Up to 30% of patients with major depression fail to respond to conventional treatments
(1–
4). Antipsychotic agents may exhibit antidepressant activity, either alone or in combination with an antidepressant
(5), particularly in depression with psychotic features
(6–
9). However, wide-scale application of augmentation with typical antipsychotics has been largely precluded by the high risk of extrapyramidal symptoms and/or tardive dyskinesia
(10,
11). In contrast, novel antipsychotic agents such as olanzapine exhibit a substantially lower risk of extrapyramidal symptoms
(12) and tardive dyskinesia
(13).
To our knowledge, there are no controlled trials of atypical antipsychotics in patients with treatment-resistant, nonpsychotic unipolar depression. We conducted a randomized double-blind trial to assess the efficacy and safety of olanzapine combined with the selective serotonin reuptake inhibitor (SSRI) fluoxetine versus either agent alone in subjects diagnosed with recurrent major depressive disorder (nonbipolar) without psychotic features who were unresponsive to conventional antidepressant therapy.
Method
Written informed consent was obtained from all participants. The study was conducted between April 1997 and June 1998 in outpatients who met DSM-IV criteria for recurrent major depression without psychotic features and were resistant to conventional antidepressant pharmacotherapy. Patients with a history of psychosis, dysthymic disorder, or bipolar disorder were excluded. Treatment resistance was defined retrospectively by history of failure to respond to antidepressants of two different classes, one of which was not an SSRI, after at least 4 weeks of therapy at an acceptable therapeutic dose. Failure to respond was confirmed prospectively during a screening period in which fluoxetine was given. At entry, patients were required to score ≥20 on the 21-item Hamilton Depression Rating Scale
(14).
The investigation consisted of three phases. The first was a 6-week open-label screening phase in which fluoxetine was given in escalating doses. Patients were titrated from an initial fluoxetine dose of 20 mg/day to the maximum tolerable dose, up to 60 mg/day. The second phase was an 8-week double-blind trial in which nonresponders to fluoxetine were randomly assigned in a 1:1:1 ratio to receive olanzapine plus placebo (“olanzapine”), fluoxetine plus placebo (“fluoxetine”), or olanzapine plus fluoxetine (“combination”). Patients in the olanzapine group discontinued fluoxetine on the day of random assignment. For all other patients, the fluoxetine dose received 1 week before random assignment remained unchanged throughout the double-blind period. For patients receiving olanzapine, the initial dose was 5 mg/day, titrated weekly within a range of 5–20 mg/day on the basis of response and tolerability.
The final study period was an 8-week open-label extension of olanzapine plus fluoxetine therapy. Only patients who successfully completed the double-blind phase were eligible to enter the open-label phase. Initial doses and subsequent titrations of olanzapine and fluoxetine were identical to those in the acute phase and were made at the investigators’ discretion. Analyses were performed on an intent-to-treat basis
(15). Repeated measures analysis of variance was used to assess mean change from baseline, while the last observation carried forward was used to analyze weekly visits. All significance tests were performed at a two-tailed alpha level of 0.016, incorporating a Bonferroni correction for multiple comparisons.
Results
Thirty-four patients entered the open-label screening period with fluoxetine treatment. One subject responded during the screening; five others dropped out during the study (three for protocol violations and one for lack of efficacy; one was lost to follow-up). There were no significant differences between the three treatment groups on baseline depression ratings or demographic characteristics (age, gender, or ethnic origin) before random assignment. The majority of the 28 patients randomly assigned to double-blind therapy were women (75%) and white (96%). The mean age was 42 years (SD=11).
During double-blind therapy, the mean modal dose of fluoxetine was 52.0 mg/day for both the monotherapy and combination groups (SD=14.0 and SD=10.3, respectively). The mean modal dose of olanzapine was 12.5 mg/day (SD=5.3) and 13.5 mg/day (SD=4.1) for the monotherapy and combination groups, respectively.
