What is the role of sleep disturbance in the onset of depression? From a clinical perspective, there clearly is a strong association between sleep problems and depression, so much so that disturbed sleep (insomnia and/or hypersomnia) has been included as one of the nine diagnostic criteria in DSM-III, DSM-III-R, and DSM-IV for major depressive episodes.
Ford and Kamerow
(12) found that subjects with complaints of persistent insomnia were three times more likely to develop depression within a 1-year interval than those without persistent insomnia. Dryman and Eaton
(13) found the emergence of four depressive symptoms over the course of a year to be associated with the onset of new episodes of depression. One of these symptoms was disturbed sleep. Breslau et al.
(14) reported that the relative risk for the onset of major depression was four times greater for subjects with a lifetime history of 2 or more weeks of insomnia than for those without such complaints. Rodin et al.
(15) found an association between depressed mood and self-reports of four sleep problems over a 3-year period. Early morning awakening was the sleep symptom that most consistently related to depressed mood over time. In the longest prospective study yet reported, Chang et al.
(16) found the relative risk of clinical depression was double for men with reported insomnia at baseline. Livingston et al.
(17) reported that the strongest predictor of future depression among those who were not depressed at baseline was sleep disturbance at baseline. Only two of these prospective studies
(15,
17) examined sleep and depression by using data from study groups of older subjects. Thus, at this point, we have few data on the role of sleep disturbance as a precursor or prodrome
(18) of depression that occurs later in life.
Our purpose in this report is to provide additional data on the role of sleep disturbance in the occurrence of depression among older persons. Specifically, we examine the risk of depression occurring among older individuals who had sleep disturbances but did not meet the symptom criteria for DSM major depression at baseline.
By using data from the 1994 and 1995 Alameda County (California) Study surveys, we estimated the prevalence of symptoms of DSM-IV major depressive episodes in the Alameda County cohort and examined associated risk factors—in particular, the effects of sleep complaints—on subjects age 50 years and older.
RESULTS
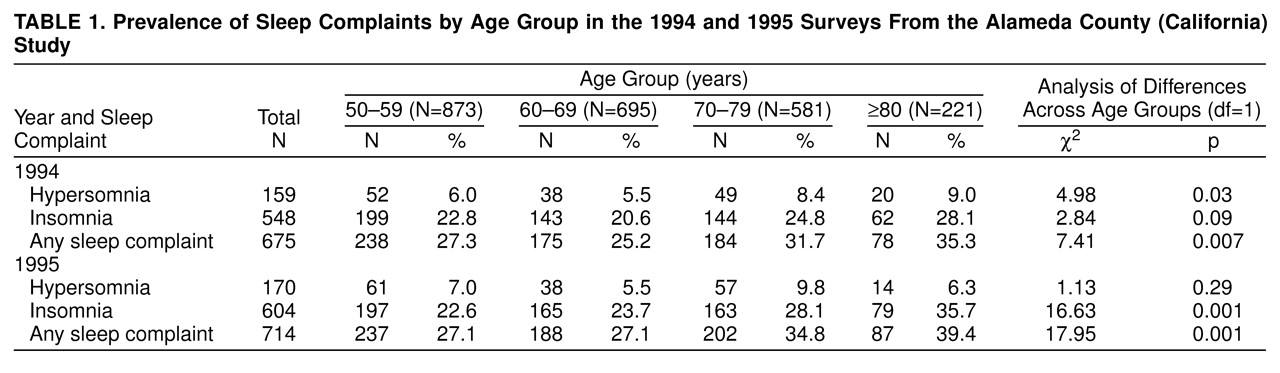
table 1 presents data on the prevalence of sleep complaints in the Alameda County Study cohort in 1994 and in 1995. There was a statistically significant difference in the self-reported prevalences of insomnia and hypersomnia across age categories. A chi-square test for trends revealed an association between sleep problems and age for hypersomnia and for any sleep problem in 1994 and for insomnia and for any sleep problem in 1995. For example, the prevalence of any sleep problem in 1994 was 27.3% among subjects aged 50–59 years and 35.3% among those aged 80 years and older. In 1994, the overall prevalence of insomnia was 23.1%, and the overall prevalence of hypersomnia was 6.7%. The prevalence of any sleep complaint was 28.5%.
