Subjects
Twenty-nine patients with schizophrenia (23 men and six women; mean age=34.6 years, SD=11.0) and 29 normal subjects (20 men and nine women; mean age=36.7 years, SD=11.5) participated in the study. Patients and comparison subjects were naive about the purpose of the study procedure. This study was approved by the local ethics committee (Comité Consultatif de Protection des Personnes se Prétant à la Recherche Biomédicale, Centre Léon Bérard, Lyon). After a complete description of the study procedures, all participants provided written consent.
Patients who were selected for the study met the DSM-IV criteria for schizophrenia. None of the patients met criteria for additional diagnoses. Comparison subjects were recruited from the maintenance staff of two hospitals. Exclusion criteria in both groups were visual and auditory disorders, history of neurological illness or trauma, alcohol and drug dependence according to the DSM-IV criteria, and age older than 65 years or younger than 18 years. The patient and comparison groups did not differ significantly in age, sex, laterality, and educational level.
Seventeen of the 29 patients were hospitalized at the time of the study. Twelve patients met the criteria for the paranoid type of schizophrenia, three for the disorganized type, 11 for the undifferentiated type, and three for the residual type. All but three patients were right-handed, according to assessments made with the Edinburgh Inventory
(8). The mean disease duration was 11.3 years (SD=9.0, range=1–33). All patients were treated with antipsychotic medication (principally risperidone, olanzapine, clozapine, and levomepromazine) and were clinically stable at the time of testing. We could find no information in the literature on possible effects of medications on tasks similar to those used in the present work.
Neuropsychological tests, including the Birmingham Object Recognition Battery
(9) and Raven’s Coloured Progressive Matrices
(10), were used to assess patients’ spatial perception abilities and intellectual performance. The Birmingham Object Recognition Battery assesses the ability to process basic features of simple or geometric pictures. The patients’ mean scores on the six tests from the battery that were used in the study were within the normal range (line match test A score=26.7, compared with the cutoff score of 22 for the lower limit of the normal range; circle match test A score=26.7, compared with the cutoff of 19; line orientation match test A score=24.5, compared with the cutoff of 18; position of gap match test A score=34.7, compared with the cutoff of 24; minimal feature view task score=24.4, compared with the cutoff of 18.5; and item match task score=31.5, compared with the cutoff of 24). The Coloured Progressive Matrices examines the effectiveness of visuospatial reasoning and may detect low intellectual performance. The patients’ mean score on this test (mean=28.4, SD=2.3, range=24–31) was within the normal range for their age group
(11).
All patients underwent clinical assessment with the Scale for the Assessment of Positive Symptoms (SAPS)
(12) and the Scale for the Assessment of Negative Symptoms (SANS)
(13). Mean scores were 24.7 for the SAPS (SD=12.3, range=8–60) and 41.3 for the SANS (SD=19.9, range=6–85). In addition, a subscale for passivity phenomena, consisting of items 15–19 of the SAPS, was defined. This subscale allowed classification of the patients as having or not having delusions of influence. At the time of testing, six patients with a passivity phenomena subscale score greater than 2 (mean=6.3, SD=2.8, range=3–9) were classified as “influenced.” The remaining 23 patients, with scores of 2 or less on this subscale, were classified as “noninfluenced.” There were no differences between the two groups of patients in educational level, intellectual level, clinical features (SAPS and SANS total scores), and scores on five tests from the Birmingham Object Recognition Battery. The mean age of the influenced patients (25.2 years, SD=3.5) was significantly lower than the mean age of the noninfluenced patients (37.1 years, SD=11.0) (t=–2.6, df=27, p<0.02). Performance on the item match task of the Birmingham Object Recognition Battery was significantly lower in influenced patients (mean score=29.7, SD=3.9) than in noninfluenced patients (mean score=31.9, SD=0.3) (t=–2.7, df=27, p<0.02) but was within the normal range.
During the study procedure, five noninfluenced patients were unable to perform the task correctly, and their data were not included in the comparative analysis. The behavior of these five patients during the task will be described in the first section of Results. They did not differ from the other noninfluenced patients in age, illness duration, educational level, intellectual performance, perceptual abilities (Birmingham Object Recognition Battery scores), or total SAPS score. By contrast, their total SANS score was significantly higher (mean=58.2, SD=16.5) than that of the other noninfluenced patients (mean=36.0, SD=18.8) (t=2.38, df=21, p<0.03).
Materials
During the study procedure, the image of an electronically constructed hand was presented to the subjects on a computer screen with a high refresh rate. A specially designed program synthesized pictures of a hand holding a joystick according to the position of a joystick that was actually held by the subject and was connected to the computer. This design allowed the dynamic representation of the movements of the joystick held by the subject with an intrinsic delay <30 msec. Temporal or angular biases could be introduced in this representation (see the section on procedure), modifying the apparent direction or the degree of synchrony of the movement actually performed by the subject with respect to the movement displayed on the computer screen.
