Bulimic symptoms were recognized in anorexia nervosa long before bulimia nervosa was delineated as a distinct syndrome
(1). The delay in recognizing bulimia nervosa may have been partially attributable to the observed crossover of patients from anorexia nervosa to bulimia nervosa. Indeed, early debates centered on whether bulimia represented an end stage of anorexia nervosa, a subgroup of women with anorexia nervosa, or a separate syndrome
(1). More recently, some authors have argued that “bulimia nervosa and binge eating disorder may not represent distinct nosological entities” (
2, p. 382). Recommendations to consolidate all eating disorders as one diagnosis have been made as well
(3). Information concerning long-term outcome can determine the predictive validity of bulimia nervosa as a distinct diagnostic category. However, little is known regarding long-term outcome, given bulimia nervosa’s recent delineation as a syndrome.
This study sought to investigate the predictive validity of bulimia nervosa as a diagnostic category. Additionally, we explored the relation of eating disorder outcome to other axis I disorders.
METHOD
Subjects (N=222) who were diagnosed with bulimia nervosa during their participation in a study at the University of Minnesota
(4,
5) were assessed a mean length of 11.5 years (SD=1.9) after presentation. At baseline the women met the DSM-III criteria for bulimia and the additional criterion of binge eating and purging at least three times each week for 6 months. Additional baseline inclusion and exclusion criteria are presented elsewhere
(4,
5).
Of the 222 subjects we sought for follow-up assessment, 22 (9.9%) could not be located, one (0.5%) was deceased, one (0.5%) was severely disabled, and 21 (9.5%) declined or did not complete participation. Thus, 177 women (79.7%) participated. Participants and nonparticipants did not differ significantly on baseline demographic variables or severity of disorder
(6). The women had a mean age of 35.3 years (SD=5.1) and were predominantly Caucasian (98.9%).
After a complete study description, written informed consent was obtained from the subjects. The subjects completed the Structured Clinical Interview for DSM-IV Axis I Disorders
(7) and the Hamilton Rating Scale for Depression (8). Reliability estimates were generally high (Cronbach’s alpha r=0.82 and kappa=0.73–1.00). Data were analyzed by using SPSS for the Macintosh. Tests were two-tailed with an alpha of 0.01.
Eating disorder outcome was defined both as categorical and continuous variables. The categorical definition distinguished between the women who met the DSM-IV criteria for an eating disorder and the women who were free from recurrent eating disorder symptoms during the month preceding the assessment. The continuous definition represented the natural log of months between the most recent binge or purge episode and the assessment.
RESULTS
No significant differences based on the original study
(4,
5) existed after we controlled for the duration of follow-up (p>0.10 for all values). Therefore, data are presented for the total study group.
Four women appeared retrospectively never to have met the DSM-IV criteria for bulimia nervosa and were eliminated from all subsequent analyses, resulting in 173 women with a lifetime history of bulimia nervosa. At the follow-up assessment, 19 (11.0%) of the women met the criteria for bulimia nervosa. Sixty-two women (35.8%) had a lifetime history of anorexia nervosa on the basis of follow-up ratings on the Structured Clinical Interview for DSM-IV Axis I Disorders. Of these women, only one (1.6%) currently met the criteria for anorexia nervosa. Nineteen women (11.0%) had a lifetime history of binge eating disorder; however, only one (5.3%) of these women currently had binge eating disorder. Thirty-two women (18.5%) currently had an eating disorder not otherwise specified.
Eating disorder not otherwise specified was the most common eating disorder at follow-up (χ2=28.0, df=2, p<0.001). Among these women, recurrent binge-purge episodes or purging alone were significantly more common than recurrent binge eating alone (χ2=9.2, df=2, p=0.01).
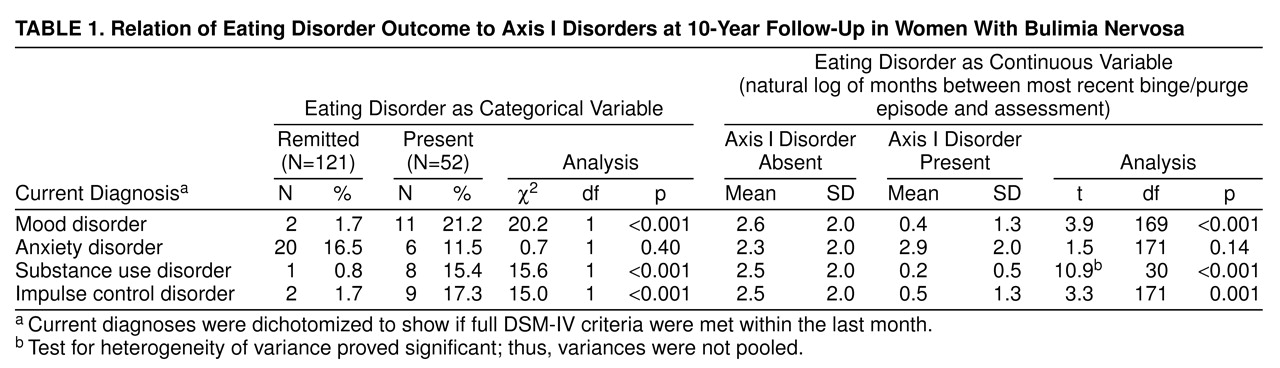
The relation of current axis I pathology to eating disorder outcome appears in
table 1. Eating disorder outcome was associated with current mood disorders and Hamilton depression scale scores (t=3.3, df=75, p=0.002; r=–0.19, N=173, p=0.01, for categorical outcome and continuous outcome, respectively). Current substance use and impulse control disorders but not anxiety disorders were also associated with eating disorder outcome.
DISCUSSION
This study investigated the predictive validity of bulimia nervosa by exploring its long-term outcome and relation to other axis I disorders. More than 10 years after the women presented with bulimia nervosa, their bulimic symptoms remained predominant within full and subthreshold eating disorder diagnoses. Furthermore, bulimia nervosa outcome clustered with syndromes marked by distress and disinhibition, distinguishing it from restricting anorexia nervosa, which clusters with syndromes characterized by distress and inhibition
(9). Finally, bulimia nervosa appears to have a favorable prognosis compared to that of anorexia nervosa
(6). Our results support the predictive validity of bulimia nervosa as a syndrome distinct from anorexia nervosa and binge eating disorder, pending further study data on the latter.
The relation of eating disorder outcome to mood disorder at follow-up replicated the findings of other investigations
(10,
11). Conversely, the relation of eating disorder outcome to substance use disorder did not
(11). Too few studies have investigated comorbid substance use disorder to clarify the meaning of this. Women with poor eating disorder outcomes were not at an increased risk for current anxiety disorder, replicating the results from another investigation
(12).
The strengths of this study include its size, follow-up duration, and participation rate. Additionally, the assessments employed psychometrically sound instruments. A limitation was the nonparticipation of 20% of the women we sought from the first assessment, which may have produced an underestimation of the diagnosis of current axis I disorders. Additionally, our participants may not be representative of the bulimia nervosa population, owing to selection biases based on treatment seeking or completion.
Nearly 30% (N=52) of the women met the criteria for a current eating disorder that most often involved recurrent binge-purge episodes. Women who continued to struggle with an eating disorder were more likely to have current mood, substance use, and impulse control disorders. These results suggest that such problems may be prolonged by a continuing eating disorder or may limit success in resolving an eating disorder. Thus, treatments may benefit from focusing on difficulties in affect regulation and impulse control.