Life satisfaction is one of the indicators of subjective well-being
(1). It has been conceptualized as an assessment of life as a whole on the basis of the fit between personal goals and achievements
(2,
3). It has also been viewed as a dimension of mental health
(4). Indeed, many of its correlates—such as depressive symptoms, self-esteem, anxiety, and psychosomatic symptoms
(4–
6)—are aspects of mental health, but life satisfaction is also associated with diagnosed mental disease and health risk factors, including poor health behavior and poor social support
(7). Thus, life satisfaction is a broad and nonspecific subjective perception comparable to self-rated health—another of its correlates. Both have proven to be predictors of mortality
(8,
9), but level of life satisfaction is a particularly effective predictor of psychiatric morbidity
(7). It is not surprising that life dissatisfaction is much more common in psychiatric patients than in the general population
(7,
9) regardless of the level of psychopathology
(6,
10).
Suicide is a major health problem that has been linked to several risk factors but most notably to diagnosed mental disorders, especially affective disorders
(11–
13). The lifetime suicide risk in patients with affective disorders has been estimated to be 6%
(14), and patients with major depression and dysthymia have been shown to have suicide risks that are 20 and 12 times greater, respectively, than would be expected
(15). Furthermore, depression, even subthreshold depression, may have a deleterious course that results in several poor health outcomes, including poorer self-rated health and poor physical and psychosocial functioning
(16–
19).
A diagnosis-based approach to suicide prevention is often possible only for a short period before suicidal behavior is exhibited, and only a portion of the suicide candidates are reached by this method. Thus, suicide prevention approaches need to pay attention to other risk factors or indicators for higher suicide risk. Easily administered indicators would be particularly valuable.
We studied the effect of self-reported life satisfaction on the risk of suicide during a 20-year follow-up of adults who were 18–64 years of age at the start of the study. The effects of health status, gender, health behavior, and social situation on this relationship were also examined.
Method
This prospective cohort study was based on the Finnish Twin Cohort and consisted of a nationwide sample of all Finnish adult same-sex twin pairs born before 1958 and with both members alive in 1975. Twin candidates were identified from the Central Population Registry in 1974
(20). In the autumn of 1975, a postal questionnaire was sent, with up to three reminders, to all twin candidates, i.e., sets of persons with the same community of birth, surname at birth, date of birth, and same sex. Thus, some singletons who satisfied the selection criteria were included. The aim of the project was to study environmental, psychosocial, and genetic factors that affected public health problems. The questionnaire included information on psychosocial and health-related factors and a life satisfaction scale. After complete description of the study to the subjects, written informed consent was obtained. Virtually all responses were received by April 1976. The response rate for all those aged 18–64 in 1975 was 84%, higher (89%) for the twins. Subjects in a twin candidate pair were not sent a reminder if it became known that they were not biological twins. Follow-up postal inquiries were sent to the twins in 1981 and 1990.
Self-reported life satisfaction was measured by a four-item scale
(21) modified from quality-of-life studies
(2,
3). Subjects were asked to rate on a 5-point Likert scale four aspects of life satisfaction: interest in life (1=very interesting, 5=very boring), happiness (1=very happy, 5=very sad), ease of living (1=very easy, 5=very hard), and feeling of loneliness (4-point scale: 1=not at all lonely, 4=fairly lonely, and 5=very lonely).
Responses of “cannot say” and all missing data were scored as 3. Thus, the range of possible total life satisfaction scores was 4–20, with higher scores indicating greater dissatisfaction. If a response was missing for three or four items, the life satisfaction score was recorded as missing data. All four questions concerning life satisfaction were answered by 98.17% (N=28,906 of 29,444) of the respondents and at least two questions by 99.08% (N=29,173). Cronbach’s alpha
(22) was 0.74. Distribution of life satisfaction scores was skewed, with lower scores (i.e., higher life satisfaction) predominating (mean score=8.76 [SD=2.93], median=8, mode=7). On the basis of their life satisfaction score, subjects were classified into groups as being satisfied (score=4–6) or dissatisfied (score=12–20), with the intermediate group consisting of subjects whose life satisfaction score was within one standard deviation of the mean
(7).
The life satisfaction scale has been used in Nordic countries
(21) for the general adult population
(7,
9) as well as for psychiatric patients
(6,
10). Life satisfaction has been associated with health, health behavior, social situation, and personality features
(7,
23–
26) and has been strongly associated with depressive symptoms
(27). In psychiatric patients, score on the Beck Depression Inventory alone accounted for 48% of the variation in life satisfaction score
(6). In 1990, when both scores were available in a subsample of the Finnish Twin Cohort (N=12,063, aged 33–60), a highly significant correlation between life satisfaction score and Beck Depression Inventory score was reported (r=0.61, df=12,061, p<0.001). Over 97% of those who were satisfied had a Beck Depression Inventory score of <10, indicating normal mood; of those with at least moderate depression (Beck Depression Inventory score >18), nearly 83% were dissatisfied. More detailed information concerning the scale has been presented elsewhere
(7,
9).
