Nelson et al. (
3) have proposed that the activation of a word may be modulated by both the size and the degree of connectivity of its network. Consider the example provided by Nelson and colleagues of the words “dog” and “dinner.” Each has five associates, which include “cat,” “puppy,” “animal,” “house,” and “friend” for “dog,” and “supper,” “eat,” “lunch,” “food,” and “meal” for “dinner.” However, Nelson et al. have also shown that among the five associates of “dog,” only one associate (animal) is connected to another associate (cat). By contrast, “dinner” has been shown to have 17 connections among its associates.
Using a connectionist framework, Nelson et al. (
3) developed a word recall paradigm to isolate the effects of network size and connectivity on associative memory in healthy subjects. As shown in
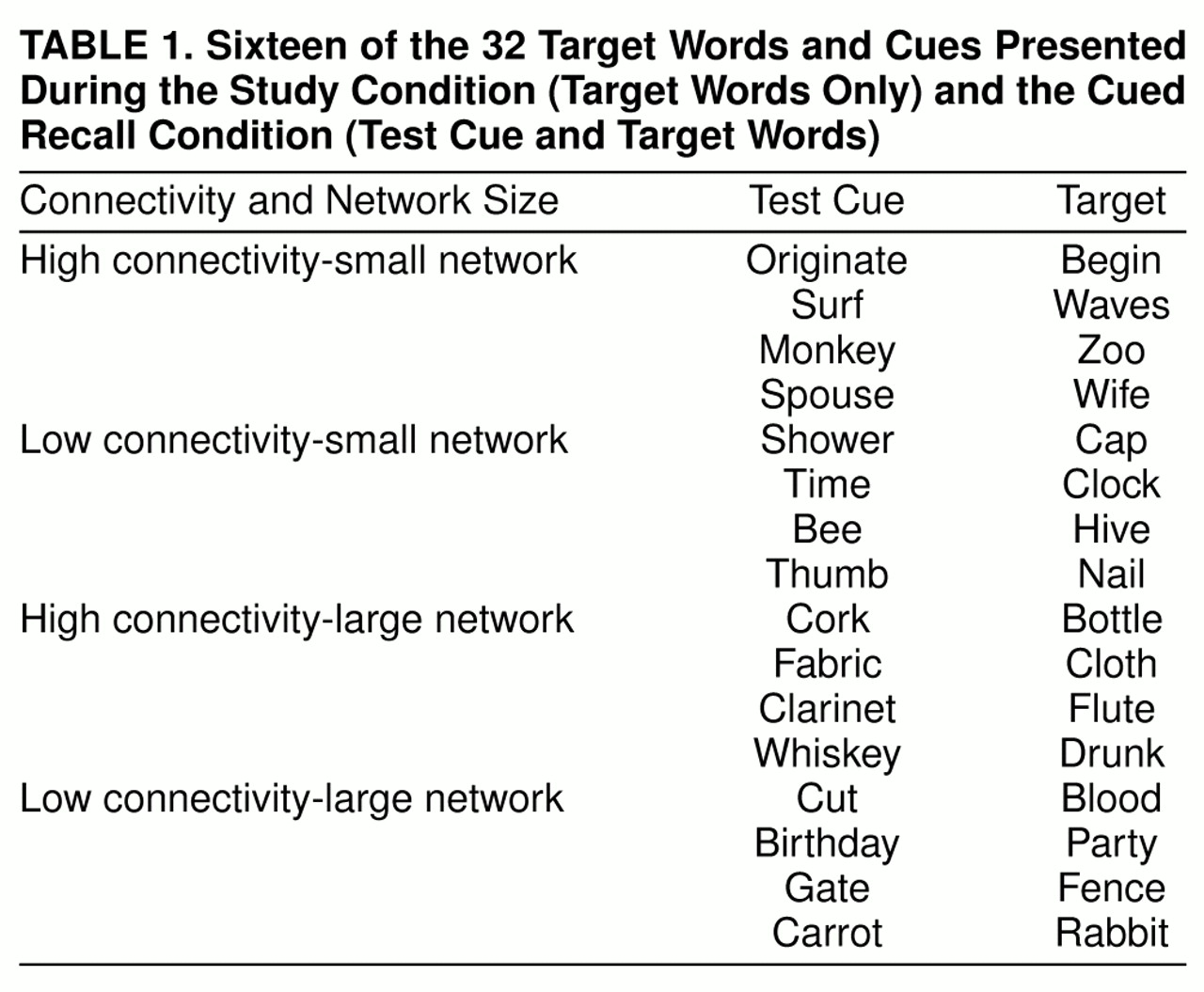
table 1, the paradigm consisted of four types of words: 1) high connectivity-small network (e.g., waves, wife, zoo), 2) low connectivity-small network (e.g., cap, clock, hive), 3) high connectivity-large network (e.g., bottle, cloth, flute), and 4) low connectivity-large network (e.g., blood, party, rabbit). Subjects first study a list of words consisting of equal proportions of these four types, followed by a cued recall test in which word cues and targets are equated on both connectivity and network size. In several carefully controlled experiments, Nelson and colleagues have consistently found support for their model: words of small networks are easier to recall than words of large networks, and words of high connectivity are easier to recall than words of low connectivity. In addition, for single-trial cued recall, performance is best for words of high connectivity-small network (e.g., wife cued by spouse), followed by low connectivity-small network (e.g., clock cued by time), then by high connectivity-large network (e.g., bottle cued by cork), and last by low connectivity-large network (e.g., party cued by birthday).
METHOD
Eighteen male schizophrenic patients and 21 normal comparison subjects participated in the study. All subjects were between the ages of 20 and 65 years, were native speakers of English, and were without histories of ECT, neurological illness, or a DSM-III-R diagnosis of drug or alcohol abuse. DSM-III-R diagnoses of schizophrenia were ascertained on the basis of the Structured Clinical Interview for DSM-III-R—Patient Version (