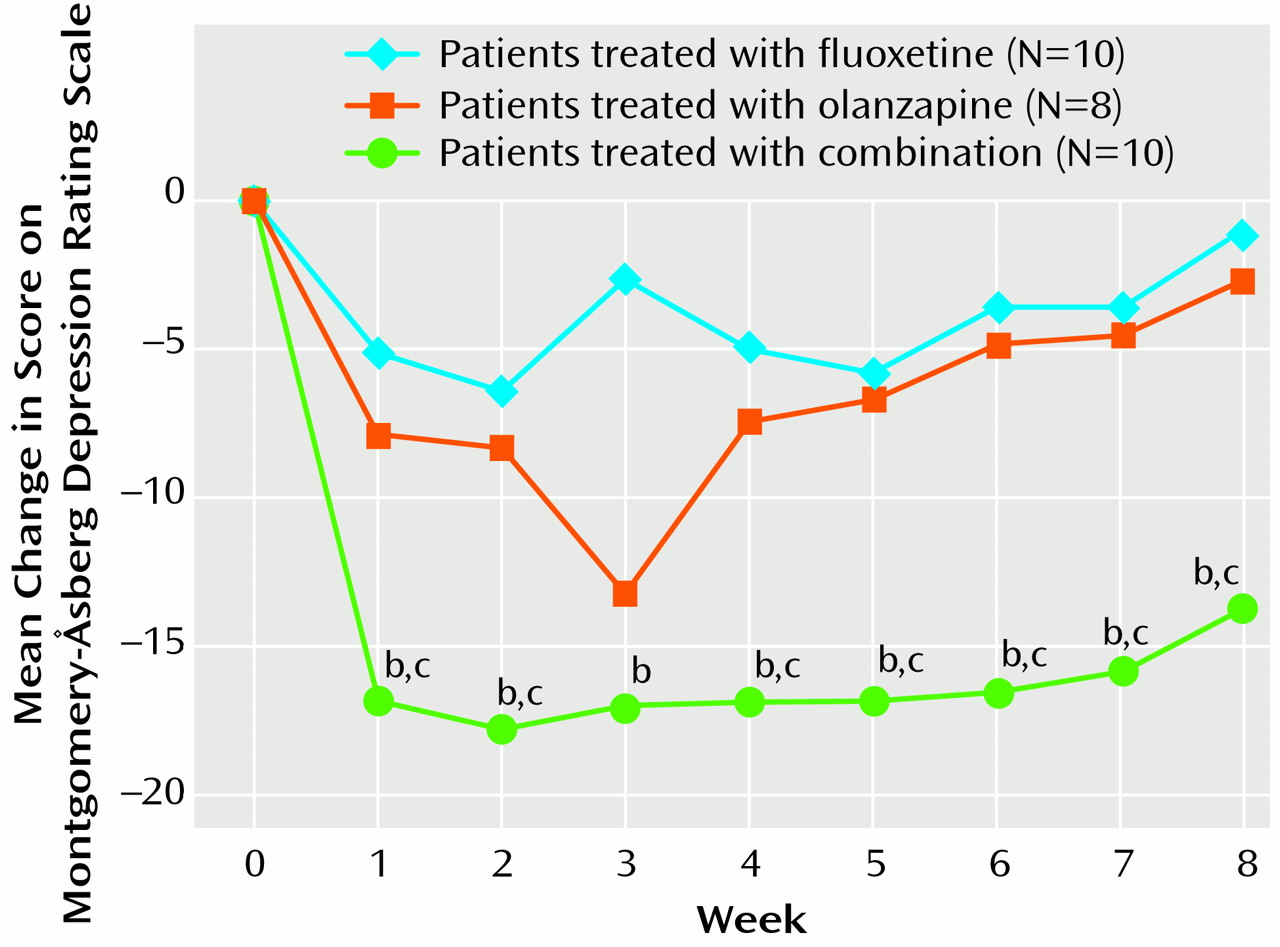
The combination group (N=10) achieved greater improvement from baseline on the Montgomery-Åsberg Depression Rating Scale
(16) than either monotherapy group (combination, –13.6) (olanzapine, –2.8; pair-wise F=2.22, df=8, 176, p=0.03) (fluoxetine, –1.2; pair-wise F=2.78, df=8, 176, p=0.006) on the basis of a repeated measures analysis with independent variables of therapy (F=1.46, df=2, 25, p=0.25), time (F=9.55, df=8, 176, p=0.001), and therapy-by-time (F=2.41, df=16, 176, p=0.003). Improvement was also greater with olanzapine plus fluoxetine on the Hamilton depression scale total score
(14) than with olanzapine monotherapy but not significantly greater than with fluoxetine monotherapy (combination, –11.7) (olanzapine, –5.9; pair-wise F=2.23, df=8, 176, p=0.03) (fluoxetine, –3.8; pair-wise F=1.87, df=8, 176, p=0.07) on the basis of a repeated measures analysis with independent variables of therapy (F=1.52, df=2, 25, p=0.24), time (F=13.60, df=8, 176, p=0.001), and therapy-by-time (F=2.26, df=16, 176, p=0.005).
Finally, the combination group achieved significantly greater improvement from baseline than the olanzapine monotherapy group, but not the fluoxetine group, on the severity of depression subscale of the CGI
(17) (combination, –2.0) (olanzapine, –0.0; pair-wise F=2.63, df=8, 174, p=0.01) (fluoxetine, –0.4; pair-wise F=0.94, df=8, 174, p=0.48) on the basis of a repeated measures analysis with the independent variables of therapy (F=3.72, df=2, 25, p=0.04), time (F=3.29, df=8, 174, p=0.002), and therapy-by-time (F=1.74, df=16, 174, p=0.04).