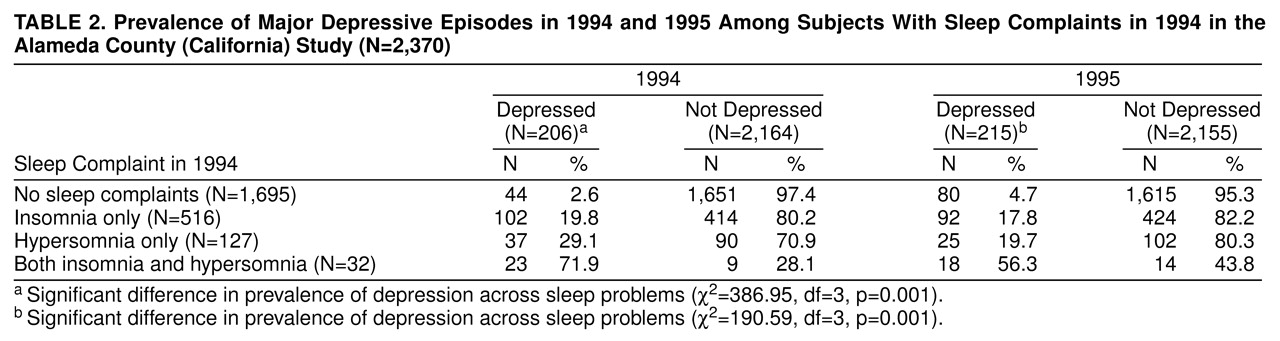
table 2 presents data on the association between sleep problems and DSM-12D depression in 1994 and 1995. As shown, the relation was pronounced. In 1994, only 2.6% of those with no sleep complaints were classified as depressed, whereas 71.9% of those with both sleep complaints were depressed. Prospectively, the pattern was very similar. That is, 1994 sleep problems were significantly associated with depression in 1995.
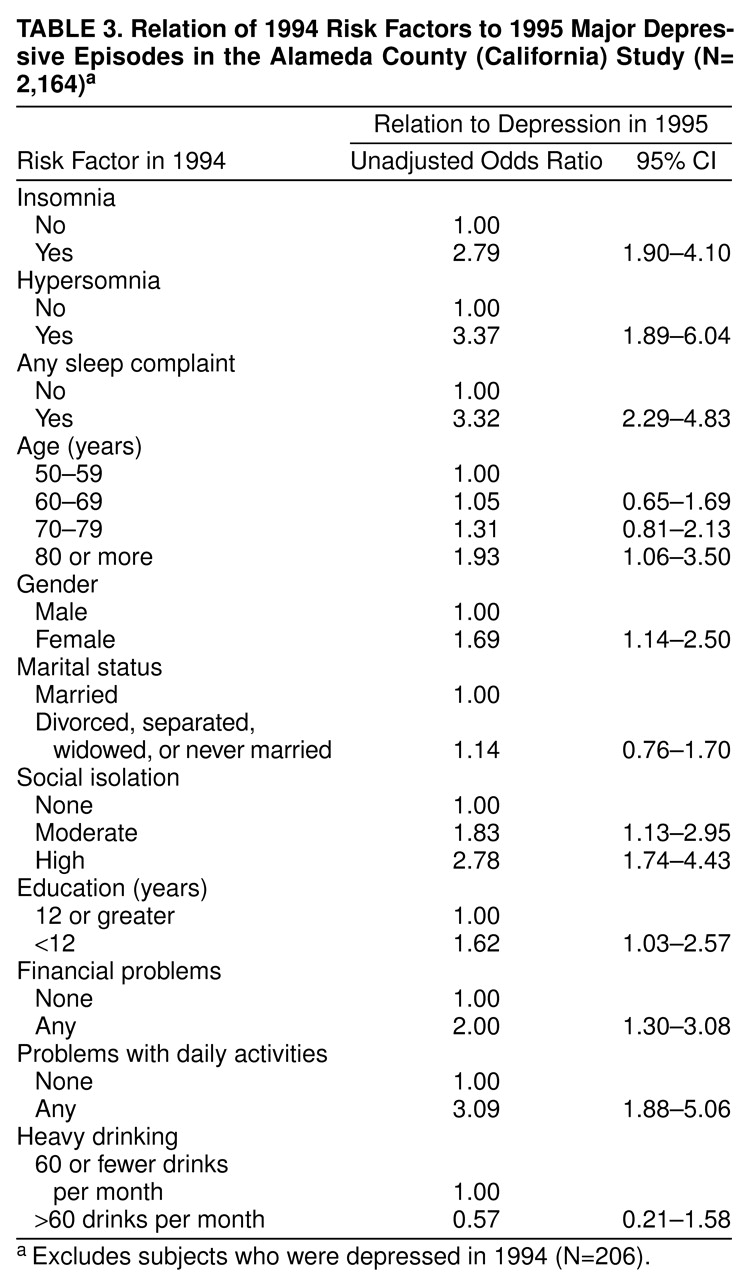
The crude association of putative risk factors (including sleep disturbance) measured in 1994 to depression status in 1995 is presented in
table 3. For these analyses, we eliminated from the cohort all subjects who met the DSM-IV diagnostic criteria for major depressive episodes at baseline in 1994. Significant correlates of depression were sleep complaints, female gender, older age, high level of social isolation, low education