Those eligible for the present study were aged 18–64 on January 1, 1976 (N=29,444), had a baseline life satisfaction score available (N=29,173), and were alive at the start of the follow-up period on May 1, 1976 (N=29,137). The study population consisted of 14,348 men and 14,789 women, of whom 4,224 were singletons and 24,913 twins. On the basis of life satisfaction score, 19% of the study population was “satisfied” (score=4–6), 18% “dissatisfied” (score=12–20), and 63% fell into the intermediate group (score=7–11).
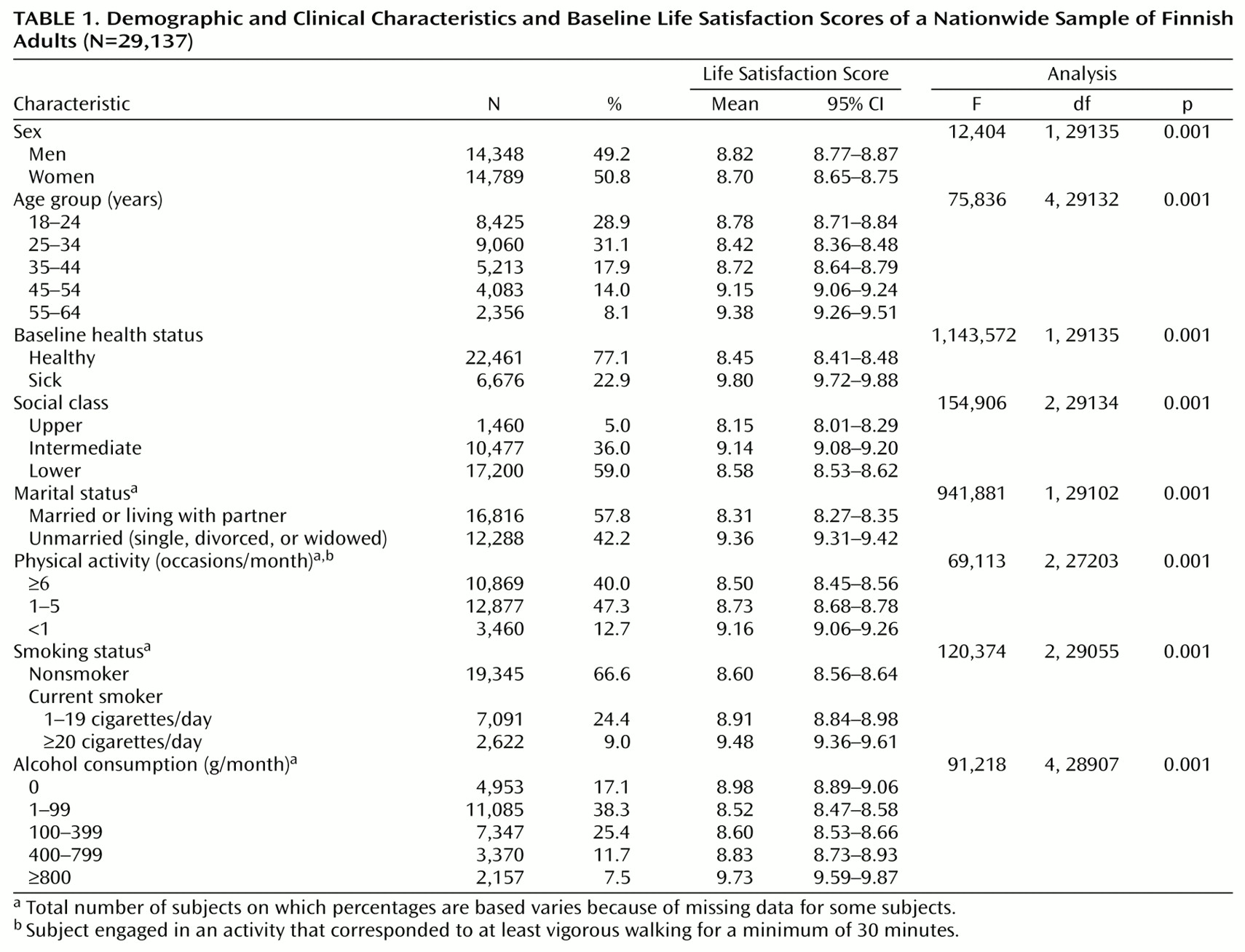
Age was broken down into a five-category variable for the analyses (
Table 1). Marital status was classified as either living with a partner or alone (single/divorced/widowed). Social class was a three-category variable: upper was defined as having at least 13 years of education (high school graduates with ≥1 year of vocational training/university education) and sedentary work, and the lower group was defined as having no more than 9 years of education (primary school) and work involving at least standing and walking
(26); the remaining subjects were placed in an intermediate group. Physical activity during leisure time was defined as the number of times per month the subject engaged in an activity that corresponded to at least vigorous walking for at least 30 minutes
(28). Smoking status
(29) and alcohol consumption (which was converted into grams of absolute alcohol per month
[30]) were broken down into three and five categories, respectively (
Table 1).