6) and medical chart review. All patients were receiving neuroleptic medication; the mean daily dose was 555 mg (SD=455) of chlorpromazine equivalents. The mean duration of illness was 23.2 years (SD=10.2). Positive and Negative Syndrome Scale scores (
7) were available for 14 of the 18 patients. Ten of the patients met the criteria for negative subtype, and four for positive subtype. The normal comparison subjects were recruited from newspaper advertisements and were matched to the patients on the basis of age, sex, and handedness. Potential comparison subjects were excluded if they had a personal or family history of mental illness. Mean age did not differ significantly between the comparison group (39.9 years, SD=11.4) and the patient group (44 years, SD=9.5). After complete description of the study to the subjects, written informed consent was obtained.
The words used in this experiment were identical to those used by Nelson et al. (
3), who have established norms for more than 2,000 words over the course of 15 years of research. These norms provide an empirical basis for rating words on both connectivity and network size. On the basis of these norms, Nelson and colleagues reported that connectivity averaged 2.50 for words of high connectivity and 0.89 for words of low connectivity. They also reported that the mean number of associates was 6.75 for words of small network size and 21.46 for words of large network size. In addition, Nelson and colleagues have provided lists of target words and cues consisting of equal proportions of words reflecting 1) high connectivity-small network, 2) low connectivity-small network, 3) high connectivity-large network, and 4) low connectivity-large network. Both frequency and concreteness have been equated across these four types of words (
3).
Table 1 provides examples of each of the four types of target words and cues used in the current study.
The subjects were tested individually; they were presented with single words typed in uppercase letters, one at a time for 3 seconds, on laminated index cards. To familiarize the subject with the rate of presentation, a short list of names was first presented one at a time. A study list of 32 to-be-remembered target words was then presented, and the subject read each word aloud. Immediately after the subject studied these words, a cued recall test was administered, again following the procedures of Nelson and colleagues.