level, financial problems, and problems with daily activities. Alcohol use was not related to depression. A perusal of the crude odds ratios presented in
table 3 indicates that the strongest correlates of depression were problems with daily activities and sleep complaints.
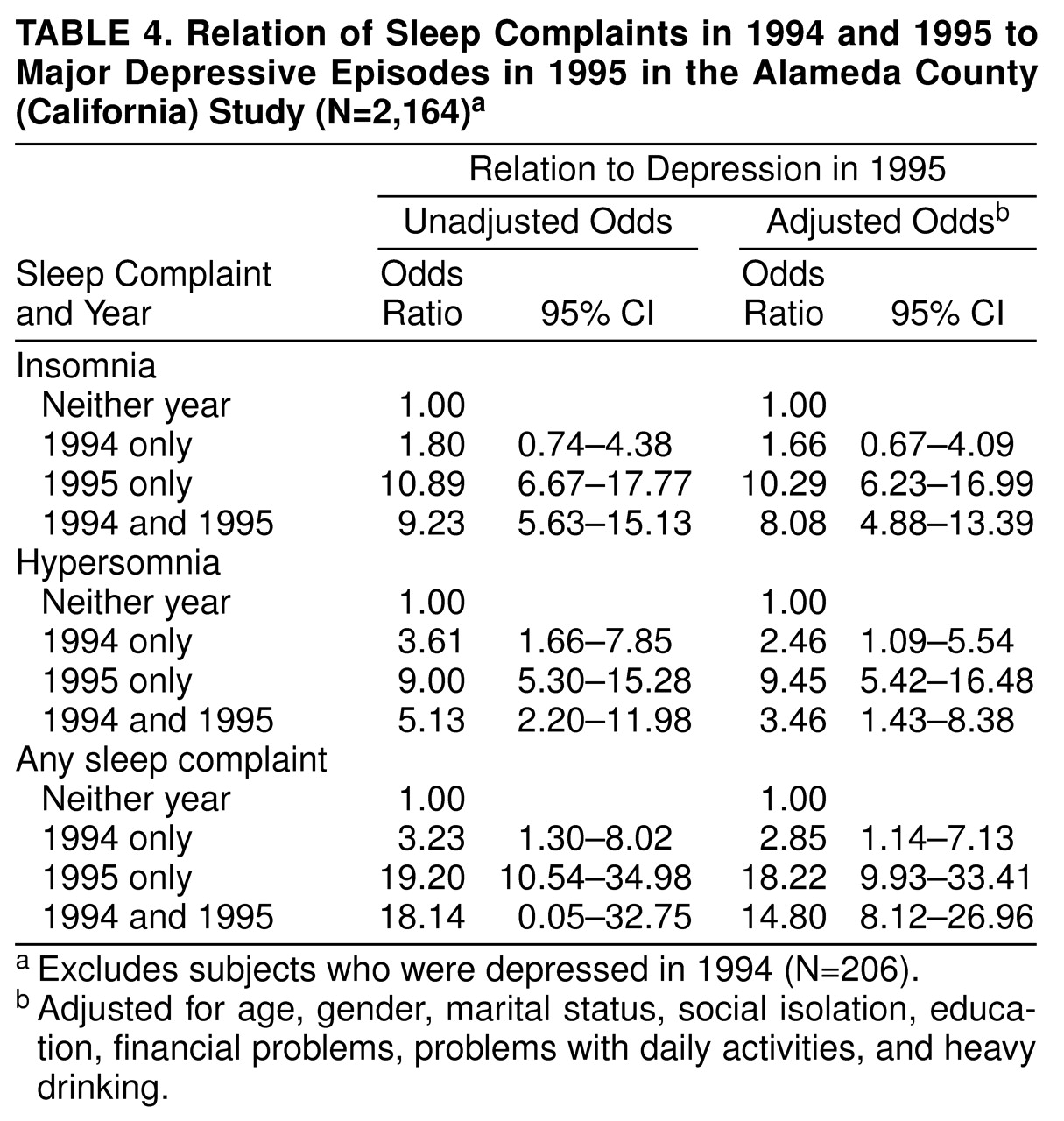
We then examined the association of sleep complaints in 1994 and 1995 to the risk of depression in 1995. As was done previously, subjects with sleep problems in 1994 who did not meet the diagnostic criteria for major depressive episodes were used to examine the risk for depression in 1995. As shown in
table 4, the strongest risk factor for depression in 1995 was a sleep complaint in 1995, as expected. However, a sleep complaint in both 1994 and 1995, which suggests chronic sleep difficulties, substantially increased the relative risk of depression in 1995. Sleep complaints only in 1994 increased the relative risk of depression much