While a great deal of attention has been devoted to racial and ethnic health disparities, health disparities in individuals disadvantaged by low income, lack of education, or employment (i.e., lower class) have been relatively neglected
(1) . Depression and anxiety disorders are known to be more prevalent in economically disadvantaged populations
(2 –
5), and impoverished depressed and anxious persons have demonstrated poor clinical outcomes in observational studies
(2,
4) . Despite these associations, little is known about outcomes of evidence-based care with poor and low-income individuals. Miranda and colleagues
(6) showed that both cognitive behavior therapy (CBT) and antidepressant medications (paroxetine or bupropion) were effective for treating poor minority women with depression who received extensive outreach and supportive services for attending care. A study of impoverished Chilean primary care patients with depression demonstrated that a collaborative care program designed to increase adherence to antidepressant pharmacotherapy improved outcomes
(7) . While both studies document the effectiveness of evidence-based interventions relative to usual care in poor populations, neither study included a comparison group of subjects with greater socioeconomic resources. In a secondary analysis of a large (43 primary care clinics) quality improvement study for depression (Partners in Care), the quality improvement interventions were found to produce significantly greater effects in Latino and African American patients than in Caucasian patients
(8) . Although the Latino patients tended to be poorer than the Caucasian patients, the impact of poverty per se on outcome was not examined.
We previously conducted a three-site primary care study (the Collaborative Care for Anxiety and Panic study) that demonstrated superior clinical effectiveness of a combined CBT and pharmacotherapy intervention relative to usual care for panic disorder patients in six university-based primary care clinics in three West Coast cities
