For the past three decades the mainstay of pharmacological treatment of schizophrenia was the “typical” neuroleptics, which were predominantly dopamine D
2 receptor blockers. These drugs were effective in controlling positive symptoms but had only a partial effect on the negative symptoms and cognitive dysfunction of schizophrenia. Furthermore, because of their prominent blockade of the dopamine D
2 receptors, these drugs are associated with a high prevalence of acute extrapyramidal side effects as well as tardive dyskinesia, and they elevate prolactin levels, leading to sexual and endocrine side effects. The introduction of clozapine radically changed thinking about the mechanism of action of antipsychotics. Clozapine is a weak blocker of the dopamine D
2 receptor and shows significantly more affinity for a range of receptors, especially the serotonin 5-HT
2 receptor. At a clinical level, clozapine shows a superior efficacy on negative symptoms and is practically free of extrapyramidal side effects, tardive dyskinesia, and prolactin elevation. Thus, clozapine has served as a template for the development of the next generation of “atypical” antipsychotics (e.g., risperidone, olanzapine, sertindole, and quetiapine). While the precise mechanism of the atypicality of clozapine is unclear, one prominent hypothesis implicates its high affinity for the 5-HT
2 receptor, combined with its low affinity for the dopamine D
2 receptor (
1–
4).
Olanzapine, another newly marketed atypical antipsychotic, is chemically similar to clozapine and shares several aspects of clozapine's in vitro pharmacological profile (stronger affinities for the 5-HT
2, muscarinic, and histaminic receptors than for the dopamine D
2 receptor) (
12). These pharmacological characteristics translate into clozapine-like clinical benefits: substantially reduced extrapyramidal side effects, less effect on prolactin, and probably a direct effect on ameliorating negative symptoms (
13–
16). These clinical studies suggest that the optimal dose for olanzapine may be between 10 and 20 mg/day. Therefore, it is of clinical and scientific interest to determine olanzapine's in vivo receptor occupancy profile in patients at clinically relevant doses. In particular, we asked 1) Does olanzapine (like clozapine and risperidone) have a potent effect on 5-HT
2 receptors? 2) What is olanzapine's D
2 occupancy in its effective dose range? 3) Does olanzapine (like clozapine and risperidone) have a greater effect on the 5-HT
2 as opposed to the D
2 receptors? 4) At what doses, if any, does olanzapine demonstrate greater than 80% D
2 occupancy? 5) If its D
2 occupancy does go beyond 80%, what implication does this have for prolactin levels and extrapyramidal side effects?
METHOD
This study was approved by the Human Subjects Review Committee of the University of Toronto. Patients participated after receiving detailed information about the study and signing a written consent document. Male and female patients were included if they were between the ages of 18 and 45 years and met DSM-IV criteria for a diagnosis of schizophrenia. Patients were excluded from participation if they suffered from a major medical or neurological illness, if they met DSM-IV criteria for substance abuse in the last 3 months, if they had received a depot antipsychotic medication in the last 6 months, or if they were receiving a concomitant psychotropic medication (benzodiazepine and antiparkinsonian agents were administered).
The study was designed to obtain PET data on three subjects in each of the four dose groups, 5 mg/day, 10 mg/day, 15 mg/day, and 20 mg/day, by random assignment. Three subjects dropped out before the PET scan and were replaced by random assignment. In addition to these data, three scans were obtained for three patients receiving treatment with 30, 30, and 40 mg/day of olanzapine, respectively. Two of these scans were for individuals who had participated in the study and did not show a satisfactory response at their assigned dose, and the third scan was for an individual receiving clinical treatment with 30 mg/day.