less, and for insomnia, the increase was not statistically significant. These associations held for univariate associations and in multivariate analyses that controlled for the other risk factors presented in
table 3.
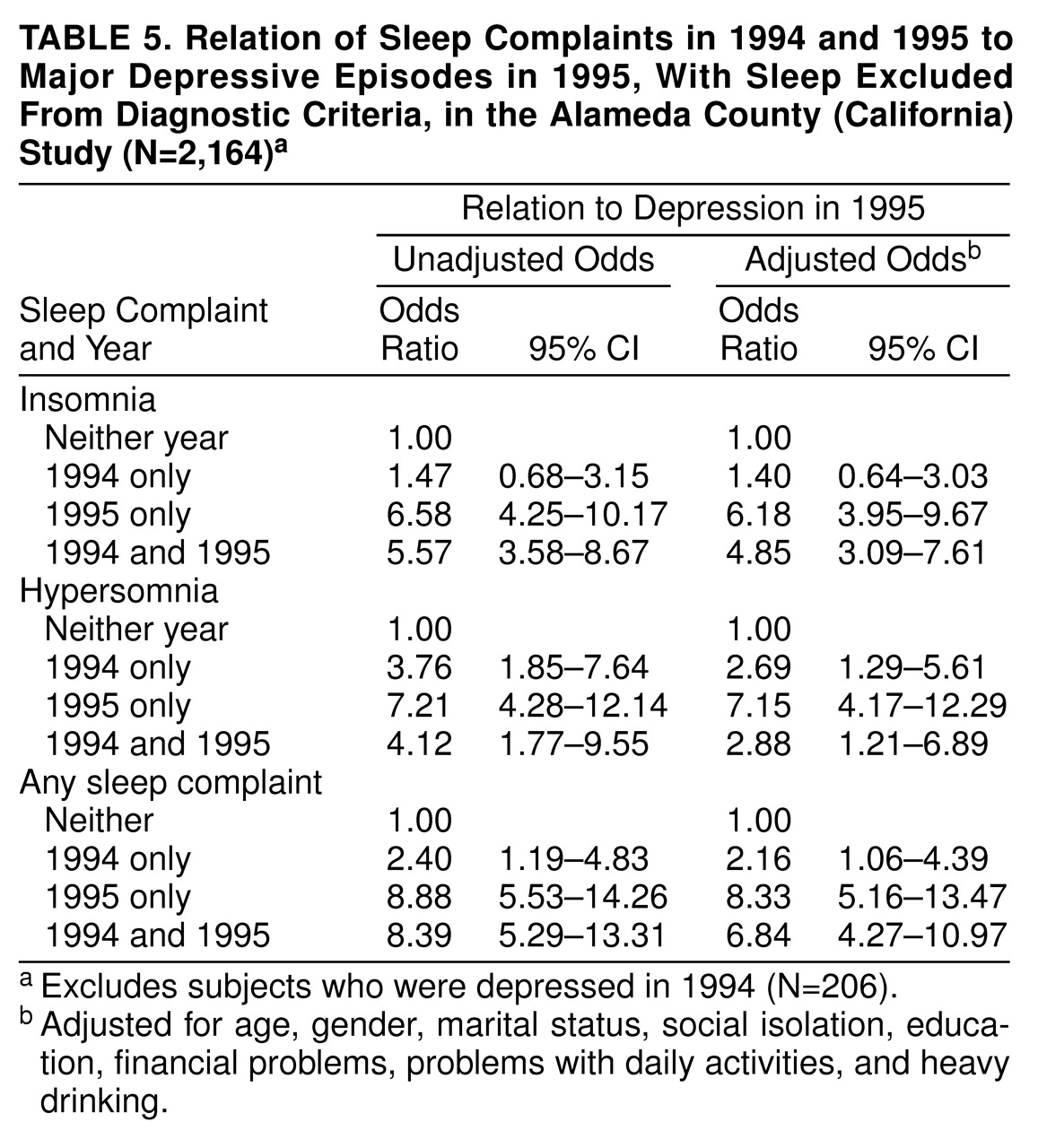
As shown in table 5, eliminating the symptoms of disturbed sleep from the diagnostic criteria for major depression did not alter the association observed in
table 4, with one exception. The odds ratios declined in value, substantially so in the case of any sleep problem in 1995 only or in 1994 and 1995. But the same pattern was observed in <
table 4 and
table 5—a sleep problem in both 1994 and 1995 was a stronger predictor than a sleep problem only in 1994, and a sleep problem only in 1995 also was a strong predictor of 1995 depression. In
table 5, even with sleep removed from the diagnostic criteria for major depressive episodes, current sleep problems were a strong predictor of a current major depressive episode.
At one level, our analyses could be construed as testing whether sleep in 1994 predicts conversion from not meeting the DSM criteria for major depressive episodes in 1994 to doing so in 1995. One way to address this issue would be to construct a measure of subthreshold depression and to examine the risk of subthreshold depression in 1995 among those with and without a sleep disturbance at baseline in 1994. We attempted such an analytic strategy, but after we defined depression as a mood disturbance and/or anhedonia plus three other criteria (excluding sleep), there were insufficient numbers of subthreshold cases to sustain multivariate analyses prospectively. Thus, we were not able to explore this issue and cannot rule out this possibility. Still, we believe our results make it reasonably clear that sleep disturbance has implications for the development of DSM-IV episodes of major depression.
