A cognitive neuropsychiatric model of the persecutory delusion specifies the cognitive abnormalities underlying delusion formation and maintenance, and in turn it characterizes these processes in functional neuroanatomical terms
(1–
3). In this paper we review the major cognitive theories currently proposed as explanatory frameworks for the genesis and maintenance of persecutory delusions, together with relevant neural network and functional neuroimaging studies. There is a significant clinical need for a satisfactory explanatory model: persecutory delusions are preoccupying, obtrusive, and distressing
(4) and stand out as directly related to serious violent crime
(5–
8). Patients act on their persecutory delusional beliefs
(9,
10), particularly when the belief has a significant affective impact
(11,
12). A plausible model has the potential to guide future research in both cognitive behavior and pharmacotherapeutic approaches to the treatment of delusions.
Classical definitions of delusions maintained that they were qualitatively different from normal beliefs
(13). They were operationally defined as false beliefs held with unusual conviction, whose absurdity was manifest to others and which were not amenable to logic
(14). However, this monolithic definition has been modified in the light of more recent phenomenological studies. Delusions are not incorrigible: delusional conviction, preoccupation, and distress fluctuate over time
(15,
16) and can be reduced by specific cognitive behavior interventions
(17–
21). Delusions are therefore now conceptualized as dimensional entities rather than categorical ones, lying at the extreme end of a “belief continuum”
(22–
28).
Earlier explanatory frameworks related persecutory delusions to disordered intelligence, thought, affect, or perception. They had obvious limitations and lacked experimental justification
(29). Equally, simplistic models that explained persecutory delusions in terms of neuropsychological dysfunction were discredited by studies in which no specific neuropsychological deficit, e.g., in mnemonic
(30,
31) or executive
(32,
33) function, consistently correlated with measures of persecutory delusions
(34–
36).
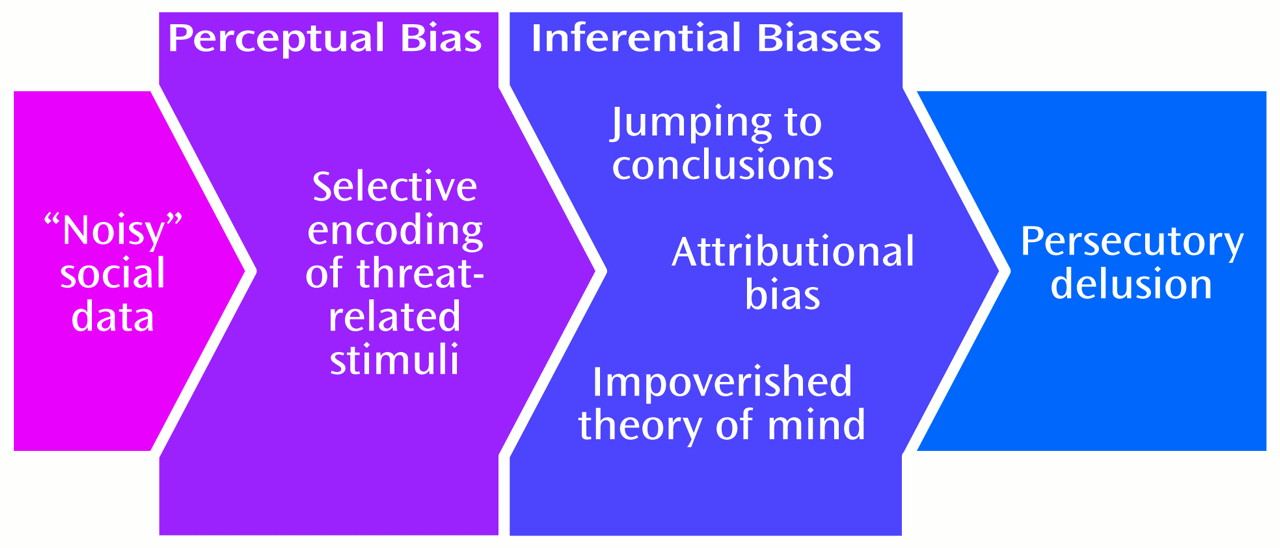
Normal formation of social beliefs depends on 1) selection of social data in the environment relevant to oneself and 2) inferential processing using these data to determine others’ intentions toward oneself in order to guide one’s own behavior. Such social inferential processing is based on access to information stored in the “self-schema,” a repository of autobiographical experience that includes information about the self, relationships with others, and social situations, which determines what is encoded and how it is interpreted
(38). Biases or deficits in these processes (attentional bias, attributional bias, a jumping-to-conclusions reasoning bias, and theory of mind deficits) have been proposed to have etiological significance in the formation of persecutory delusions (
Figure 1). These will be considered in turn.