Patients enrolled in the study went through a washout period from their previous neuroleptic that lasted 2–4 days, and medication was then titrated to their assigned dose. Patients assigned to 5 and 10 mg/day started with these doses. Those assigned to 15 and 20 mg/day were started at 10 mg/day, and their dose was increased in weekly increments of 5 mg/day. Patients were held at their assigned target dose until steady-state levels were achieved (5 days or greater), at which stage PET scans were done. Two of the patients were neuroleptic naive, another two had not had any neuroleptic for more than 6 months, and the rest had at least a 14-day washout from their previous neuroleptic at the time of PET scanning during olanzapine treatment. The D
2 occupancy was assessed by using [
11C]raclopride, 12 hours after the last dose, while the 5-HT
2 occupancy was assessed on the same day 2–3 hours after the D
2 PET scan (14–15 hours after the last dose). After the PET scan the patients reverted to a flexible-dosing, open clinical treatment and were followed for a maximum of 8 weeks. To determine their clinical status, each of the patients was rated with the Positive and Negative Syndrome Scale (
19) and a Positive and Negative Syndrome Scale-derived Brief Psychiatric Rating Scale (
20) at baseline, at the time of the PET scan, and at end of their participation in the open clinical phase. At these times, extrapyramidal side effects were assessed with the Barnes Akathisia Scale (
21) and the Simpson Angus Rating Scale (
22).
The PET scans to estimate D
2 occupancy were obtained after the injection of 10 mCi of high-specific-activity [
11C]raclopride (300–1600 Ci/mmol), through use of a bolus plus infusion protocol. The methods employed here are identical to those described in previous reports in this journal (
7). The pertinent aspects are the following: striatal and cerebellar regions of interest were drawn on two contiguous PET slices on a composite PET image with reference to an MRI scan (General Electric Signa 1.5-T scanner, T
2-weighted spin-echo sequence) coregistered to the PET scan by using a surface-matching algorithm as implemented in ANALYZE 7.0 (Biomedical Imaging Resource, Rochester, Minn.). An estimate of binding potential of raclopride (D
2BP) (which represents the B
max/K
d of [
11C]~raclopride for D
2 receptors; where B
max is the total number of receptors available to a ligand and K
d the affinity of the ligand for the receptors) was obtained from the ratio of the striatum to the cerebellum. As used in our laboratory, this method yields a test-retest standard deviation of 6% and has been standardized to have a high interrater and intrarater reliability (intraclass correlation coefficient [ICC] greater than 0.95).
To estimate receptor occupancy, we used an age-corrected baseline derived from a pool of 16 normal control subjects and 12 neuroleptic-naive patients with schizophrenia. Since the illness has no statistically discernible effect on D
2 receptors as measured with [
11C]raclopride (
23), the data from neuroleptic-naive patients and control subjects were pooled to get a better estimate of the effect of age on D
2BP (F=0.66, df=1,25, p=0.42). Olanzapine-induced D
2 receptor occupancy was determined as (D
2BP
Bas–D
2BP
Olz)/(D
2BP
Bas), where D
2BP
Bas is the age-corrected D
2BP baseline and D
2BP
Olz is the D
2BP for patients on a regimen of olanzapine. The absence of patients' own baseline values introduces a potential error; the error, as calculated on the basis of variance in data from neuroleptic-naive patients, is expected to vary from 0% to 9% for patients with 50% occupancy and 0% to 4% for patients who have 80% occupancy (
24).
The 5-HT
2 scans were obtained by using a bolus injection of 5 mCi of high-specific-activity [
18F]setoperone (360–6210 Ci/mmol), after the method developed and standardized by Blin et al. (
25,
26). The 5-HT
2 occupancy was determined in the prefrontal cortex regions of interest drawn on the [
18F]setoperone scan with reference to a coregistered MRI (as described earlier). An index of the 5-HT
2 receptors was obtained from the prefrontal cortex to cerebellum ratio over the 65–90-minute time period. The cerebellum is practically devoid of 5-HT
2 receptors (
27), and studies of baboons as well as of humans report no displaceable [
18F]setoperone binding in this region (
25,
26,
28). It can be shown that at a time when the binding of the radioligand is at pseudoequilibrium, the prefrontal to cerebellum ratio represents binding potential + 1 (
29). The details of this method as applied here have been described elsewhere (
30). This method yields an average test-retest deviation of 6%–7% and an acceptably high interrater reliability (ICC r>>0.95) (
30).