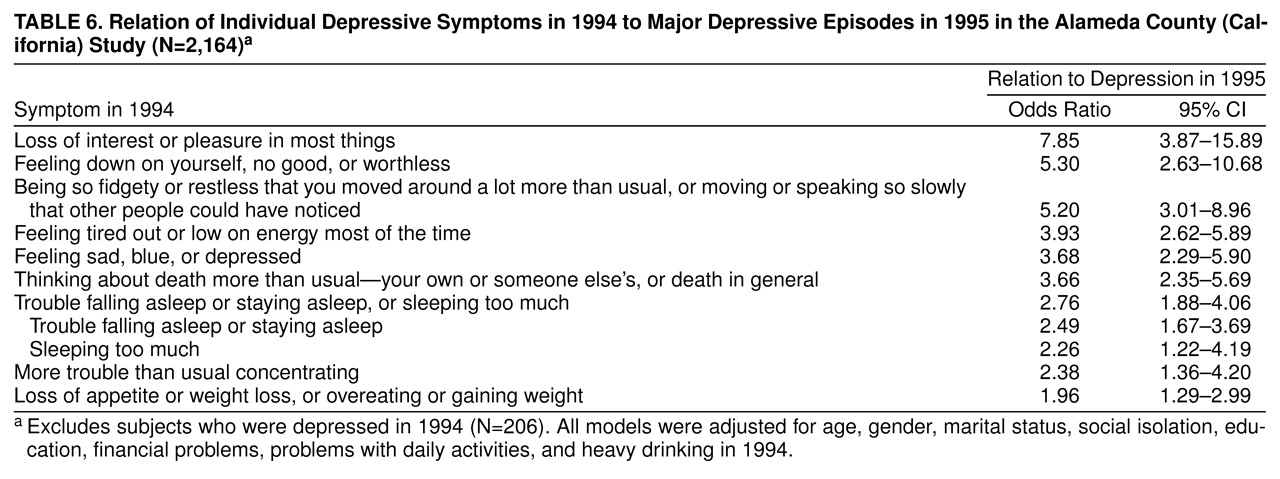
However, we then posed a different question. Given that sleep disturbance is a significant predictor of the risk of future episodes of depression, what is the importance of sleep relative to the other diagnostic criteria? These results are presented in
table 6. When we analyzed the data for this question, it became clear that the symptoms of disturbed sleep, while a significant predictor of future episodes of major depression, are not among the most important criteria. When they are arrayed in descending order according to the magnitude of their odds ratios, the symptoms of disturbed sleep rank near the bottom in predicting future depressive episodes. For this older study group, anhedonia, feelings of worthlessness, psychomotor agitation/retardation, mood disturbance, and thoughts of death are more strongly associated with future episodes of depression than are symptoms of sleep disturbance. We also examined the effect on 1995 depression status of symptoms of disturbed sleep only in 1994, only in 1995, and in both 1994 and 1995. The same general pattern observed in table 6 was observed (data not shown). That is, the symptoms of disturbed sleep ranked well behind mood disturbance, anhedonia, fatigue, worthlessness, psychomotor agitation, and thoughts of death in terms of the relative risk for 1995 depression.
DISCUSSION
To summarize, our analyses of the Alameda County Study cohort data from the 1994 and 1995 surveys indicate that sleep complaints increase the subsequent risk of depression. In 1994, those with any sleep complaint had a 2.85 relative risk of being depressed in 1995. Those with hypersomnia in 1994 had a 2.46 relative risk of depression in 1995. The increase in relative risk for those with insomnia in 1994 was 1.66, but this was not statistically significant (
table 4).
The Alameda County Study data also demonstrate the possible role of chronic sleep problems in the relative risk for depression. Among those with insomnia in both 1994 and 1995, the relative risk for depression in 1995 was 8.08. For those with hypersomnia in 1994 and 1995, the relative risk for depression was 3.46. For those with any sleep complaint in both 1994 and 1995, the relative risk for depression in 1995 was 14.80 (
table 4). Some of this increased relative risk is, of course, probably the result of the presence of depression in 1995. The data in
table 5 indicate that, even with the symptoms of disturbed sleep removed from the diagnostic algorithm for major depressive episodes, sleep in 1995 was still the strongest predictor of depression in 1995, relative to the other putative risk factors, although the magnitude of the odds ratios was substantially reduced from
table 4 to
table 5.