Individuals were considered to be ill at baseline if one or more of the following were present: 1) a history or symptoms of cardiovascular disease or diabetes as determined through standard questioning
(31,
32); 2) use of hypnotics or tranquilizers for more than 10 days in the preceding year; 3) receipt of work disability pension due to any cause; 4) inpatient admissions on record with the nationwide Hospital Discharge Registry
(33) between 1972 and April 30, 1976, for diabetes, cardiovascular diseases (except hypertension and venous diseases), chronic obstructive pulmonary diseases, or a psychiatric disorder; 5) receipt of free medication for 34 selected chronic diseases
(34) other than hypertension (including psychoses) before 1977 according to the nationwide Registry of Specially Refunded Medication; or 6) presence of incident malignant cancer before 1977 according to the Finnish Cancer Registry
(35).
The national registries used in this study are based on the unique personal identification code assigned to each Finnish citizen and have a high coverage and diagnostic accuracy
(33). In addition, 99% of the psychotic persons in Finland have received psychiatric treatment
(36) and have a right to free medication. Furthermore, every adult citizen, regardless of former work status, is entitled to work disability pension if unable to work because of disease or injury.
The follow-up period extended from May 1, 1976, to December 31, 1995. Mortality data were derived from The National Registry for Cause of Death, which has 100% coverage
(37). The cause of death was classified according to ICD-8 for 1976–1986 and ICD-9 revision for 1987–1995. Suicide was defined according to the underlying cause of death (ICD codes: E950–E959). During the total follow-up period, 2,859 deaths (9.81%) occurred (1,847 men and 1,012 women). The total number of suicides was 182 (149 men and 33 women).
Data analyses were carried out by using SPSS (Chicago). The adjusted effects of life satisfaction on suicide were studied with Cox regression by comparing the proportional hazards of the dissatisfied subjects (life satisfaction score=12–20) to those of the satisfied (score=4–6).
Since 38.60% of the study subjects were age-matched siblings of another study subject, the assumption of independent observations was not strictly true. To assess the possible bias due to twinship, we randomly selected only one member of each twin pair for separate subanalyses with singletons. In addition, the association between life satisfaction and suicide was studied also in subsamples that included only singletons or twins.
Results
Mean age at baseline was 33.5 years (SD=11.9) for men and 34.0 years (SD=12.8) for women. Greater life satisfaction (i.e., lower baseline life satisfaction score) was associated with subjects who were female, healthy, married or living with a partner, physically active, nonsmokers, less than 45 years old, and in the upper social class (
Table 1). Less life satisfaction was associated with heavy drinking; this was true for both genders. The association between alcohol consumption and life satisfaction was j-shaped, which indicated a higher level of satisfaction with low or moderate alcohol consumption relative to that of both teetotalers and heavy drinkers.
The cumulative incidence of suicide over the 20-year follow-up period was 1.04% for men and 0.22% for women (rates of 56.9 and 11.8 per 100,000 person years, respectively). Suicide victims were significantly more likely to have been grouped in the dissatisfied category (31.87%) than were the other subjects (18.10%) (χ2=25.27, df=2, p<0.001). Significantly greater dissatisfaction was indicated by their higher mean life satisfaction scores (10.15, 95% confidence interval [CI]=9.63–10.66, versus 8.75, 95% CI=8.71–8.78; F=41.30, df=1, p<0.001). Suicide victims were also more likely to live alone (52.20% versus 42.20%; χ2=7.47, df=1, p<0.01), be heavy drinkers (22.53% versus 7.40%; χ2=85.65, df=4, p<0.001) and smokers (19.23% versus 9.00%; χ2=48,518, df=2, p<0.001), and be sick significantly more often (31.32% versus 22.90%; χ2=7.33, df=1, p<0.01); no difference in amount of physical activity was found.