The computer screen was placed face down on a metallic support. A horizontal mirror, located 18 centimeters below the screen, reflected the image. The joystick was placed below the mirror on the table supporting the apparatus. The distance between the table and the mirror was 31 cm, so that the subject’s hand holding the joystick was approximately 18 cm below the mirror. Thus, when subjects looked at the mirror, they saw the image of a virtual hand moving a joystick just above their own hand actually moving a joystick.
Procedure
Subjects sat comfortably in front of the apparatus with their forehead leaning on a foam cushion. They held the joystick with the right hand, with the elbow resting on the table. The position of the forearm was adjusted so as to coincide with the direction of the virtual forearm seen in the mirror. Subjects were instructed to maintain their fingers in a fixed position on the joystick and to restrict their movements to the wrist joint.
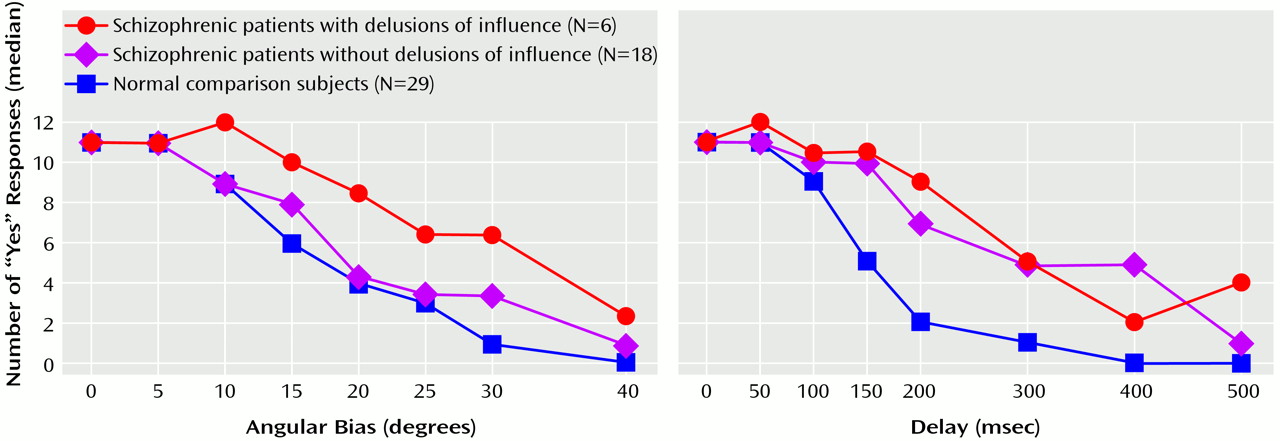
The task consisted of executing a series of simple movements with the joystick. Each trial started with a dark screen. A green spot (1 cm in diameter) was displayed for 1 second on the left, on the right, or on the top of the screen. The image of the virtual hand then appeared for 2 seconds, during which the subject had to execute a movement of the joystick in the direction indicated by the position of the green spot. Immediately after the trial, subjects had to answer the following question with a yes-or-no response: “Did the movement you saw on the screen exactly correspond to that you have made with your hand?”