(9,
10) . Because approximately one-third of this study group was at or below the federal poverty line and included significant numbers of impoverished Caucasian patients, this study provides an opportunity to examine the association between income and clinical outcomes without substantial confounding by ethnicity. Furthermore, because disadvantaged patients are more likely to seek care in medical as opposed to mental health specialty settings
(11), this study group and setting is especially appropriate for examining the effects of poverty. The purpose of this secondary post hoc analysis is to determine whether or not, and to what extent, economic disadvantage is associated with clinical outcomes when an evidence-based intervention for panic disorder is compared with treatment as usual. If poor subjects show less improvement than those who are not disadvantaged, it is likely that interventions tailored to the needs of this population will be required to optimize the effectiveness of these interventions. If poor subjects demonstrate a better or equal response, then specially tailored interventions are unlikely to be required.
Discussion
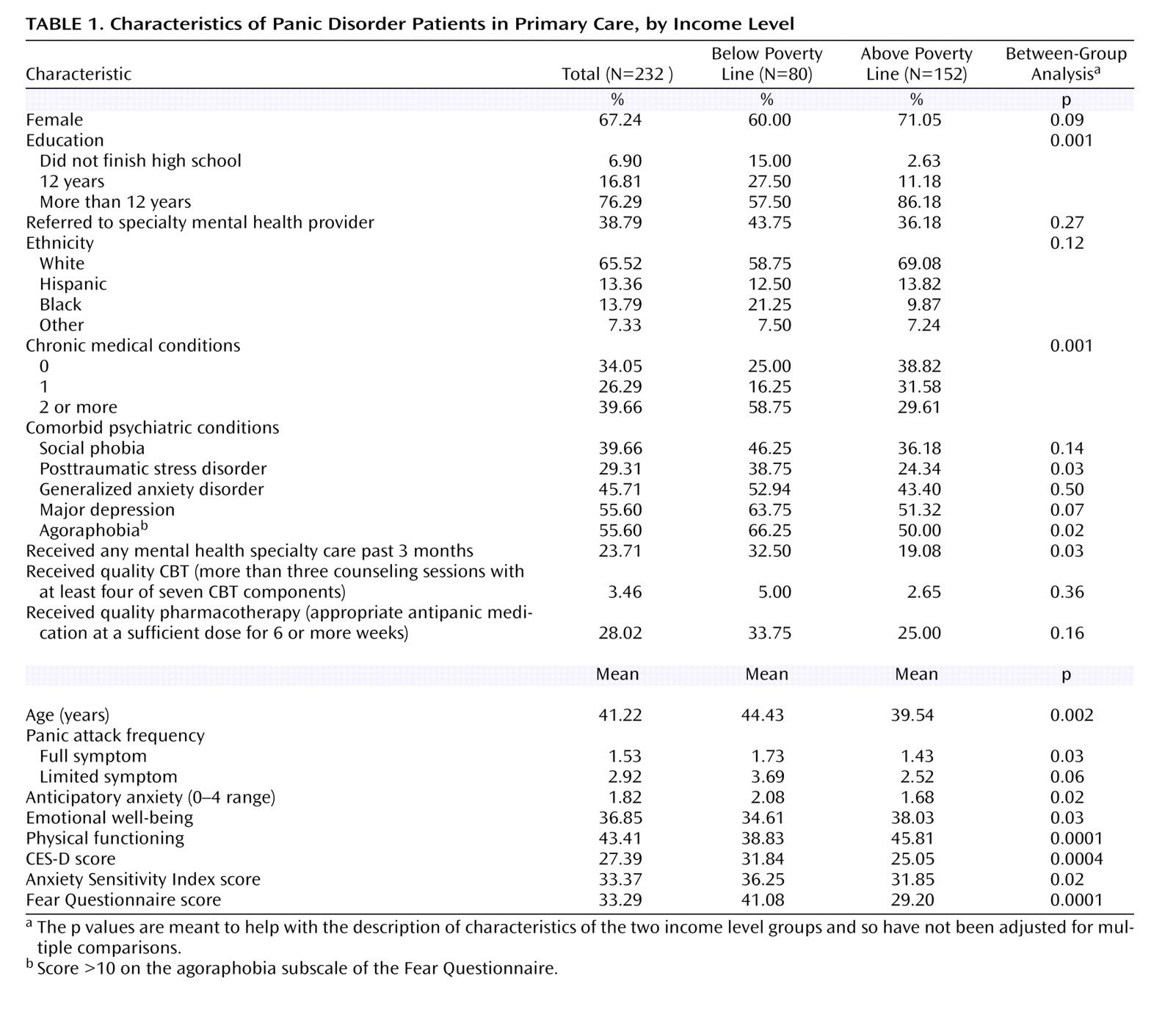
This analysis confirms prior findings that low-income psychiatric patients with depression and anxiety have more severe symptoms and functional disability associated with their illness
(2,
3,
5,
30) . Even after they receive clinically effective, carefully executed, evidence-based interventions their outcomes, because they start out more severely ill, lag behind those without economic disadvantage. At baseline, our panic disorder patients with incomes below the poverty line had more severe symptoms of panic, anxiety, and depression and also more severe chronic medical illness and associated physical disability. This may be related to the increased rate of stressful life events