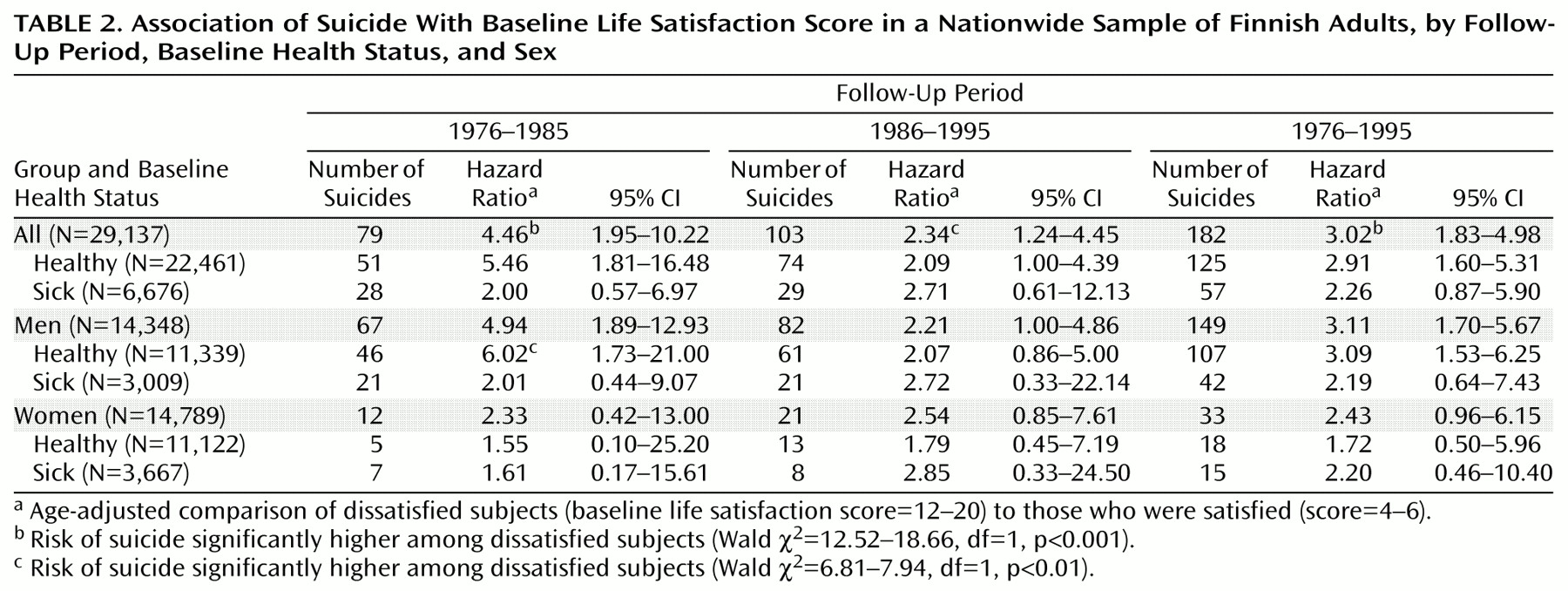
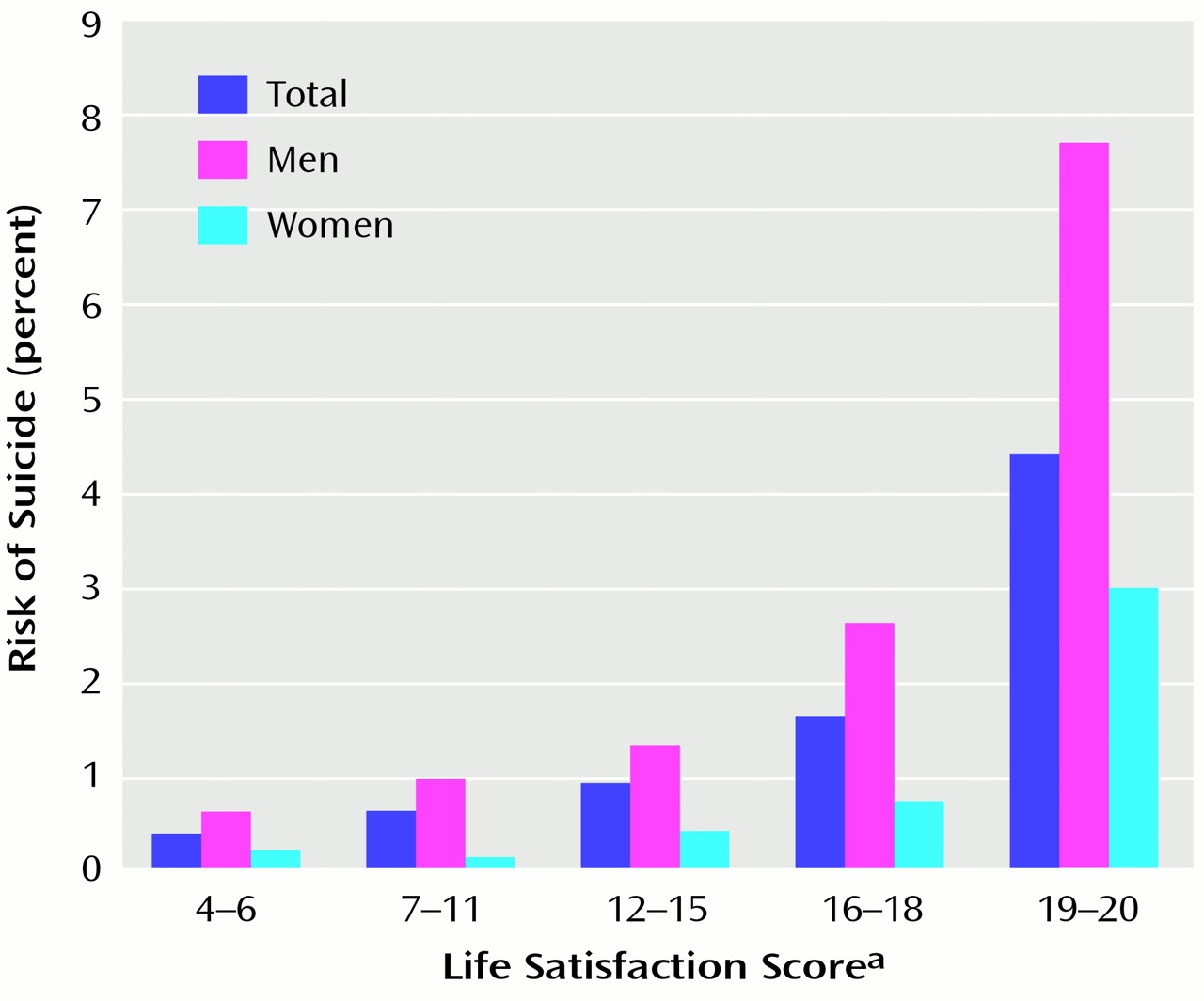
The age-adjusted risk of suicide was significantly higher among the dissatisfied (life satisfaction score=12–20) than the satisfied (score=4–6) throughout the 20-year follow-up period, being somewhat higher, although nonsignificantly so, in the first decade than in the second half of the follow-up (
Table 2). A dose-response relationship was also seen (
Figure 1). The most dissatisfied men (life satisfaction score=19–20) had a 24.85-fold higher risk of suicide (Wald χ
2=19.34, df=1, p<0.001) than the satisfied men during the first decade. Throughout the entire follow-up, these highly dissatisfied men had a 14.41-fold higher risk (Wald χ