Since these patients were already receiving treatment, it was not possible to measure their baseline 5-HT2 binding potential. In the absence of this baseline, we used the age-corrected 5-HT2 binding potential obtained from 11 neuroleptic-free patients with schizophrenia and 26 age-matched normal control subjects. The pooling of normal control subjects and patients results in a more robust age-corrected regression and is justified, since there was neither an effect of diagnosis (F=1.23, df=1,33, p=0.28) nor a significant effect of diagnosis on the age regression (F=0.59, df=1,33, p=0.45). Occupancy was calculated in the same way as for dopamine D2 occupancy.
Coincident with the PET scans, blood was drawn for olanzapine and prolactin analysis. The levels of olanzapine were estimated in heparinized human plasma by using high performance liquid chromatography with electrochemical detection (BAS Analytics, West Lafayette, Ind.). Prolactin levels were determined by using a two-site cheminoluminometric immunoassay with a minimum detectable limit of 0.3 ng/ml and a coefficient of variance of 3.6%–4.5% (ACS, CIBA-Corning Diagnostics). Statistical analysis was implemented by using STATISTICA release 5 (StatSoft, Tulsa, Okla.).
RESULTS
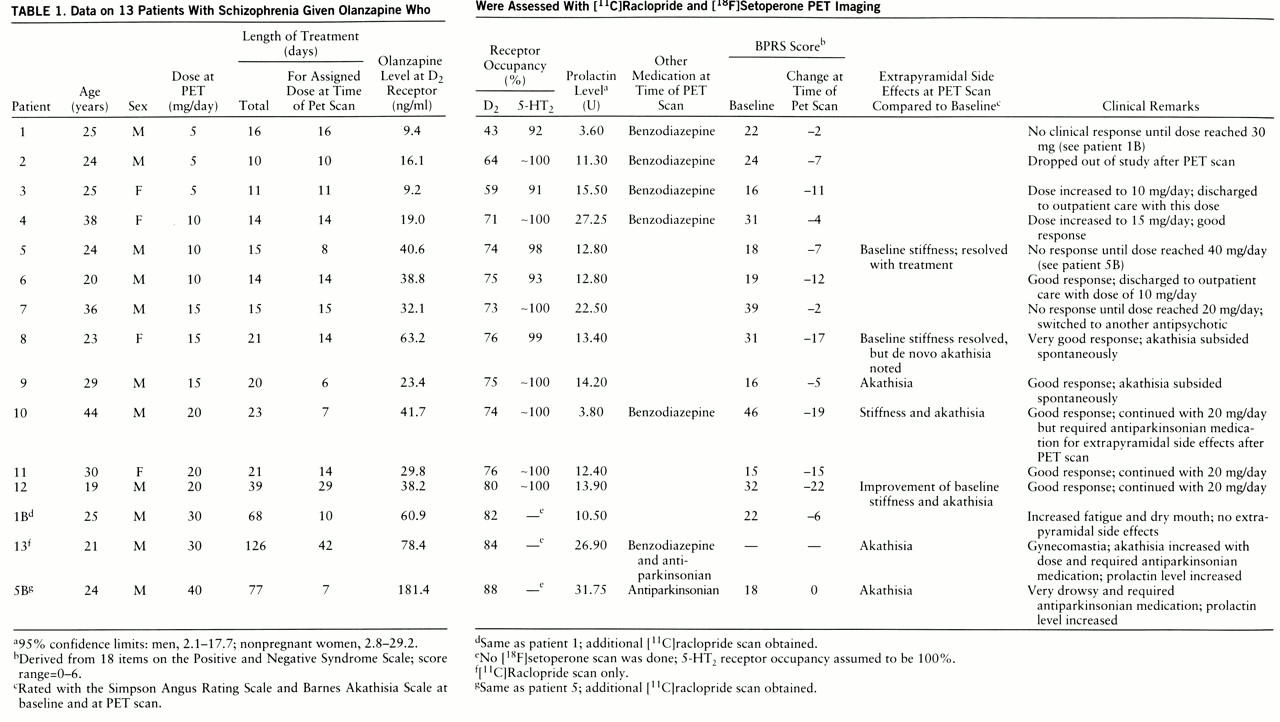
Twelve patients (patients 1–12 in
table 1) each had a [
11C]raclopride and a [
18F]setoperone scan, and three additional [
11C]raclopride scans (for patients 1B, 5B, and 13) were obtained; data on all the scans are reported. Plasma levels at the time of the [
11C]raclopride PET scan, 12 hours after the last dose, were linearly related to dose as plasma level=5.8 + 1.99×dose (F=22.16, df=1,12, multiple R=0.80, p≤0.001). The plasma levels at the time of the setoperone scan (14–15 hours after the last dose) were slightly lower than those at the time of the raclopride scan (on average, 8% lower) (paired t test t=2.63, df=11, p<0.05) but, understand~ably, were highly correlated (F=273.38, df=1,10, multiple R=0.98, p<0.001).