The proportion of patients noted as responding (≥50% improvement) on the Montgomery-Åsberg Depression Rating Scale was significantly greater for the combination group (N=6, 60%; global Fisher’s p=0.007) than for the olanzapine group (N=0, 0%; pair-wise, Bonferroni-adjusted Fisher’s p=0.03) but not for the fluoxetine group (N=1, 10%; pair-wise, Bonferroni-adjusted Fisher’s p=0.11). Significant last-observation-carried-forward differences between the combination and the fluoxetine monotherapy groups were evident by week 1 of double-blind therapy on all three scales (
Figure 1). The significant response of the combination group (N=9) was maintained throughout the 8-week open-label extension period on all three measures. However, patients receiving monotherapy (olanzapine=6, fluoxetine=7) during the double-blind phase did not improve significantly during open-label combination treatment.
Both drugs were well tolerated either alone or in combination. During double-blind therapy, one patient in the olanzapine group discontinued treatment because of an adverse event (ataxia). Completion rates were high (combination, N=9, 90%; fluoxetine, N=7, 70%; olanzapine, N=6, 75%). The most frequently reported significant adverse events included somnolence, increased appetite, asthenia, weight gain, headache, dry mouth, and nervousness. Of these, both increased appetite and weight gain occurred significantly more frequently among patients treated with olanzapine (both as monotherapy and in combination). No clinically significant changes in vital signs or laboratory analytes were found among treatment groups, nor were there significant differences in the incidence of extrapyramidal symptoms. Mean weight increases from baseline to endpoint were 0.88 kg (SD=1.33; N=10, p=0.06, Wilcoxon’s signed rank test), 6.07 kg (SD=2.57; N=8, p=0.008, Wilcoxon’s signed rank test), and 6.67 kg (SD=4.54; N=10, p=0.002, Wilcoxon’s signed rank test) for the fluoxetine, olanzapine, and combination groups, respectively. A total of 27 (96.4%) of the patients completed the open-label extension phase of the trial. One patient dropped out of the study because of fever secondary to infection.
Discussion
In the present study, the combination of olanzapine with fluoxetine in patients with treatment-resistant, nonpsychotic, unipolar depression produced superior improvements over either agent alone across a variety of measures. Clinical responses were evident by the first week, suggesting rapid onset of action. Overall, the three treatments were well tolerated. For example, 9 (90%) of the patients receiving olanzapine plus fluoxetine completed double-blind therapy. The rates of extrapyramidal symptoms did not differ significantly between treatment groups. Previous long-term observations of olanzapine treatment suggest a significantly lower risk of tardive dyskinesia than with haloperidol
(13). Although the observation period in the present study was short, the absence of acute extrapyramidal symptoms (which may predict a risk for subsequent tardive dyskinesia) was encouraging. In this study, one treatment-emergent event among patients treated with olanzapine, both in monotherapy and in combination with fluoxetine, was weight gain, averaging more than 6 kg over the double-blind treatment period. Combined olanzapine and fluoxetine appears to be an effective and well-tolerated treatment for treatment-resistant depression.
In contrast with the significant response observed with the combined therapy, neither fluoxetine nor olanzapine alone was effective in this resistant population. It therefore appears that neither the serotonin reuptake blockade of fluoxetine nor the pleiotropic receptor effects of olanzapine
(18,
19) individually were beneficial in treating resistant depression. Concomitant administration of fluoxetine and olanzapine results in a small increase in olanzapine maximum concentration and area under the curve, zero to infinity, and a small decrease in olanzapine plasma clearance (unpublished work by Gossen et al.). Such changes, although statistically significant, are small in comparison to the overall variability between individuals and are unlikely to result in a clinically significant pharmacokinetic interaction.
Alternatively, combined administration likely introduces a pharmacodynamic synergy. Zhang and colleagues
(20) demonstrated that 3 hours after administration of olanzapine, norepinephrine and dopamine concentrations in the rat prefrontal cortex returned to baseline values. With fluoxetine treatment, norepinephrine and dopamine levels increase to 188% and 143% of baseline values, respectively. However, when both drugs are given, norepinephrine and dopamine levels increase to 269% and 349% of baseline values, respectively. This suggests a neurochemical basis for the synergistic antidepressant effect observed in the present trial. The prefrontal cortex is rich in mesocorticolimbic dopamine innervation
(21–
23). Coupled with the well-chronicled role of norepinephrine in mood states
(24), this suggests potential targets for treating resistant depression.
The antidepressant efficacy observed in the current study with the combined administration of olanzapine and fluoxetine is intriguing. The robust effect size and rapid onset of action suggest promise for this approach. Because of the small group size, these results should be considered preliminary. Nevertheless, considering the public health impact of treatment-resistant depression, these results and future treatment alternatives should be welcomed. To this end, we are currently conducting studies to investigate further the efficacy and safety of combined olanzapine and fluoxetine in the treatment of patients with refractory depression.