Our results add to the growing literature on the role of sleep disturbance in the risk of developing depression. Several studies that did not focus on older study groups have found an increased risk of depression at follow-up among those with sleep problems at baseline
(12,
14,
16,
26,
27). In several of these, the odds ratios for depression were three to four times greater for those with sleep problems at baseline. Evidence from the two prospective studies involving older study groups also corroborate our results
(15,
17). On the other hand, there is some negative evidence
(28).
In addition to these community-based, epidemiologic studies, there is evidence that sleep disturbance also affects the clinical course of depression. Perlis et al.
(29), using data from a group of 14 formerly depressed patients aged 27–49 years, found that patients who had subsequent greater levels of sleep disturbance several weeks before an episode of major depression were at an increased risk for such episodes. They suggested that sleep complaints may precede the series of symptoms that constitute the syndrome of major depression.
However, our analyses also provide a cautionary note. When we examined the role of disturbed sleep in the risk for future episodes of depression, compared to the role of the other symptoms of depression, our results suggested that disturbed sleep is less important. Data from this cohort of older subjects indicate that symptoms such as anhedonia, feelings of worthlessness, psychomotor agitation/retardation, mood disturbance, and thoughts of death are much stronger predictors of future major depressive episodes.
Ford and Kamerow
(12) did not examine the risk imposed by the symptoms of disturbed sleep relative to the other diagnostic criteria for depression. However, Dryman and Eaton
(13) did such an analysis. The subjects in the Epidemiologic Catchment Area (ECA) study group were age 18 years or older, and the results were presented separately for men and women. For the latter group, disturbed sleep ranked third in predicting future major depressive episodes behind trouble concentrating and feelings of worthlessness or guilt. For men, sleep disturbance was the least predictive for the risk of future episodes of major depression. Indeed, sleep was not a statistically significant predictor of subsequent episodes of major depression. The most robust risk factors for subsequent depression among men were the same for women—trouble concentrating and feelings of worthlessness or guilt. Dysphoric mood was not included, since all patients had to meet this criterion. Thus, our results corroborate the results for men reported by Dryman and Eaton
(13) but not their results for women. These differences may be due to the differences in study group composition or measures of depression. Dryman and Eaton used the NIMH Diagnostic Interview Schedule and the DSM-III criteria; we used a symptom checklist and the DSM-IV symptom criteria.
Our results also clearly indicate that increasing age is associated with an increased prevalence of sleep problems (
table 1). Insomnia, hypersomnia, and any sleep problems increased from age 50–59 years to age 80 years and older. The prevalences were between 20% and 40% for insomnia and any sleep problem. Prevalences were much lower for hypersomnia. The association was not uniformly monotonic. In fact, there appears to be a clear threshold effect, with those age 70 and older reporting higher prevalences of sleep problems in both 1994 and 1995 than those younger than age 70 years. How do our rates compare to those from other studies? Morgan
(30) reviewed the results of six studies that presented data on older adult populations (most were age 65 years or older). He concluded that between 20% and 40% of elderly people living at home experience disturbed or poor-quality sleep, ranging from moderate to severe. Since that review, other articles on the prevalence of sleep disturbance in community groups of older persons have appeared. In a number of these
(3,
5,
8,
17,
31), the prevalences fell between 20% and 45%. Our prevalences of any sleep problem (28.5%) and insomnia (23.1%) are at the lower end of this range, but they are within the range nonetheless. Most previous studies did not focus on hypersomnia.
Some studies have shown lower prevalences of disturbed sleep—some substantially lower
(4,
6,
7,
12,
32). Such differences are essentially indicative of the impact of case definition on subsequent prevalence rates.
