Whether psychiatric patients have adequate capacities to consent to research is an object of active attention in the popular media
(1), professional literature
(2), administrative agencies
(3), and the courts
(4). Some advocates express fears that incompetent patients may be recruited into potentially harmful research projects without comprehending the choices they have made
(5). In contrast, other commentators reflect concern that overly stringent standards and procedures for recruiting patients into research projects will stymie the pursuit of answers to the etiologic and therapeutic conundrums posed by serious psychiatric disorders
(6). Although the spotlight has shone primarily on research in schizophrenia, the capacities of depressed patients enrolled in research have also been called into question
(7).
There appears to be little disagreement that major depression can have an impact on cognitive functions related to decision making. Impairments may exist in concentration (DSM-IV), information processing
(8), and reasoning
(9), among others. Decreased motivation to protect one’s interests, perhaps associated with feelings of hopelessness, may alter the nature of patients’ treatment decisions
(10). One large-scale study
(11) suggested that about 25% of hospitalized depressed patients may manifest problems related to decision-making abilities regarding treatment, roughly half as many as patients with schizophrenia. However, we know little about the impact of depression on decisions regarding research
(12).
The few data that exist indicate that severe depression can compromise patients’ capacities related to consent to research
(13). As in the clinical realm, such impairment is less common than in schizophrenia and is more susceptible to amelioration with special educational interventions
(14), but the frequency of such impairment and its relation to the degree of depression present remain unclear. Exploration of these issues has been hampered by the absence of a generally accepted means of evaluating the decision-making capacities of potential research subjects. In this article, we report the initial use with depressed subjects of a tool derived from recent work on assessment of patients’ capacities to consent to treatment
(15,
16), the MacArthur Competence Assessment Tool—Clinical Research (MacCAT-CR).
Specifically, the aims of the study reported here were 1) to determine the feasibility of using the MacCAT-CR with depressed subjects; 2) to examine the level of performance of women with major depression on the decision-making abilities assessed by the MacCAT-CR; 3) to explore relationships between performance and other subject characteristics, especially degree of depressive symptoms; and 4) to compare subjects’ performance over time, before and after entry into the study.
METHOD
The subjects in this study were the first 26 women to enroll in a study of maintenance psychotherapy in recurrent depression (E.F., principal investigator) at the Western Psychiatric Institute and Clinic in Pittsburgh. After receiving full disclosure about both the psychotherapy research and a concurrent study of their decision-making capacity, subjects gave written consent to participate. All subjects were required to meet the Research Diagnostic Criteria
(17) for major depression, recurrent, as documented by the Schedule for Affective Disorders and Schizophrenia—Lifetime Version
(18). All subjects were outpatients; their mean age was 39 years (SD=10.45, range=24–59). Their mean score on the Hamilton Depression Rating Scale was approximately 18 (SD=2.37, range=15–25), a score that is considered to represent “moderate” depression. Seventy-five percent of the subjects reported that they had never been in a research study before.
The psychotherapy study in which the subjects were enrolled was designed to test the efficacy of various schedules for interpersonal psychotherapy in sustaining remission from depression. During the acute phase of their illness, all subjects were treated for 4–6 months with weekly therapy sessions. Once stabilized, they were randomly assigned to weekly, biweekly, or monthly maintenance sessions for 2 years. Antidepressant medications were not used. Important considerations that might enter into subjects’ decisions about whether to enter the trial, therefore, might include the absence of psychopharmacologic treatment, the long-term time commitment to psychotherapy, and eventual random assignment to a psychotherapy schedule not based on an assessment of their individual needs.
All subjects in the study received the MacCAT-CR, an instrument based on a similar tool designed to aid in the assessment of competence to consent to treatment
(15,
16); it was derived in turn from research instruments used in a multisite study of decision-making capacities in mentally ill and medically ill patients
(11,
19,
20). The MacCAT-CR provides a semistructured interview format with which to assess and rate the abilities of potential research subjects according to the four most commonly accepted components of a standard for decision-making competence in clinical settings
(21,
22): understanding of disclosed information about the nature of the research project and its procedures; appreciation of the effects of research participation (or failure to participate) on subjects’ own situations; reasoning about participation; and ability to communicate a choice. (Since all subjects in this study had to be able to communicate a choice to participate, scores on this part of the instrument are not reported in this article.)
