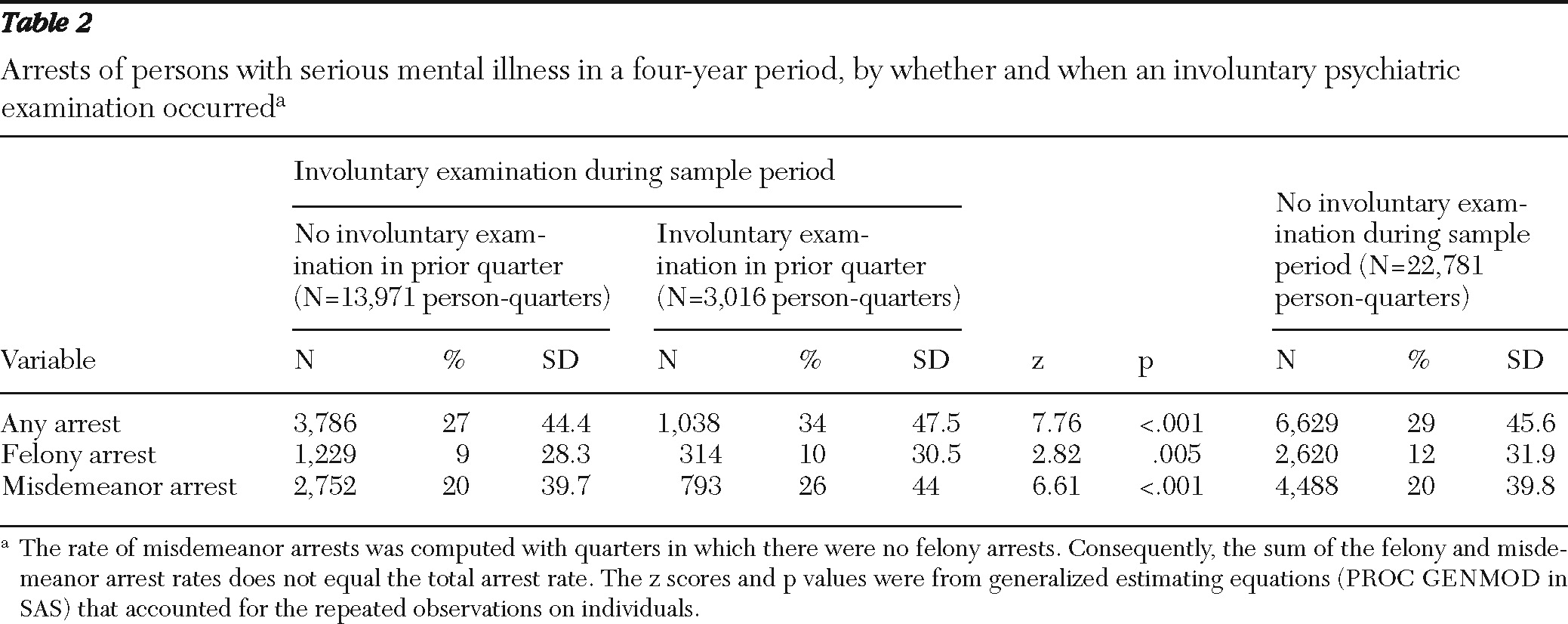
Table 2 presents data on the sample's criminal justice contacts, according to whether persons had an involuntary examination at any time during the entire four-year period. Individuals who did not experience an involuntary examination during the four years experienced an arrest in 29% of the quarters and a felony arrest in 12% of the quarters. Among individuals who had an involuntary examination at some point during the four years, we separated arrests in quarters after an examination from arrests in quarters that were not preceded by an examination. Arrest rates were higher (34%) in quarters that followed an involuntary examination compared with quarters that were not preceded by an examination (27%) (z=7.76, p<.001). Rates of felony arrests and misdemeanor arrests were both higher in quarters after an involuntary examination (z=2.82, p=.005; z=6.61, p<.001).