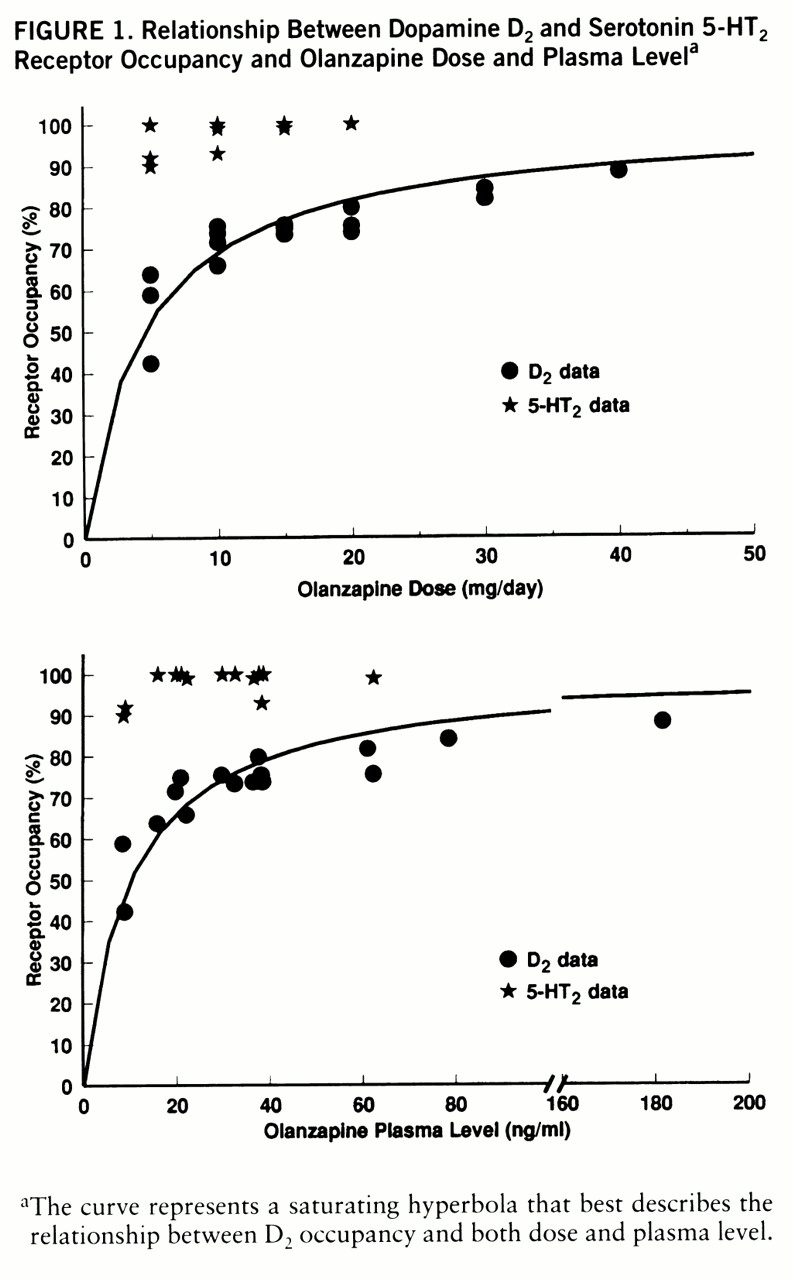
Olanzapine induced near saturation of the 5-HT2 receptors at all doses used in this study. All patients showed greater than 90% 5-HT2 occupancy, even at 5 mg/day.