2=26.21, df=1, p<0.001), with 7.70% of them committing suicide. The association between life satisfaction and suicide was especially strong among healthy men during the first decade (
Table 2).
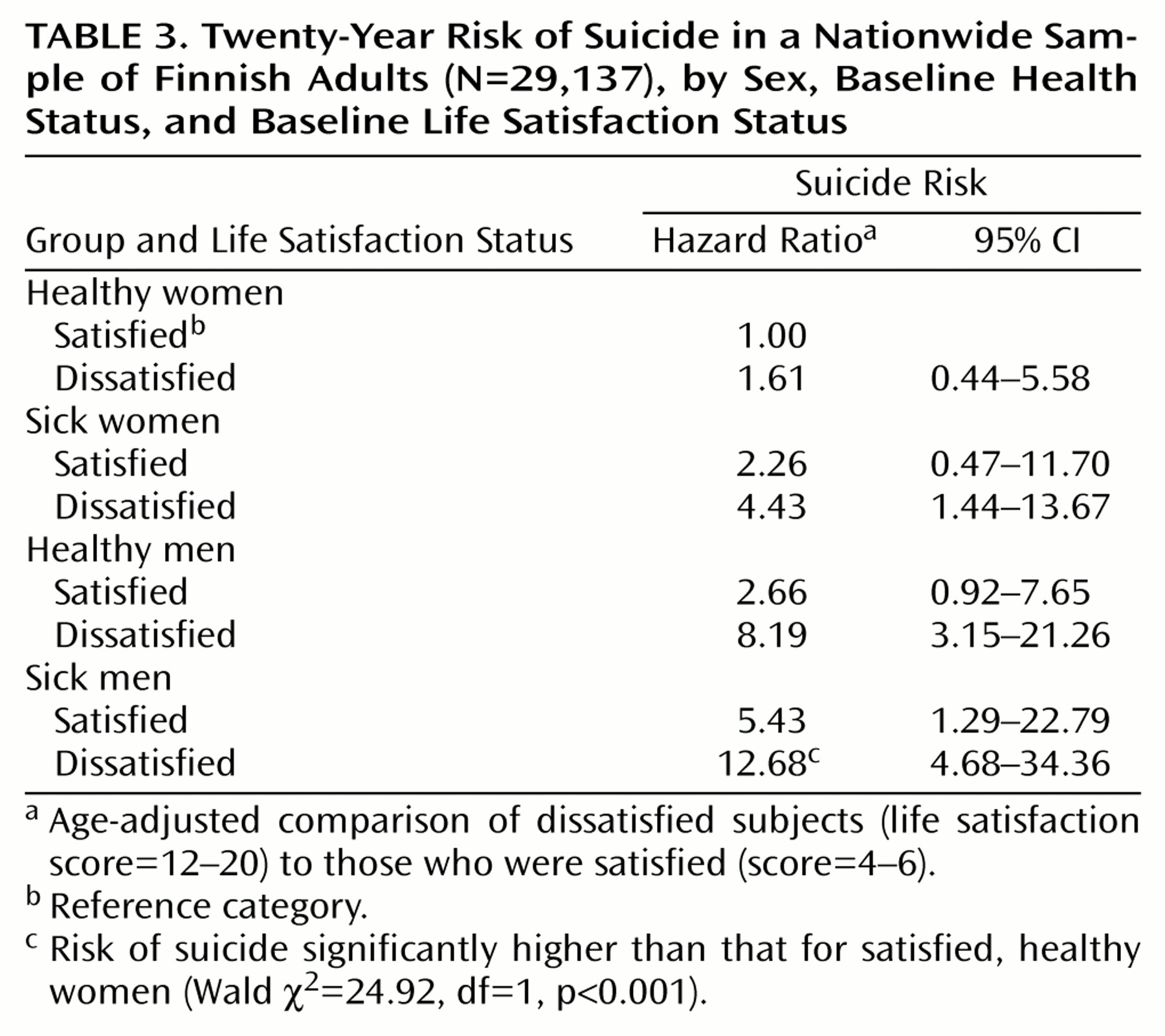
Baseline life satisfaction score was associated with risk of suicide regardless of baseline health status and gender. However, the dissatisfied sick men were at much higher risk of suicide than the satisfied, healthy women throughout the follow-up period (
Table 3). This higher risk was most prominent during the first half of the follow-up (hazard ratio=38.05, 95% CI=4.88–296.58; Wald χ