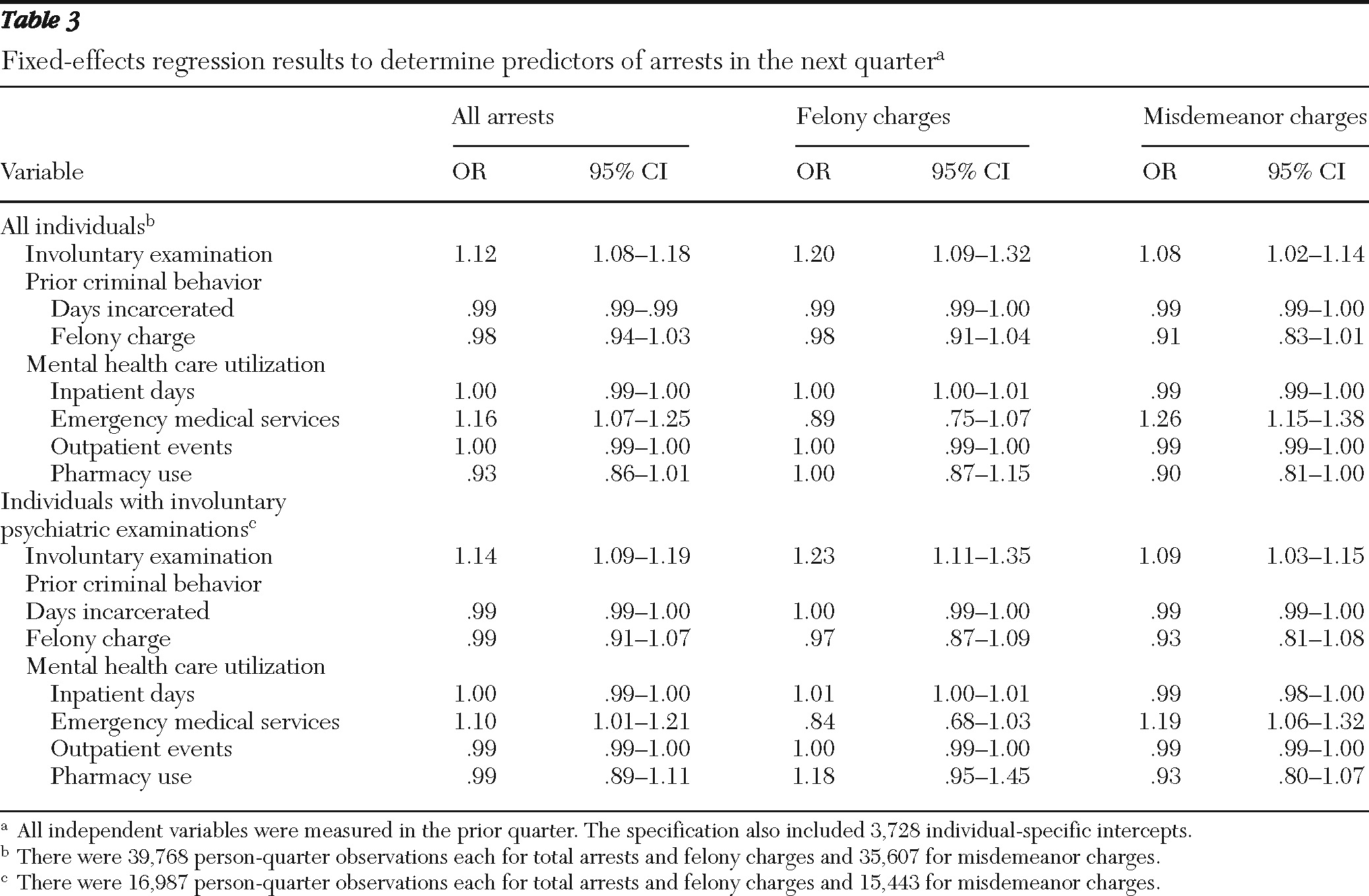
The fixed-effects regression results are provided in
Table 3. There was a significant positive relationship between the receipt of an involuntary examination in one period and the likelihood of arrest in the next period. For the full sample, the association was found for total arrests (odds ratio [OR]=1.12), felony arrests (OR=1.20), and misdemeanor arrests (OR=1.08).
Among the other findings for the full sample, individuals who spent more days incarcerated in one quarter were less likely to be arrested in the next quarter. Use of emergency medical services was associated with an increased risk of misdemeanor arrest, and a greater number of inpatient days were associated with an increased risk of felony arrest in the next quarter.
The restricted sample of individuals who experienced at least one involuntary examination had similar results for the association between involuntary examinations and likelihood of arrest. The likelihood was greater for total arrests (OR=1.14), felony arrests (OR=1.23), and misdemeanor arrests (OR=1.09) in quarters after an involuntary examination.
For people released after examination rather than committed for a longer period, the goal is stabilization and linking the individual to community treatment. Consequently, individuals with an involuntary examination should exhibit an increased rate of outpatient contacts in the next quarter. Indeed, an involuntary examination was associated with an increased likelihood of outpatient contacts in the next quarter (results not reported in table) for the full sample (OR=1.22, CI=1.10–1.35) and the restricted sample (OR=1.21, CI=1.09–1.35).