Table 1 lists 16 of the 32 target words and cues used for the cued recall test. For example, the word “originate” cued recall of the high connectivity-small network target word “begin”; the word “shower” cued recall of the low connectivity-small network target word “cap”; the word “cork” cued recall of the high connectivity-large network target word “bottle”; and the word “cut” cued recall of the low connectivity-large network target word “blood.” Two additional trials of study-cued recall in which the identical words and cues were used were presented, for a total of three trials.
RESULTS
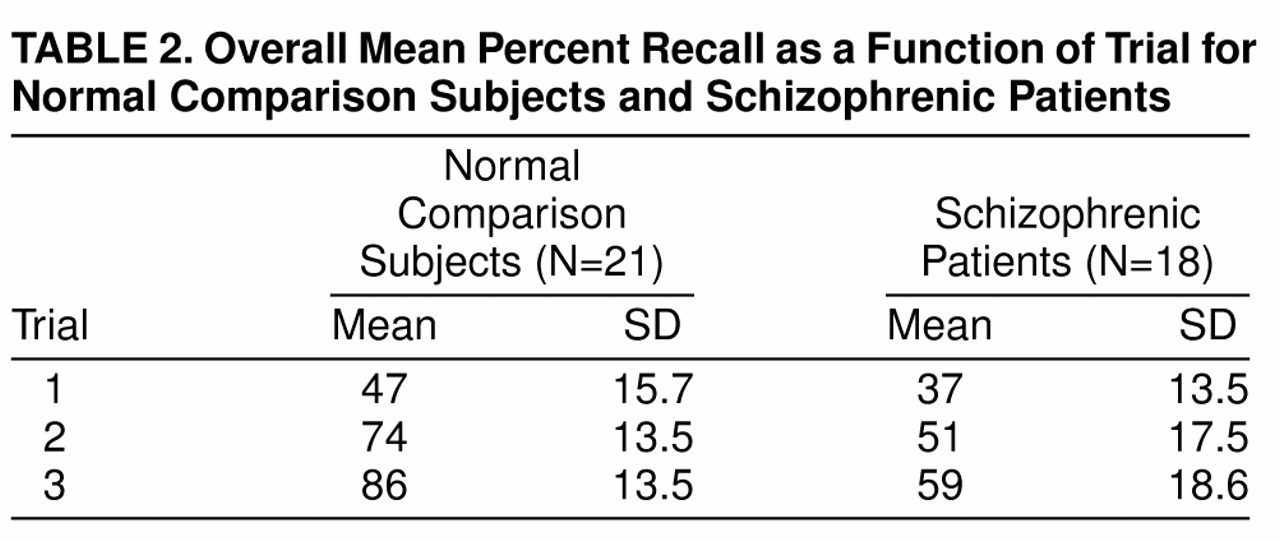
Recall rates for each of the three trials are shown in
table 2. A repeated measures analysis of variance (ANOVA) revealed highly significant effects for group (F=18.95, df=1, 37, p<0.001) and trial (F=195.90, df=2, 74, p<0.001) and for the interaction between group and trial (F=16.01, df=2, 74, p<0.001). The comparison subjects had a mean recall rate of 69%, in contrast to 49% for the schizophrenic patients. As can be seen in
table 2, the significant interaction reflected a greater rate of improvement in recall over the three trials for the comparison subjects in relation to the patients with schizophrenia: the comparison subjects showed a 39% rate of improvement, and the schizophrenic patients 22%.
Repeated measures ANOVA was also used to analyze recall rates for each of the four types of words collapsed over trials. ANOVA revealed highly significant effects for group (F=18.95, df=1, 37, p<0.001), network size (F=20.49, df=1, 37, p<0.001), and connectivity (F=21.39, df=1, 37, p<0.001). These statistically significant effects for word connectivity and word network size indicated that recall did vary as a function of these manipulations. More important, however, the repeated measures ANOVA revealed a significant interaction between connectivity and group (F=8.68, df=1, 37, p<0.02). In relation to the comparison subjects, the patients with schizophrenia not only showed a significant reduction in recall but also exhibited a different pattern of recall as a function of connectivity of the to-be-remembered words.