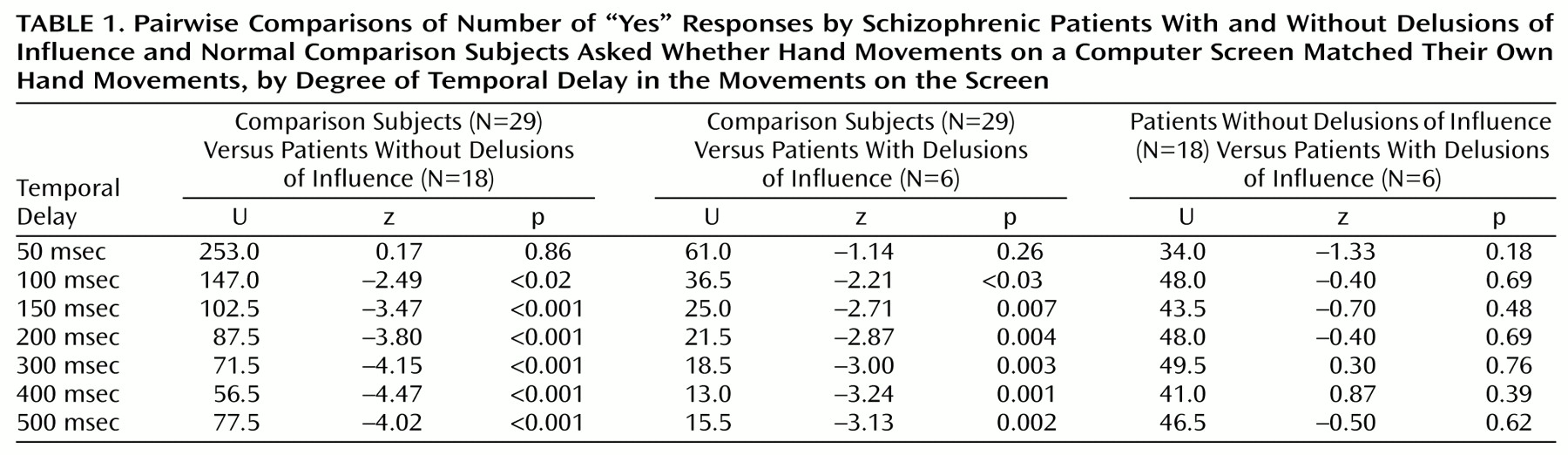
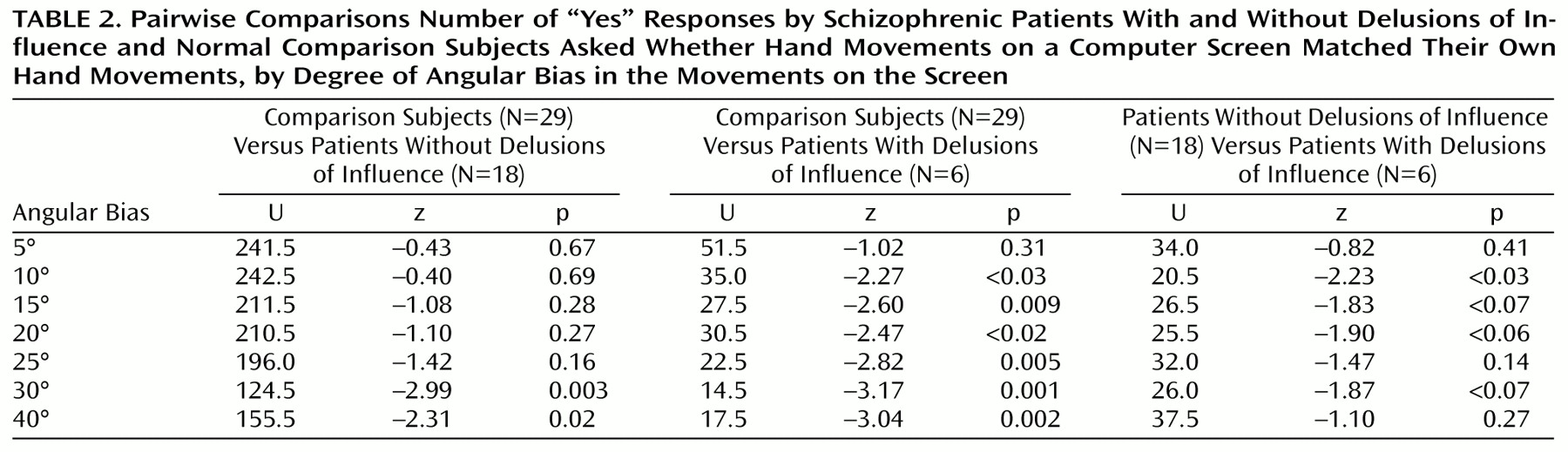
Three categories of trials were used: 1) neutral trials, in which the movements of the virtual hand exactly replicated those made by the joystick, 2) trials with angular biases, in which the movements of the virtual hand deviated by a given angular value (5°, 10°, 15°, 20°, 25°, 30°, and 40° either to the right or to the left) with respect to those made by the joystick, and 3) trials with temporal biases, in which the movements of the virtual hand were delayed by a given time (50, 100, 150, 200, 300, 400, and 500 msec) with respect to those made by the joystick. Each trial with a temporal bias was run four times for each of the three directions of movement (left, right, and top of the screen) (N=84); trials with an angular bias were run two times with a bias to the right and two times with a bias to the left for each of the three directions of movement (N=84). Finally, neutral trials were run 12 times. Each subject therefore executed a total of 180 trials. The order of presentation of the 180 trials was randomized before the participation of each subject. Identical trials could not be presented one after the other.
A 5-minute break was provided after 90 trials. Missed trials were repeated if necessary. Before the undergoing the study procedure, each subject had a training session during which the subject was instructed to freely move the joystick. During the first 30 seconds of the training session, no bias was used; then, a 500-msec bias was introduced; and finally a 30° bias was introduced.