The MacCAT-CR format can be individualized for each research project, as it was here. Selected information about the psychotherapy project, reviewed for accuracy by the investigators conducting the project, was disclosed, and a standard set of questions was asked to sample subjects’ abilities. (A copy of the MacCAT-CR manual and of the version used in this study is available from the first author on request.) Questions for assessing understanding focused on 13 pieces of critical information concerning the psychotherapy study’s purpose, procedure, benefits, risks, and alternatives (e.g., “What is the purpose of the research project I described to you?”). The three appreciation questions focused on subjects’ beliefs about whether what they had been told actually applied to themselves, specifically, 1) “Do you believe that you have been asked to be in this study primarily for your benefit?”; 2) “Do you believe, as part of this study, that you will see your therapist as often as he/she thinks is best for your care?”; and 3) “What do you believe would happen if you were to decide not to be in this study any longer?” Reasoning questions centered on subjects’ abilities to compare research participation with other treatment options and to describe the everyday consequences of participation and nonparticipation (e.g., “What is it that makes [the subject’s preferred option] seem better than [the nonchosen options]?”).
As part of their training, research staff members who administered the MacCAT-CR for the psychotherapy study had their pilot administrations audiotaped. Two of us (P.S.A. and T.G.), who had developed the instrument, reviewed the tapes and the completed forms and provided feedback on their performance. Scoring was not performed by the staff members who administered the instrument but by one of the investigators (T.G.) and a trained research assistant. MacCAT-CR items are rated 2, 1, or 0 on the basis of objective criteria. The two raters independently scored five interviews and discussed and resolved any differences. Subsequent interviews were rated independently and compared until there were minimal differences. Thereafter, the research assistant rated the remaining protocols, with the investigator reviewing and occasionally revising the ratings.
Subjects were also given a set of questions about their perceptions of the consent procedures and their reasons for having decided to participate in the psychotherapy study.
Potential subjects in the psychotherapy study were seen by a project clinician within 24 hours of evaluation to describe the psychotherapy study and ascertain their interest in participating. Interested patients were seen a week later by the same clinician, who provided a more detailed disclosure (including the consent form for the psychotherapy study) and obtained informed consent. Hamilton Depression Rating Scale forms were also completed at this session.
Psychotherapy sessions began 1 week later. Immediately after the first psychotherapy session, subjects were approached by staff members from the psychotherapy study to obtain their informed consent to participate in the research consent study. None of the first 26 subjects enrolled in the psychotherapy study declined to participate in the research consent study. The subjects, who by then had received two full disclosures regarding the psychotherapy study, were then given the MacCAT-CR, which included a redisclosure of key information about the psychotherapy study as part of its procedure for assessing understanding. Finally, 8–10 weeks later, following a routine psychotherapy session, subjects were again administered the MacCAT-CR, exactly as before.