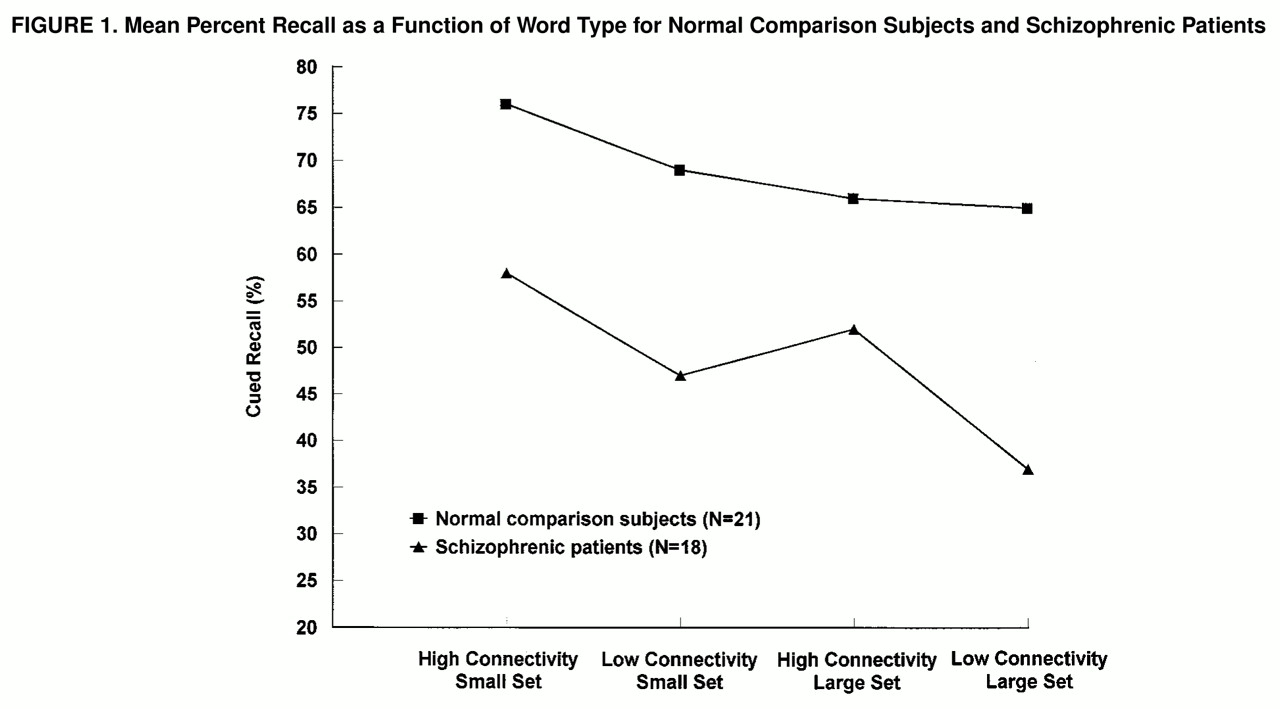
As displayed in
figure 1, comparison subjects showed the expected effects for both connectivity and network size. Their highest rates of recall were for words of high connectivity-small network size, followed by words of low connectivity-small network size, then by words of high connectivity-large network size, and finally by words of low connectivity-large network size. Schizophrenic patients also had their highest and lowest recall rates for high connectivity-small network size words and low connectivity-large network size words, respectively. However, in contrast to the comparison subjects, the schizophrenic patients recalled more words of high connectivity-large network size than words of low connectivity-small network size. For the comparison subjects, the mean recall was 69% for words of low connectivity-small network size and 66% for words of high connectivity-large network size. For the schizophrenic patients, the mean recall was 47% for words of low connectivity-small network size and 52% for words of high connectivity-large network size.