2=12.06, df=1, p<0.001). For men, being dissatisfied increased the risk of suicide more than being sick, whereas the opposite was the case for women.
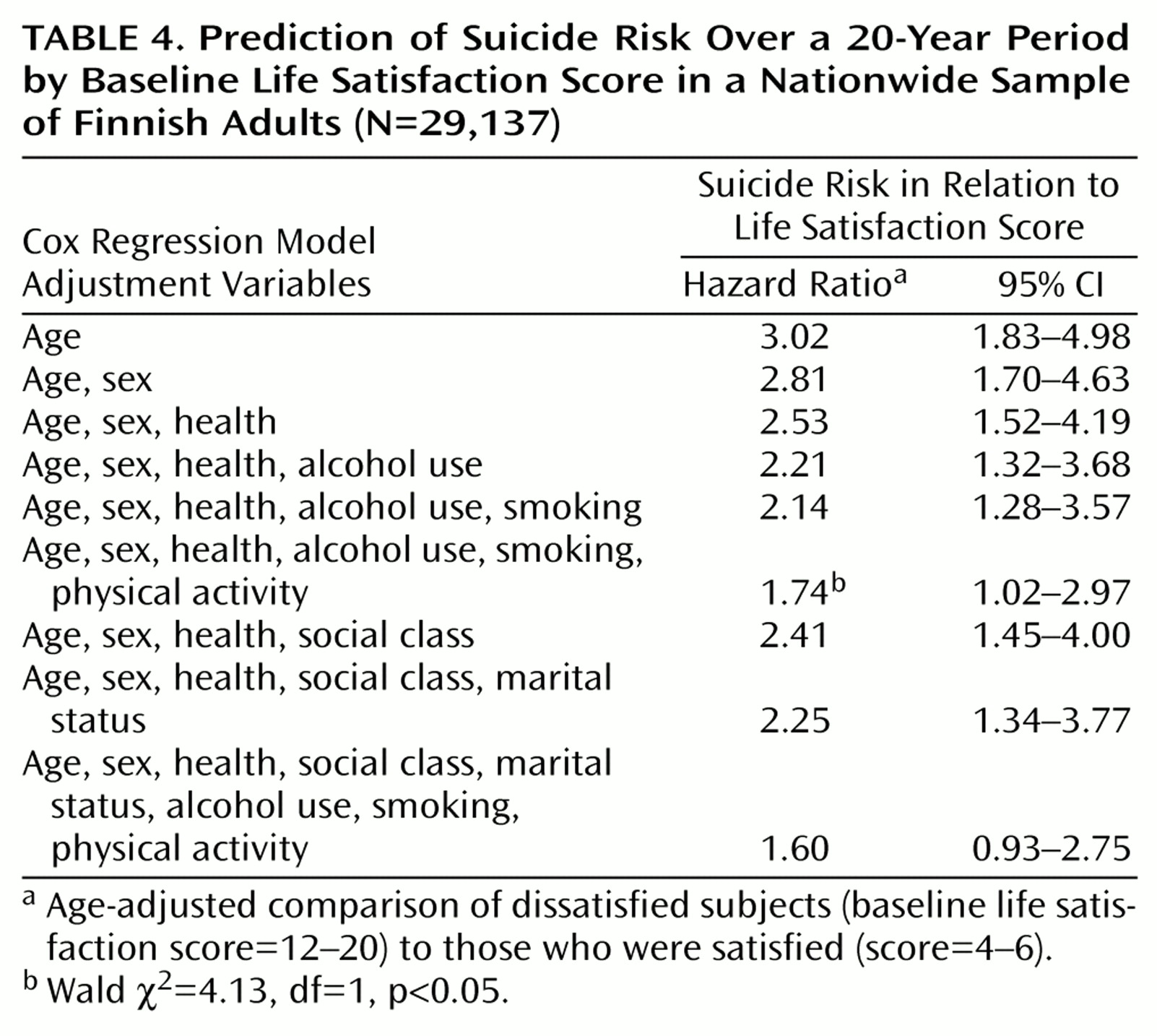
Throughout the follow-up period, when age, sex, baseline health, smoking status, physical activity, and alcohol consumption were controlled, life dissatisfaction still predicted suicide (
Table 4). Social class and marital status modified the effect of dissatisfaction less than health behavior. When all these variables were simultaneously controlled, life dissatisfaction lost its independent power to predict suicide.
There was an elevated risk of suicide among the dissatisfied subjects compared to the satisfied subjects regardless of status as a twin or a singleton (monozygotic twins: 30 suicides out of 7,134 subjects, hazard ratio=3.00 [95% CI=0.93–9.62], Wald χ2=3.41, df=1, p<0.07; dizygotic twins: 115 suicides out of 15,850 subjects, hazard ratio=3.02 [95% CI=1.56–5.84], Wald χ2=10.76, df=1, p=0.001; singletons: 23 suicides out of 4,200 subjects, hazard ratio=2.53 [95% CI=0.77–8.30], Wald χ2=2.36, df=1, p<0.13). Suicide risk remained elevated when the study group consisted of only one randomly selected member of each twin pair (87 suicides out of 13,548 subjects, hazard ratio=3.40 [95% CI=1.53–7.53], Wald χ2=9.08, df=1, p<0.01) as well as when singletons were included (104 suicides out of 16,658 subjects, hazard ratio=3.12 [95% CI=1.57–6.20], Wald χ2=10.59, df=1, p=0.001).