Discussion
We found that involuntary examinations under Florida's civil commitment law in one quarter of a year were associated with risk of arrest in the next quarter. Each involuntary examination was associated with a 12% increase in the risk of arrest, with a greater increase for felony arrests (20%) than misdemeanor arrests (8%). Thus an involuntary examination appears to be a signal for behavior considered serious (not simply nuisance crimes) by criminal justice officials.
The results are striking for several reasons. Most important, involuntary civil commitment is designed to achieve both therapeutic and public safety outcomes. Our data, showing that use of the emergency examination provision of Florida's involuntary civil commitment statute is associated instead with an increased risk of arrest, suggest that the principal aims of civil commitment are not being met.
Outpatient contacts are more likely in the quarter after an involuntary examination, and in theory, outpatient contacts should also be associated with lower arrest rates. However, our finding of a low association between outpatient services and arrests in the next quarter is consistent with the very mixed findings in the literature regarding whether mental health treatment is associated with a reduction in arrests (
10). Indeed, some types of routinely available mental health services may actually increase arrests for technical violations, although that may be the case due to increased oversight of the individual (
11). It also has been suggested that the services can be ineffective because they are the wrong kind (
7) or the wrong frequency (
12) or both.
Establishing whether there is a relationship between involuntary examinations and risk of arrest has other policy implications. Some have suggested that certain services, such as forensic assertive community treatment, can lead to reduced arrest rates of individuals with serious mental illness (
13). Others have concluded that mandated outpatient treatment has been effective at reducing criminal justice involvement (
14), for at least some individuals, and may be an alternative to inpatient placement for some individuals. Should such services be targeted more specifically to individuals who are held for involuntary psychiatric examination?
It has also been suggested that involuntary civil commitment as a vehicle for obtaining long-term inpatient care has largely been abandoned because of changes in financing, length of psychiatric hospital stays, and related reasons (
15). If that is true in even some jurisdictions, then the fundamental assumptions that civil commitment serves both therapeutic and public safety goals may need reexamination. It may be inadequate to think of diversion from only the criminal justice system; it may become necessary to think about diverting people from interventions historically thought to be therapeutic as well. Interestingly, mental health inpatient and emergency room contacts not associated with the involuntary examination were not strongly related to the risk of arrest. Involuntary psychiatric examinations are almost always done on an inpatient basis. Whereas the involuntary examination was associated with a risk of arrest in the next quarter, voluntary inpatient treatment was only weakly related to the risk of felony arrests and not significantly associated with misdemeanor arrests. Future research should consider why different types of inpatient treatment are associated with different outcomes.
To be clear, we do not propose a causal link between involuntary examinations and arrests. Rather, the event of an involuntary examination seemed to be a signal that the person was at increased risk of arrest. In addition, our sample comprised individuals with serious mental illness, and although most people who receive an involuntary examination have a serious mental illness, the results should not be generalized to all individuals who are subject to involuntary examination.
Several additional analyses were performed as sensitivity checks. We replaced the continuous involuntary examinations variable with categorical variables denoting one involuntary examination, two examinations, and so forth to assess whether multiple involuntary examinations had a larger effect on the risk of arrest than a single examination. The estimated coefficients were consistent with a positive association between the number of examinations and the risk of arrest. We also included a series of interactions between the time-varying variables in the regression and the time-invariant variables. None of the coefficients approached statistical significance.
As with any study using administrative data, this study had several limitations. First, the sample was selected from a jail population, and thus the results cannot be generalized to all individuals with a serious mental illness. For example, future research should examine whether an involuntary examination is a signal for people prone to criminal behavior but not for other individuals. On the other hand, people in the community may represent a healthier sample than those incarcerated or committed to psychiatric hospitals for long periods. Second, the involuntary examination data do not contain information on the outcome of the assessment. Thus we do not know whether the individual was released to the community or was committed for further treatment. However, people with an involuntary examination who are committed for further treatment would have limited opportunity for arrest. Consequently, the results reported in the article may be conservative estimates.
Conclusions
Involuntary examinations are associated with increased risk of arrest. Thus an involuntary examination is a significant signal that individuals with serious mental illness are at risk of arrest.
Acknowledgments and disclosures
Funding for this study was provided by Ortho-McNeill Janssen LLC.
The authors report no competing interests.