RESULTS
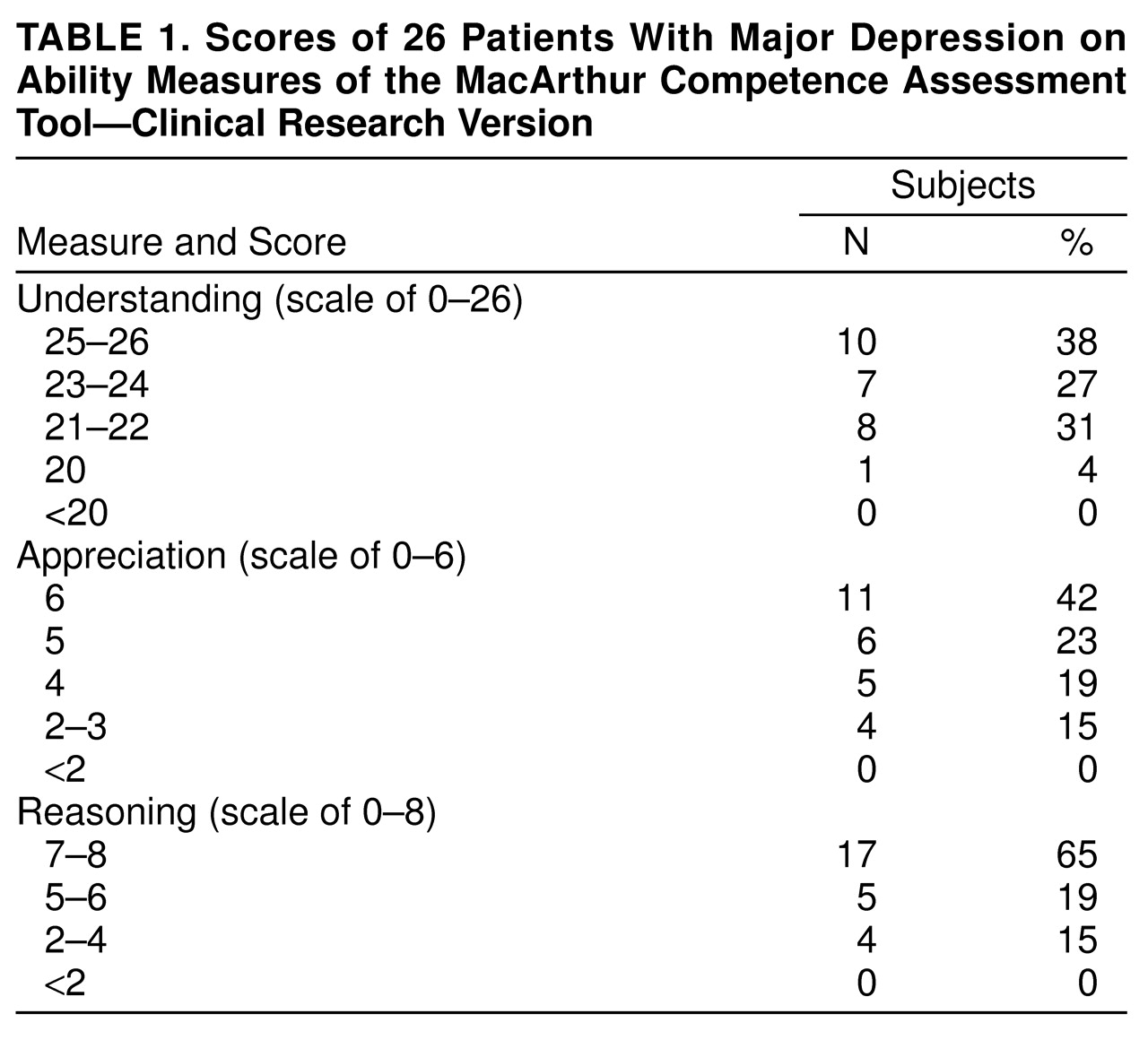
In the analysis of overall performance, at the initial administration of the MacCAT-CR, the great majority of subjects performed very well on the measures of all three abilities related to capacity to decide (
Table 1). The mean score on the understanding scale was 23.33 (SD=2.84) out of a maximum of 26, with no subject scoring below 20. More than 90% of the subjects obtained full credit on most items, and a complete lack of understanding (a score of 0 on an item) was quite rare—no subjects scored 0 on most items and at most four subjects on one item. Similarly, the mean score on the appreciation scale was 4.89 (SD=1.21) out of a maximum of 6, and the mean score on the reasoning scale was 6.50 (SD=1.75) out of a maximum of 8. Approximately 65%–75% of the subjects received full credit on most of the appreciation and reasoning items; scores of 0 were rare.
A small subgroup of subjects did poorly on appreciation and reasoning measures; one subject averaged less than a partially correct score on the appreciation scale (i.e., a total score of less than 3), and two subjects did so on the reasoning scale (i.e., a total score of less than 4).
When performance was lower on the appreciation scale, it was usually in part because of a partially correct score (i.e., a score of 1) on the question that assessed whether subjects appreciated that the frequency of therapy to which they would be assigned in the randomized phase of the study would not be based on their individual needs. The subjects appeared to be confused here by having been told of a fail-safe provision in the protocol: if their depression worsened despite psychotherapy (the frequency of which was assigned randomly), they would be taken off the assigned schedule and placed in another arm of the study. Some patients misconstrued this to mean that if they did poorly before random assignment, this could affect their assignment to frequency of therapy within the study.
Performance on understanding and performance on reasoning were significantly correlated (Kendall’s tau=0.27, N=26, p=0.05), while neither was significantly correlated with appreciation scores (for understanding, Kendall’s tau=0.03, N=26, p<0.87; for reasoning, Kendall’s tau=0.27, N=26, p<0.08). This has been a consistent finding in earlier research on decisional abilities that used related instruments
(12,
17).
In the analysis of the relation of performance to subjects’ characteristics, there was only one significant correlation between age or severity of depression (based on Hamilton scale scores) and performance on any of the three MacCAT-CR ability measures: younger women performed better on the appreciation measure (Kendall’s tau=–0.40, N=26, p=0.05). The effect of prior research experience was also limited to appreciation. All six of the subjects with prior research experience obtained full credit on all three appreciation items; in contrast, only about one-half of the 20 women with no prior experience obtained full credit on two of the appreciation items. The small number of subjects with prior experience precluded the use of tests of significance.
In the analysis of changes in performance over time, as a group the subjects had scores on appreciation and reasoning at 8- to 10-week follow-up that were almost identical to those at the initial administration of the test. There was some improvement in scores on understanding, but not to a statistically significant extent; given the already high scores at the initial MacCAT-CR interview, significant improvement in understanding was unlikely.