Attentional Bias
The adaptive behavior of humans relies on the rapid monitoring of salient cues in the environment, such as threatening stimuli. People with persecutory delusions preferentially attend to threat-related stimuli
(39–
41) and preferentially recall threatening episodes
(42,
43). The evolutionary advantage of a “threat-to-self” network outweighs the deleterious effects of such hypervigilant or attentionally biased threat detection. Similar biases have been demonstrated when the content of the task is concerned with threat to the subject’s self-image or self-concept
(44). Preferential encoding and recall of delusion-sensitive material continually reinforces the delusional belief. Such biases appear to depend on the delusional state: that is, excessive attention is paid to threatening stimuli when the subject is actively deluded but not after recovery
(41).
Visual attention and early information processing in a deluded subject may be analyzed by measuring his or her visual scan path
(45,
46), i.e., the direction and duration of gaze when the individual views a stimulus. When schizophrenic subjects with persecutory delusions viewed stimuli consisting of photographs of neutral, threatening, or ambiguous social scenes, they quickly identified the threatening elements of the pictures
(46). However, once they identified the threat in ambiguous pictures, they spent less time than schizophrenic subjects with nonpersecutory delusions and normal subjects in reappraising potentially threatening elements of the pictures. An overly simplistic model that equates persecutory delusions with greater attention to all potentially threatening information was therefore not supported. The discrepancy between this result and the findings from experiments using single words as threat cues
(39–
41) may be explained by proposing that automatic preattentive processes
are selectively tuned to threatening information in subjects with persecutory delusions; the deficient reappraisal of subtle contextual clues is a result of the jump-to-conclusions data-gathering bias we will discuss later.
Attributional Bias
Attribution theory provides a framework for understanding the causal explanations that individuals give for their own behavior and the behavior of others
(38). It has been estimated that normal people make a causal attribution (a statement that includes or implies the word “because”) every few hundred words
(47). Normal subjects consistently demonstrate a self-serving attributional bias in explaining the causes of events; that is, they tend to take credit for success (internal attribution of positive events: the “self-enhancing” bias) and to deny responsibility for failure (external attribution of negative events: the “self-protective” bias). Such biases may serve to enhance self-esteem.
Studies with clinical groups have typically used questionnaires that ask participants to infer the likely causes of hypothetical positive and negative events. Patients with persecutory delusions (with diagnoses of paranoid schizophrenia or delusional disorder) show an exaggeration of this self-serving attributional bias. In cross-sectional studies, they excessively attribute hypothetical positive events to internal causes (self)
(48,
49) and hypothetical negative events to external causes (circumstances or other people)
(40,
48–
51). Deluded patients with nonpersecutory delusions do not differ from normal subjects in their attributional style
(51), suggesting that the attributional bias in paranoid subjects shapes delusional content rather than form. Paranoid patients are additionally abnormal in that negative self-referent events are attributed to active malevolence on the part of the other person (external personal attribution) rather than to the play of circumstances or chance (external situational attribution)
(52).
Bentall
(37) has suggested that this exaggerated attributional bias functions to preserve self-esteem by limiting conscious awareness of negative aspects of the self stored in semantic memory. In this account, when such negative self-representations are primed by threatening events, external personal (other-blaming) attributions are elicited to prevent the activation of discrepancies between how the subject realistically views himself or herself (“actual-self” representations) and how the subject would like to be (“ideal-self” representations). The activation of these discrepancies would lead to a loss of self-esteem. This attributional bias occurs at the expense of contributing to the paranoid patient’s negative perceptions of the intentions of others.
This “persecutory delusion as defense” hypothesis therefore predicts that persecutory delusions will be associated with 1) normal levels of overt self-esteem (the defense’s role is to maintain self-esteem) but 2) low levels of covert self-esteem (revealed by tests capable of penetrating the defense and activating the discrepancies between the “actual self” and the “ideal self”). Cross-sectional studies examining measures of overt self-esteem largely support the hypothesis that persecutory delusions are associated with normal or high levels of self-esteem (49, 50, 53, 54) and very small discrepancies between the actual and ideal selves
(53). However, a longitudinal study examining a cohort of subjects with medication-resistant delusions in a trial of cognitive behavior therapy
(55) suggested that the majority of those with persecutory delusions had low levels of overt self-esteem, which correlated with measures of mood and social functioning. Low self-esteem in this group therefore appeared to be best understood in terms of processes identified in depression, e.g., hopelessness or illness severity. It was interesting that the deluded subjects with the predicted normal levels of overt self-esteem had greater conviction in their delusional beliefs.