The D
2 occupancy varied as a function of dose. It was an average of 55% with 5 mg/day, 73% with 10 mg/day, 75% with 15 mg/day, and 76% with 20 mg/day. The average with 30 mg/day was 83%, and the single patient on a regimen of 40 mg/day showed 88%. The expected relationship between dose/plasma levels and D
2 occupancy is that of a saturating rectangular hyperbola defined by the following equation: percent occupancy=100 (dose/(dose + ED
50), where ED
50 is the dose/plasma level that occupies 50% of the available receptors. This function fits the data quite well with an ED
50 of 4.5 mg/day of olanzapine in terms of oral dose (N=15, R=0.84, 70% of variance explained) and with an ED
50 of 10.3 ng/ml in terms of olanzapine plasma levels (N=15, R=0.83, 69% of variance explained) (
figure 1).
Patients were scanned at variable intervals after the start of olanzapine. This aspect of the design, along with the small group size, makes it difficult to draw reliable conclusions regarding the relationship between dose/plasma levels and clinical response in these data. Therefore, we have chosen to present the clinical response data on each of the patients in
table 1. In terms of side effects, three patients (patients 5, 8, and 12) in the 10–20-mg/day range noted a resolution of their baseline extrapyramidal side effects, which in all likelihood reflected a resolution of the carryover effects of the previous antipsychotic at the time of the baseline rating. On the other hand, two (patients 9 and 10) developed motor side effects with olanzapine; one developed akathisia that subsided spontaneously, while the other developed akathisia and stiffness that required antiparkinsonian medications.
Of the patients who did not respond satisfactorily to their assigned dose, two (patients 1 and 5) had their dose increased systematically to 30 and 40 mg/day but without further benefit. These patients had their D2 occupancies estimated at the higher doses and showed the expected increase in receptor occupancy (patient 1's dose was increased from 5 mg/day to 30 mg/day, and occupancy increased from 43% to 82%; patient 5's dose was increased from 10 mg/day to 40 mg/day, and occupancy increased from 74% to 88%). The second scan confirms that the lack of response at the higher dose was not due to lack of sufficient D2 occupancy. The patient who was in routine clinical treatment at 30 mg/day showed 84% D2 occupancy. Of the three patients with doses above 20 mg/day, two experienced akathisia (one with 30 mg/day and one with 40 mg/day) requiring antiparkinsonian medications.
Prolactin levels at the time of PET scans were also obtained. Of the patients in the 5–20-mg/day range, only one showed prolactin levels above the normal range (
table 1). Of the three patients with doses above 20 mg/day, two showed abnormal elevations. The subject (patient 5) whose dose was titrated from 10 to 40 mg/day showed a prolactin increase from 12.8 to 31.8 ng/ml (normal range=2.1–17.7 ng/ml), while the subject (patient 13) scanned once while taking 30 mg/day showed a value of 26.9 ng/ml. The third subject with a dose above 20 mg/day (patient 1) also showed an increase in prolactin level, from 3.6 to 10.5 ng/ml as his dose was increased from 5 to 30 mg/day. These data are to be interpreted with caution, since we do not have the subjects' own baseline (i.e., pre-olanzapine) estimates. Even if we had obtained baseline prolactin levels, the levels would be confounded because a 2–4-day washout does not eliminate the carryover effects of the previous antipsychotic. Furthermore, it has been shown previously that if prolactin elevations are noted at all at doses of 10–20 mg/day, they are generally transient. Because we determined prolactin levels only at a single point in time, we are unable to determine the persistence or transience of the levels observed at 30 and 40 mg/day. Nonetheless, until better data are available, it is valuable to consider that these data suggest that doses above 20 mg/day may be associated with a higher likelihood of prolactin elevation.
DISCUSSION
Olanzapine shows a combination of atypical and typical characteristics, as determined with PET imaging. Like clozapine, olanzapine has a potent effect on the 5-HT2 receptors. Even the lowest clinical dose of 5 mg/day occupies greater than 90% of 5-HT2 receptors. On the other hand, unlike clozapine and like risperidone, olanzapine, in routine clinical doses, occupies greater than 60% of D2 receptors and, if used at doses above 20 mg/day, occupies greater than 80% of dopamine D2 receptors. At doses above 20 mg/day, which led to greater than 80% D2 occupancy, extrapyramidal side effects and prolactin elevation were also noted. We discuss the implications of these findings for clinical practice as well as for understanding the mechanism of antipsychotic action.