(31,
32) and exposure to trauma
(33) in the poor, along with a relative lack of adequate resources to cope with these stressors
(34,
35) . This is also consistent with a previous study contrasting primary care panic patients from a public sector setting with panic disorder patients from more typical primary care settings
(30) . In that study, the low income and minority status of patients seeking care in the public sector setting accounted for the majority of clinical and functional differences (i.e., these differences disappeared when these variables were included as covariates) except for anxiety symptoms, which may have been affected by additional unmeasured factors related to the disadvantaged states of patients served in this setting (e.g., the chronic stress associated with dangerous neighborhoods and diminished social and material resources).
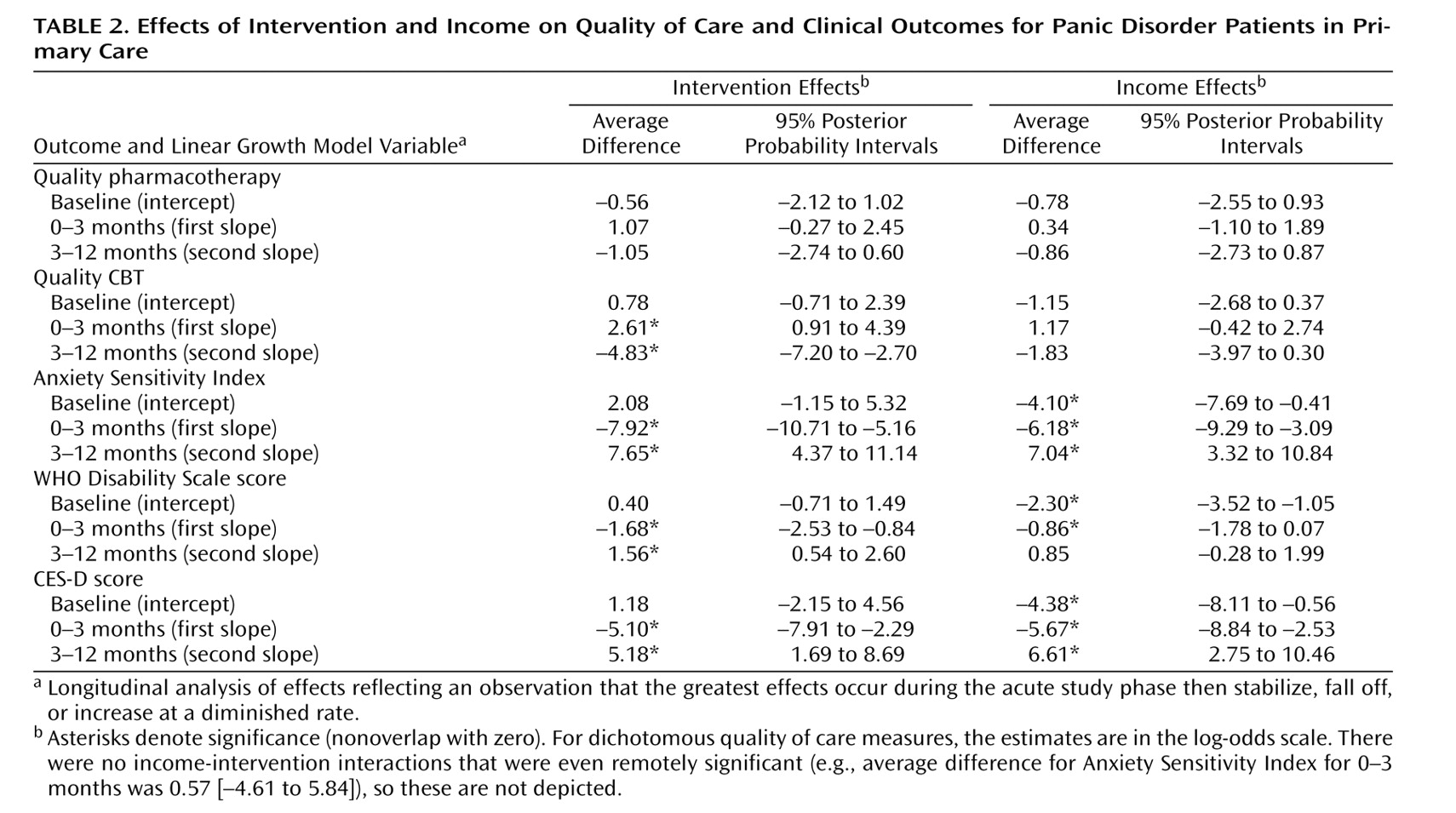
There were no differences in the effect of our intervention on quality of care in the two income groups. In both groups, the intervention successfully improved exposure to quality CBT during the first 3 months, when CBT sessions were offered to intervention patients. In contrast, the intervention failed to improve the proportion of patients receiving high-quality pharmacotherapy, with both intervention and usual care patients in both income groups increasing their exposure to quality pharmacotherapy during the study. It is possible that the nonmedical background of the behavioral health specialist—or the competing demands of both delivering CBT and trying to maximize medication use—may have led to less than optimal focus on or achievement of quality medication. It is also possible that patients were less motivated to pay for and maximize their use of medications when CBT was already improving their symptoms and was being provided free of charge.
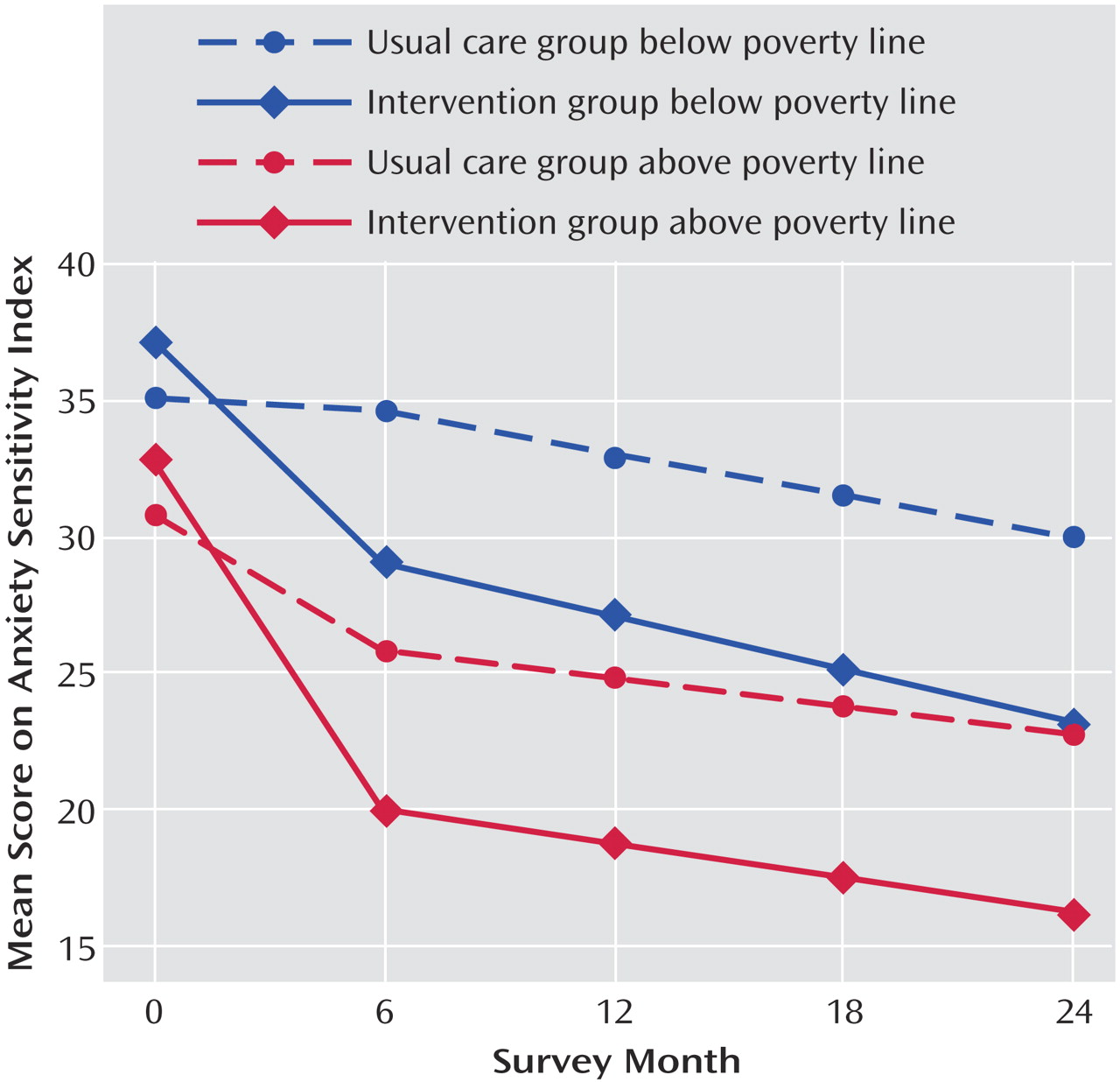