To isolate further the effects of connectivity and set size, we computed the following indexes. For connectivity (collapsed over network size), percent recall of low connectivity words was subtracted from that of high connectivity words. For network size (collapsed over connectivity), percent recall of large network words was subtracted from that of small network words. Low connectivity reduced recall by 4% in the comparison subjects and by 13% in the schizophrenic patients (t=2.95, df=37, p<0.01). By contrast, large network size had a similar effect for both groups, reducing recall by 7% in the comparison subjects and by 8% in the schizophrenic patients.
DISCUSSION
This study used a cued-recall word paradigm generated from a connectionist framework to attempt to identify the cognitive dynamics underlying schizophrenic associative disturbance. The results indicate that schizophrenic patients showed overall reduced recall in relation to normal comparison subjects. The schizophrenic patients also showed a different pattern of recall as a function of word type; that is, the comparison subjects showed the expected effects for both connectivity and network size, as they recalled more words with high connectivity than words with low connectivity and more words with small networks of associates than words with large networks of associates. The schizophrenic patients also recalled more words of small networks than words of large networks. However, as reflected by the statistically significant interaction of connectivity and group, the patients showed a pronounced effect of connectivity: recall improved substantially for words of high connectivity and declined dramatically for words of low connectivity.
These results demonstrate that the connectivity and the size of the networks of the to-be-remembered words exerted different effects on recall in patients with schizophrenia in relation to comparison subjects. The two groups showed similar effects of network size, recalling more words of small networks than words of large networks. This indicates that for both groups, the number of associates of a given word had a similar influence on recall of that word. Thus, the overall decline in recall by patients with schizophrenia could not be attributed to a decay or loss of associates. By contrast, however, the data point to a fairly selective connectivity effect for patients with schizophrenia; network connectivity significantly affected recall for these patients. For example, whereas comparison subjects recalled more words of low connectivity-small network size than words of high connectivity-large network size, patients with schizophrenia showed the opposite pattern, recalling more words of high connectivity-large network size than words of low connectivity-small network size.
This pattern of findings suggests an overactivation of strongly connected networks and an underactivation of weakly connected networks in schizophrenic patients. For patients with schizophrenia, recall may thus be dominated by network connectivity at the expense of other critical contextual factors. This might explain some of the associative intrusions that are often characteristic of schizophrenic discourse, as in the famous example of Bleuler’s patient, mentioned earlier, for whom the highly activated and perhaps dominant but irrelevant associate of “family” (Holy Ghost) entered into consciousness. Similarly, other experimental findings (
8) have demonstrated that schizophrenic patients tend to respond to the strongest associate of a word, regardless of context (e.g., pen as writing instrument even though the context suggests a fence). More recently, the enhanced priming effect demonstrated in several (
9–
11), albeit not all (
12), word priming studies in patients with schizophrenia may also reflect an overactivation of dominant associates of words.
The foregoing emphasizes that a key element of any network, whether it is cognitive, computational, or biological, is its ability to maintain stability and to manage excitation (
13). For cognition, a word produces various levels of excitatory buildup, as reflected by competition among simultaneously activated representations (
14). For patients, schizophrenia may produce a dysregulation of network excitation, resulting in aberrant activation and instability (
15). Such a failure to maintain stability within an activation-based network may lead not only to intrusions of highly active irrelevant representations into consciousness but also to an overall weakening of associations, as reflected by impoverished thinking.
Connectionist models often include artificial neural networks to simulate behavioral or cognitive effects of various brain disorders (
16). In its simplest form, an artificial neural network is composed of units (i.e., input, hidden, output) and links that serve to connect these units. Network size is described as the number of units, and the degree of connectivity of these units is described as their weight. An important consideration is how well a computational model represents a cognitive disturbance. For example, recent simulations of the cognitive deterioration in Alzheimer’s disease (
16) randomly chose and removed connections affecting both functional and perceptual features while sparing connections directly supporting phonologic computations. These manipulations produced a gradual decay in semantic memory that provided a reasonable representation of some of the observed cognitive changes associated with Alzheimer’s disease.