Like all field studies, the Alameda County Study imposes certain limitations on the analysis and interpretation of the data. First and foremost, our measure of disturbed sleep was not comprehensive. While we were able to examine both hypersomnia and insomnia, we were not able to examine different dimensions of the latter. For example, we did not have separate data on difficulty initiating and difficulty maintaining sleep and on early morning awakening. The latter has been implicated in the risk of depression in adult study groups
(14,
15).
As noted earlier, our sleep items assessed whether subjects had experienced disturbed sleep (insomnia or hypersomnia) almost every day in the past 2 weeks. The items were a subset of the DSM-IV diagnostic criteria for a major depressive episode. Thus, our results were limited in that we were not able to partition our study group into those with acute sleep problems and those with chronic sleep problems. In their epidemiologic study from the United Kingdom, Ohayon et al.
(32) found that the median duration of the symptoms of insomnia was 24 months. We could not examine whether the risk factor profiles differed for those with sleep disturbances of shorter and longer duration, although it might be expected that the role of comorbid somatic and psychiatric problems would be more pronounced for chronic sleep problems
(33). We also should note that since our measure of disturbed sleep was part of our measure of depression (as per DSM-IV), we analyzed our data on the association of sleep with and without the sleep symptoms in our definition of depression. The fact that sleep still predicted depression provides a more convincing case for this association. Even so, future research should focus on acute and chronic sleep disturbances and their impact on the subsequent risk for depression.
Comorbid psychiatric disorders—in particular, anxiety and drug and alcohol abuse disorders—might confound the observed association between the symptoms of disturbed sleep and depression. For example, Ford and Kamerow
(12) found that subjects in the ECA study with disturbed sleep at baseline were at an increased risk of subsequent episodes of major depression, anxiety disorders, alcohol abuse, and any psychiatric disorder. The Alameda County Study was an omnibus health survey and, as such, did not include diagnostic data on anxiety or substance abuse disorders. However, we did include a measure of the quantity and frequency of alcohol consumption. This measure contributed little to the observed association between sleep and depression. Clearly, comorbidity is an area for future exploration.
Another obvious limitation is that we did not have objective data on disturbed sleep. That is, we did not have physiological measures of sleep generated by procedures such as EEGs. Whereas such measures are desirable, to date they have not been regularly incorporated into community-based, epidemiologic studies. Thus, whereas such data would be useful to have, self-reports and interview-based measures remain the measures most widely used in community surveys. Our study was no exception.
To summarize, we believe that the available evidence is reasonably clear on three points. First, sleep disturbance exhibits strong patterns of co-occurrence with other defining symptoms of major depression. Second, sleep disturbance, particularly of a chronic nature, is associated with the risk of subsequent depression. In fact, several studies
(18,
29) suggest that sleep disturbance may occur before and presage development of the full clinical syndrome of depression. Third, whereas the symptoms of disturbed sleep may constitute precursor or prodromal symptoms in the development of clinical depression
(29), the etiologic role of sleep vis-�-vis the other symptoms of depression remains poorly understood. Our data suggest that disturbed sleep may not be as important as the other diagnostic criteria in predicting who might be at risk of future episodes of depression.
We suggest that more effort needs to be directed at understanding the timing and sequence of precursor or prodromal symptoms in the development of clinical syndromes. From an etiologic perspective, one unresolved question is the natural history of symptoms that constitute the diagnostic criteria for depression. That is, what is the risk for future episodes of depression that is attributable to the various diagnostic criteria—in this case, the symptoms of disturbed sleep? If strong precursors (i.e., those with a high attributable risk) can be identified, then we have potential targets for preventive interventions
(18). When we realize that the prodromal period may be quite long (perhaps 8–10 years in the case of major depression
[18]), preventive intervention strategies directed at strong precursors may have time to lower the risk of developing the full clinical syndrome. In this case, what may be more useful from a prevention perspective is knowledge about the risk factors that affect precursor symptoms such as disturbed sleep rather than clinical syndromes per se.