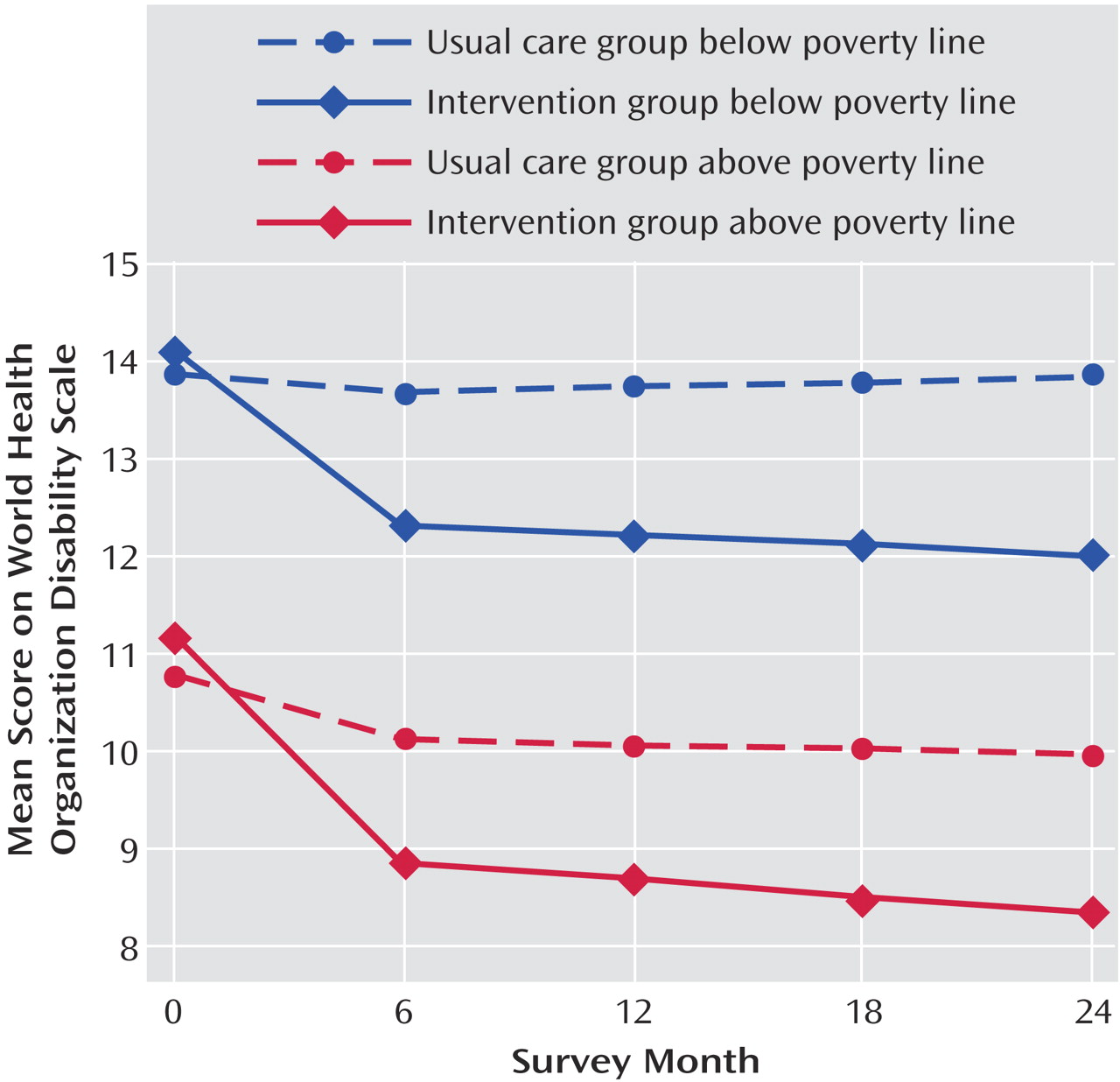
Finally, the intervention had equivalent effects on the various measures of clinical and functional outcome in the two income groups. Low-income patients started off with more severe symptoms and on average remained more symptomatic than patients above the poverty line, with both income groups showing greater improvement with the intervention relative to usual care. It is of interest that low income patients receiving the intervention were able to achieve a level of anxiety symptom reduction on the Anxiety Sensitivity Index comparable to higher income patients in the usual care group, suggesting that this intervention was able to eradicate the differences in illness severity that existed at baseline and also persisted across the combined group (intervention plus usual care) at 12 months.
Previous analysis from this dataset documented that more patients in the intervention group received CBT than in the usual care group, but that delivery of high-quality pharmacotherapy was not different in the two groups
(10) . CBT appeared to be the active ingredient in the intervention. The current analysis, demonstrating similar intervention response in subjects above and below the poverty line, suggests that CBT as an intervention for panic disorder works equally well in poor people. Thus, we do not think that this intervention needs to be modified or specially “tailored” for this population, even if these individuals may be less well educated. This is consistent with recent studies showing that CBT can be effectively delivered to anxiety disorder patients in low income settings
(36) and to low income panic disorder patients of African American ethnicity
(37), although none of these studies included an inactive treatment control group so that magnitude of treatment response could be compared. It is also consistent with studies documenting an expected level of response to evidence-based mental health treatments in disadvantaged depressed patients