Test-retest correlations for understanding (Kendall’s tau=0.26, N=26, p=0.08) and appreciation (Kendall’s tau=0.36, N=26, p=0.01) were at or near significance but not very strong. This is to be expected when ratings are clustered within a small range. The test-retest correlation for the reasoning scores was –0.15 (Kendall’s tau, df=26, p=0.97), indicating no relation between performance at the first and second administrations. Inspection of subjects’ verbatim responses leads us to believe that this may be an artifact caused by the tendency of subjects to truncate their answers to reasoning questions (which ask them to “think aloud” about their choices) on repeat administration of the test. Future studies using the MacCAT-CR with test-retest designs may need to provide special instructions to examiners to counteract this change in response style by some subjects.
In this exploratory study, we augmented the MacCAT-CR with several open-ended questions designed to explore in greater depth subjects’ reasons for participating in the psychotherapy study. We were concerned about the adequacy of our appreciation questions for assessing subjects’ grasp of the implications of research involvement.
When asked why others would participate in the research, one-third to one-half of the subjects mentioned one or more of three reasons: financial advantages (i.e., the therapy was free), higher anticipated quality of treatment at this well-known center, and obtaining help. Only one subject mentioned altruistic reasons (i.e., to help other depressed women by contributing to the advancement of knowledge about treatment of the disorder). When asked why they themselves had decided to participate, in contrast, 80% of the subjects mentioned the desire to obtain help for their depression, and roughly one-third of the subjects offered only this reason. This may raise some question about these subjects’ abilities to distinguish between reasons for seeking ordinary clinical care—usually, to obtain the care that a professional believes is most appropriate for a patient—and for participation in research studies—which, however potentially beneficial, does not guarantee the same kind of individualized treatment decisions.
Subjects’ reasons for why others might not want to participate focused most often on the length of the commitment to therapy (2 years). One-quarter of the subjects mentioned that the treatment conditions were controlled by research requirements rather than by subjects’ individual needs, and another quarter pointed to some people’s fears about being in research studies in general.
DISCUSSION
In this study, nonhospitalized women with major depressive disorder of at least moderate intensity performed quite well on a measure of their decision-making capacities related to research. Few subjects manifested difficulties with understanding, appreciation, or reasoning to a degree that would raise suspicions about their capacity to make an informed choice. Moreover, at least in this outpatient group, the extent of depressive symptoms did not seem to affect the level of performance—perhaps a counterintuitive finding, and certainly one that requires confirmation. Nonetheless, these data appear to be reassuring to those who have expressed concerns that researchers might face widespread difficulties with informed consent in depressed populations.
This conclusion, however, must be tempered by the recognition that our study group was small and not typical of all persons with depression. Persons with depression severe enough to require hospitalization, perhaps especially those with psychotic depression, may manifest higher levels of decisional incapacity. This would be consistent with previous research on consent to treatment and consent to research that pointed to potential problems with these groups
(11,
13). Further work with what might be higher-risk populations certainly seems warranted.
If there was an area of performance about which concern might be expressed, it was subjects’ performance on the appreciation measure, which raised some questions. A large number of subjects obtained partially correct scores on a question that required them to apply their knowledge that treatment would be randomly assigned after the initial stabilization period. This could be interpreted in one of two ways. Subjects might simply have been confused by information provided to them which indicated that special measures would be taken after random assignment to treatment if their conditions worsened markedly. In this case, our findings would indicate a modest failure of understanding rather than of appreciation. Alternatively, the propensity of subjects to manifest precisely this confusion could be attributed to what has been referred to as the “therapeutic misconception”—the tendency of research subjects to believe that research methods will not interfere with their receiving individualized care
(23). The large proportion of subjects who indicated that their motivation (as opposed to the likely motivation of others) in entering this study was to obtain help for themselves might support this latter interpretation and may underscore the importance of investigators being as explicit as possible about the limits on personalized care inherent in their research projects.
This initial study of the MacCAT-CR with a depressed study group suggests the overall utility of the instrument. It proved straightforward to administer to subjects, requiring 15–20 minutes. Interviewers with no previous experience with the method learned it quickly after brief training and review of several practice cases. The MacCAT-CR format adapted easily to the relevant content for informed consent in this particular clinical study. Questions about the stability of MacCAT-CR ratings over time could not be answered because of the overall high level of performance of the subjects in this study group. Also the utility of the instrument with more highly impaired populations will have to be explored in other studies. Finally, it is clear that procedures need to be modified when the MacCAT-CR is used with test-retest designs.