We did not design the current study to provide a computer simulation of the observed reduced recall by schizophrenic patients. However, the observed behavioral findings did provide some clear directions for the focus of future computational simulations. The empirical findings reflect schizophrenic patients’ reduced performance on cued recall of words that differed in both the size and the degree of connectivity of their networks. These findings in turn suggest that the differences in recall between groups may be attributable to the effects of abnormal connectivity but not network size in patients with schizophrenia. Thus, these observed behavioral findings may lead to simulations that incorporate network anomalies in connection weights while holding constant the number of units representing network size. Such modeling may represent a reasonable first-step approximation of the reduced recall by the patients in the present study. It may also represent a promising analogy to the current behavioral finding suggesting that perhaps a disease-related modulatory failure of associative links is central to schizophrenic cognitive disturbance.
If schizophrenia represents a dysregulation of connections that bind associates within local networks, an important question is where these networks might be distributed within the brain. In healthy subjects, neuroimaging studies have demonstrated that various dimensions of words produce differential patterns of brain activation (
17–
19). For example, semantic categories (animals or tools) and syntactic categories (verbs or nouns) produce differential activity within specific brain regions of the left temporal lobe (
17). Similarly, emotional words (e.g., sex, murder, sadness) have been shown to activate orbital frontal and limbic structures (
18). Even more relevant are findings of a recent study (
19) which demonstrated that the degree of associative strength of word pairs produces bilateral frontal activity, which increases as the associative strength of the word pairs decreases. Taken together, these studies have demonstrated that these patterns of elicited brain activity are primarily confined to frontal and temporal lobe structures, and such findings have been cited as evidence for a brain dictionary or lexicon that is critically dependent on the integrity of these regions (
5).
The effect of abnormal connectivity observed in schizophrenic patients may therefore represent neuropsychological evidence of a functional disturbance in the lexicon of the frontal and temporal lobes. This observation is supported by other lines of evidence, such as neurophysiological studies (
20,
21) demonstrating schizophrenic subjects’ abnormalities in the semantically sensitive event-related potential N400, which is thought to depend largely on left temporal lobe generators (
22). In addition, magnetic resonance imaging (MRI) studies of schizophrenic patients have revealed volumetric reductions in the areas of the frontal and temporal lobes that are often intimately associated with the lexicon (
23,
24). These structural abnormalities have in turn been correlated with specific patterns of neuropsychological impairments. For example, reduced temporal lobe volumes have been correlated with severity of thought disorder and neuropsychological deficits in associative memory and categorization (
25). By contrast, on MRI reduced frontal lobe volumes of schizophrenic subjects have been associated with reduced performance on neuropsychological tests of attention and working memory (
26). However, the current study provided no direct empirical evidence to address the nature of the underlying disease-related brain disturbance that presumably accounts for the abnormal connectivity effect that we observed in the patients. Nor did the study examine the relation between the patients’ overall level of neuropsychological functioning and the abnormal connectivity effect that was evident on the list of words used in the experiment.
In summary, the current experiment represents one of the first studies to apply a connectionist framework to examine the cognitive dynamics of schizophrenia. We examined cued word recall by using a connectionist paradigm that manipulated two dimensions of the to-be-remembered words, connectivity and network size. These variables were selected not only because they may be related to important properties of neuronal networks but also because they may be highly amenable to computational simulations. The results revealed effects of abnormal connectivity but not network size in patients with schizophrenia. These behavioral data suggest that the most realistic simulations of schizophrenic associative disturbance may be the ones which selectively manipulate connection weights that serve to modulate associative links. Thus, these findings may provide an empirical and computational direction for simulating the well-known schizophrenic disturbance in associations, first described by Bleuler as a hallmark of the disorder.