This study constitutes the first systematic analysis of the in vivo occupancy of olanzapine and extends and clarifies two previous reports. Pilowsky and colleagues (
31) have reported that the D
2 occupancy of olanzapine, through use of I
123-Iodobenzamide (IBZM) single photon emission computed tomography (SPECT) imaging, is similar to that of clozapine and lower than that of typical neuroleptics. However, the report of Pilowsky et al. has several limitations. The spatial resolution, quantification, and signal/noise characteristics of IBZM-SPECT imaging are inferior to those of [
11C]~raclopride PET imaging. The study had only six patients (four on a regimen of 10 mg/day, one each on a regimen of 15 and 20 mg/day), nonrandom dose assignment, flexible dose titration, and variable duration before scanning. It did not control for age-related D
2 changes, and plasma levels were not available to confirm compliance. Furthermore, the study found no relationship between dose and occupancy, questioning the internal consistency of the data. The present study overcomes these limitations. The other previous data come from Nyberg et al. (
18), who studied three normal control subjects after a single dose of 10 mg of olanzapine. Seven hours after the dose the subjects had olanzapine plasma levels of 10–12 ng/ml, with 59%–63% D
2 occupancy. Nyberg et al. predicted that patients taking 10 mg/day would have 75% occupancy at steady state—very close to the 73% (SD=2%) that we observed. Given the limitations of the Pilowsky et al. data, and the concordance of our results with the Nyberg et al. prediction, we feel confident that our conclusion that olanzapine D
2 occupancy is higher than that of clozapine and comparable to that of typical neuroleptics is correct.
Meltzer et al. (
1,
32) have suggested that the distinguishing pharmacological characteristic of an atypical antipsychotic is a higher affinity for 5-HT
2 than D
2 receptors in vitro (
1,
32). In patients this characteristic manifests itself as greater than 80% 5-HT
2 occupancy along with less than 80% D
2 occupancy (
3,
4). By these accounts, olanzapine's in vivo pharmacology is clearly atypical. It is to be noted that olanzapine differs from typical neuroleptics along several other dimensions. In particular, it has prominent actions on the dopamine D
4 and D
1, muscarinic, and histaminic receptors (
12), any of which may, in principle, contribute to its clinical atypicality. However, at this time there are no studies of olanzapine's actions at these other receptors in humans.
While other receptors may be of additive interest in the newer atypical antipsychotics, the role of D
2 blockade is still central. Risperidone, for example, is proven to be effective only at doses that block greater than 60% of D
2 receptors (i.e., a dose of 2 mg/day), and doses that lead to greater than 80% dopamine D
2 blockade (i.e., doses above 6 mg/day) tend to lose some of their atypical characteristics (
10,
11,
33). Olanzapine also seems to share this characteristic. It has been proven to be superior to placebo in the 10–20-mg/day range (
13,
14,
16), which, as we observe here, leads to 70%–80% D
2 occupancy. Our data show that doses greater than 20 mg/day lead to higher than 80% occupancy; and this was associated with extrapyramidal side effects as well as prolactin elevation. Because of its built-in anticholinergic activity, it is likely that patients may be able to tolerate doses higher than 20 mg/day without manifest extrapyramidal side effects (akin to using haloperidol with greater than 80% D
2 occupancy but under cover of an anticholinergic). A recent report (uncontrolled case series) on the use of high-dose olanzapine (30–40 mg/day) in refractory patients found that five of eight patients experienced motor side effects, three with akathisia and four with parkinsonism, although the symptoms were mild for most patients and required medication in only one (
34). Therefore, until more systematic clinical trials are done at doses higher than 20 mg/day, it should not be assumed that the relative freedom from extrapyramidal side effects seen in the 10–20-mg/day range (
13,
14,
16) will apply to doses beyond 20 mg/day. On the basis of our PET findings, it is quite likely that doses of olanzapine higher than 20 mg/day will not exhibit the virtually complete freedom from extrapyramidal side effects and prolactin elevation that is observed in the 10–20-mg/day range.