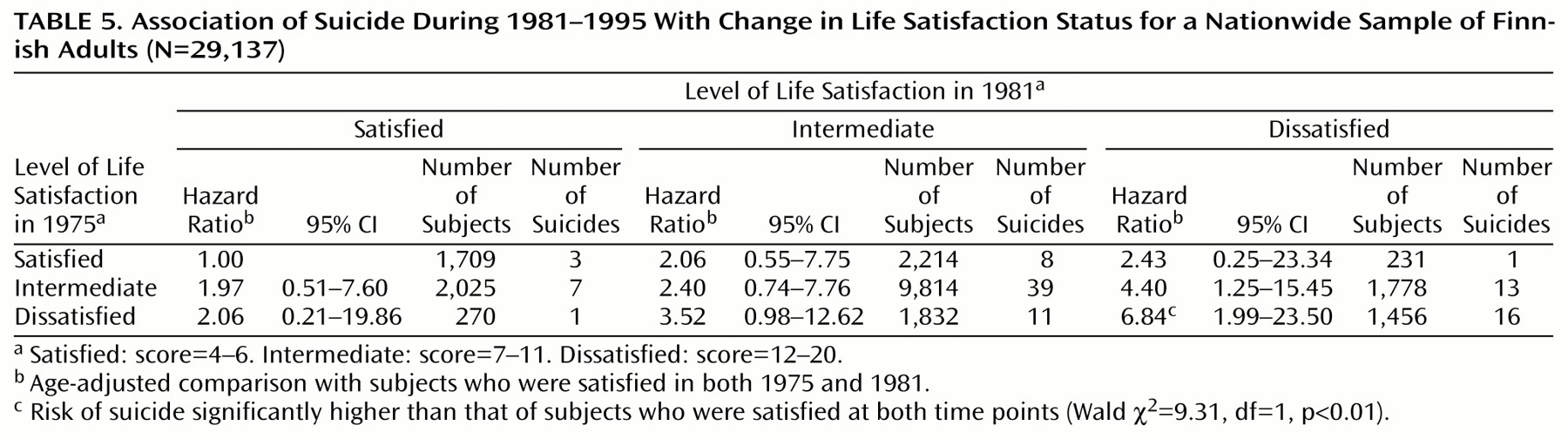
Among twins whose life satisfaction scores were available both in 1976 and 1981 (N=21,329), life satisfaction score was quite stable: 2.3% of them changed from being satisfied (score=4–6) to being dissatisfied (score=12–20) or vice versa, while 60.8% remained in the same life satisfaction score category. Compared to those who were satisfied in both years, the age-adjusted risk of suicide during 1981–1995 was significantly higher for those who remained dissatisfied (
Table 5).
Discussion
This was a long-term prospective study of the association between self-reported life satisfaction and suicide. Life satisfaction was measured with an easily administered, four-item scale that assessed happiness, ease of living, interest in life, and feeling of loneliness. Given the low frequency of missing data, the items seemed to be well understood by and acceptable to the subjects. The main result was that life dissatisfaction was associated with a higher risk of suicide throughout the 20-year follow-up period.
Suicide is a major public health problem in Finland; men are especially at high risk. In 1995, suicide rates were 53.2/100,000 per year for men and 11.5/100,000 per year for women
(38), with which our results are in good agreement. This lends support to the generalizations from our study. The mortality among twins and the general population has been reported to be similar
(39). In our study, subanalyses on twins, singletons, or sole independent observations did not affect the results. Thus, twinship seemed not to bias our results.
Other strengths of this study include a large nationwide sample with high response rate and long follow-up time. The criteria of ill health were comprehensive and based both on self-reports and several national registries with high coverage and validity. This enabled us to examine the effect of life satisfaction for both the healthy and the sick. Also, the effect of change in life satisfaction on risk of suicide could be studied. However, a study limitation was that information on health behavior consisted of self-reports that were based only on baseline situation.
The sick category included somatic and mental disorders as well as those who used only minimal amounts of psychotropic medication. The healthy category may have included a few individuals currently undergoing psychiatric treatment but without previous hospitalization or medication, while the vast majority were not receiving any psychiatric treatment. Still, among them dissatisfaction was also associated with a prominently greater risk of suicide. Thus, self-reported life satisfaction seems to provide information on mental health of a group that would otherwise have remained unnoticed.
Several mechanisms might explain the association between life satisfaction and suicide. Stability of subjective well-being and life satisfaction has been previously reported
(9,
40,
41) and was found also in this study. The long-term effect of life satisfaction on risk of suicide suggests that it may be related to personality. Still, improved life satisfaction or improved ability to cope with stress and dissatisfaction over time or early suicide of those at highest risk might explain partly the decreasing risk in the second decade of the follow-up period. A better ability to cope might also explain the weaker association between suicide and life satisfaction among women, who have shown to react to life dissatisfaction with impaired work ability
(25) rather than with increased mortality
(7,
9). This may also be partly supported by the finding that hostile men but not women were at a higher risk of suicide
(42). However, the small number of female suicides prevents definitive conclusions.
Life satisfaction is strongly associated with depressive symptoms as measured by the Beck Depression Inventory
(6,
9,
10). Therefore, our results could also reflect the known association between depression and suicide
(15). Still, undiagnosed depression is one of the main obstacles to suicide prevention. The assessment of life satisfaction could, in part, promote the early identification of depressive persons who have not necessarily been in reach of psychiatric evaluation.
More generally, life dissatisfaction might be an early sign of future mental problems or a device to detect an already existing one
(7). It may manifest as nonoptimal health behavior or social relations, supporting the notion that risk factors for suicide may accumulate over a lifetime
(43).