(6,
7) . Unlike the Partners in Care study, where depressed minority patients (many of them quite poor) improved more than depressed Caucasian patients (most of whom were not poor), our poor patients appeared to respond equally to our more economically advantaged patients. This may be because, unlike that study, our poor patients’ rate of receiving care at baseline was comparable to, rather than lower than, the comparison group. It should be noted, however, that our power to detect an income-intervention interaction, which is estimated in this study to be quite small, is extremely low and would require a much larger sample size. It would not appear, however, that this estimated small effect would likely be clinically significant.
In conclusion, this analysis showed that impoverished patients with panic disorder responded equally well to an intervention designed to increase rates of quality antipanic pharmacotherapy and CBT. Because these patients began with more severe symptoms and disability, they ended up after treatment with less complete responses (i.e., a higher level of residual symptoms) than patients above the poverty line who started off with less severe symptoms. Their greater rate of comorbid psychiatric and medical conditions also likely contributed to this. This suggests that although CBT worked equally well in this impoverished population, helping these initially more ill patients achieve more complete resolution of their symptoms and functional deficits will require more intensive treatment, characterized either by greater amounts and frequency of the same treatment or perhaps additional “stepped-care,” which would deliver either adjunctive medications or behavioral treatments targeted toward both residual symptoms and additional comorbid conditions that may be contributing to disability. This hypothesis should be tested in future controlled studies.