These findings raise interesting questions regarding the comparison of olanzapine to typical neuroleptics and to clozapine. All currently published comparisons of olanzapine have used 10–20 mg/day of haloperidol as a reference drug. Thus, doses of olanzapine that result in 70% to 80% D
2 occupancy have been compared to doses of haloperidol that would result in greater than 90% D
2 occupancy for most patients (
35). It is increasingly realized that the optimal dose of haloperidol may be lower than 10 mg/day and that higher doses may result in greater extrapyramidal side effects and in higher negative symptom ratings (
36–
38). Furthermore, it has also been shown that doses which induce occupancies higher than 80% with typical neuroleptics are associated with a greater prevalence of extrapyramidal side effects (
5,
6). These facts raise an interesting question: would olanzapine demonstrate benefits on negative symptoms, extrapyramidal side effects, and prolactin that are superior to those of a typical neuroleptic, if their D
2 occupancies were matched one to one?
Olanzapine's D
2 occupancy is also of interest when compared with that of clozapine. Olanzapine is chemically very similar to clozapine and in vitro seems to have the same relative receptor affinity profile. However, its absolute affinity for the dopamine D
2 receptor is twenty-five to fifty times higher than that of clozapine. Therefore, the comparison of its D
2 occupancy in a clinical situation is of interest. While clozapine occupies, on average, 30%–60% of D
2 receptors at therapeutic doses (
8,
9), olanzapine occupies 70%–80%. This is an important distinction. It has been shown that greater than 60% dopamine D
2 occupancy may be sufficient to induce antipsychotic response in and of itself, while less than 60% dopamine D
2 occupancy may be insufficient (
6). Thus, while clozapine does not call on the typical D
2 mechanism for inducing clinical response, olanzapine in all likelihood does.
While the ultimate clinical significance of this difference between clozapine and olanzapine can be determined only in a direct clinical comparison, the D
2 data obtained here provide grounds for hypothesizing a difference. Clinical data indicate that all atypical antipsychotics are not alike. For example, risperidone is not particularly effective for individuals who have not responded to clozapine, whereas clozapine can be beneficial in up to 50% of individuals who have not responded to risperidone (
39–
41). A direct comparison between olanzapine and clozapine, and data on the use of each in patients who have not responded to the other, would provide the clinical data to understand whether this difference in D
2 occupancy manifests itself clinically.
These data need to be interpreted in light of the salient limitations of this study. The group size of the study was chosen to address the primary objective, i.e., the in vivo profile of olanzapine with respect to 5-HT
2 and D
2 occupancy at clinical doses in patients. This group is much smaller than would be required to definitively analyze the relationship between dose/receptor occupancy and clinical response. Since the dose-response relationships of olanzapine are well established from previous multicenter, fixed-dose clinical trials (
13,
14,
16), patients in this study were randomly assigned to the same doses in fixed-dose regimens so that the PET data could be related to the previously published clinical data. A second limitation of this study is the measure of D
2 occupancy. [
11C]Raclopride is the most reliable and standardized ligand for the determination of D
2 occupancy; however, it provides data only for the striatum. The exact site of antipsychotic response is not known, but it is speculated that mesolimbic dopamine D
2 receptors may be crucial determinants. Because of a low density of D
2 receptors in the mesolimbic regions, they are not reliably visualized with [
11C]raclopride. Since it has been demonstrated that olanzapine shows the same affinity for the striatal and mesolimbic D
2 receptors (
42), it is fair to consider striatal D
2 occupancy as a surrogate for mesolimbic D
2 occupancy, until more direct measures of mesolimbic occupancy are available (
43).
In summary, olanzapine saturates 5-HT2 receptors and demonstrates a higher 5-HT2 than D2 occupancy at all doses. However, its D2 occupancy is higher than that of clozapine and comparable to that reported previously for typical neuroleptics and risperidone. Thus, at doses that give higher D2 occupancies (particularly at doses greater than 20 mg/day that give higher than 80% occupancy), it may show a higher prevalence of extrapyramidal side effects and prolactin elevation. Thus, while olanzapine is a well-tolerated atypical antipsychotic in the 10–20-mg/day dose range, it may lose some of its atypical clinical benefits if used at higher doses.