Assessing covert self-esteem is more difficult
(56), and different methods for investigating discrepancies between the actual self and the ideal self have yielded conflicting results
(40,
44,
57–
59). For example, low self-esteem is normally associated with perfectionist standards for self-evaluation, which have been found in paranoid patients
(40) even when not depressed
(57). Normal individuals more rapidly generate internal attributions for positive than for negative events, presumably because positive self-representations are more cognitively “available” to them than negative self-representations. This bias is absent in paranoid patients, suggesting that they harbor a relative excess of negative self-representations associated with low levels of covert self-esteem
(58). However, a study using the pragmatic inference task (an attributional questionnaire disguised as a memory questionnaire, therefore generating measures of covert attributions)
(59) did not yield evidence of low covert self-esteem in paranoid patients. To our knowledge, only one study has convincingly demonstrated a discrepancy between overt and covert self-esteem
(50). This research area is complicated by the fact that self-representations are likely to be multifaceted and therefore cannot readily be reduced to a single self-esteem construct
(60,
61).
Methodological limitations of this body of research include its cross-sectional nature, a failure to measure the dimensional severity of delusional beliefs, and a failure to examine symptom specificity, e.g., by examining the attributional style of schizophrenic patients with passivity features but without persecutory delusions. There does nevertheless appear to be convincing evidence at this stage of the externalizing personal attributional bias for negative events in subjects with persecutory delusions, but the “persecutory delusion as defense” hypothesis is less well supported. A parsimonious explanation would hold that this applies to a specific subgroup with persecutory delusions and maintained self-esteem and without a confounding comorbid depression
(56). Longitudinal studies of the relationship between the attributional bias and delusional ideation are required to determine whether the bias is causal or merely an epiphenomenon. However, there is at least preliminary evidence of a residual attributional bias in patients recovered from first-episode psychosis that correlates with residual suspiciousness
(62).
Jumping-to-Conclusions Reasoning Bias
Both the irrationality of normal individuals
(63) and the subtlety of the logical reasoning deficits observed in deluded subjects
(64,
65) are striking. Furthermore, reasoning is heterogeneous to the extent that notions of “normative” performance are elusive
(66). However, paranoid patients have demonstrated a consistent reasoning bias in one particular area: that of jumping to conclusions in tests of probabilistic reasoning.
Hemsley and Garety
(67) have used Bayes’s decision-making theorem as a theoretical basis for examining reasoning biases in deluded subjects. Bayesian models specify whether a subject’s confidence in a current belief should increase or decrease according to the value of new evidence received
(68). The hypothesis that patients with delusions are more prone than normal individuals to draw firm conclusions based on equivocal evidence was examined in a series of studies using affectively neutral material
(59,
69–
71). Deluded schizophrenic subjects and patients with delusional disorder, with either persecutory or grandiose delusions, were asked to make a probabilistic reasoning judgment, namely, which jar (A or B) various sequences of black and white beads had been drawn from, when jar A contained predominantly black beads and jar B contained predominantly white beads. The deluded patients reached a conclusion on the basis of significantly fewer beads than the comparison subjects (demonstrating a jumping-to-conclusions bias) and were relatively overconfident in their decisions. However, when asked to view the same number of beads as other participants before coming to a decision, the group with delusions generated accurate hypotheses with a degree of conviction similar to those for depressed and normal subjects
(72). In other studies
(73,
74) with experimental designs using visual discrimination problems or sensible hypothesis generation and testing, deluded subjects appeared able to formulate and test hypotheses appropriately when supplied with a range of options. Taken together, these results suggest that people with delusions have a data-gathering bias (seeking less information before making a decision) rather than a probabilistic reasoning bias (deluded subjects can aggregate information appropriately, generate hypotheses, and test them).
Such a data-gathering bias was also observed during an inductive reasoning task
(75) and more naturalistic versions of the probabilistic reasoning task in which participants were involved in reasoning about personality characteristics
(76,
77). The bias is more pronounced with emotionally salient material
(76,
77) and is also observed in individuals with high levels of delusional ideation (but falling short in delusional intensity) recruited from the normal population
(78).
The origins of the data-gathering bias remain uncertain. It is a consequence neither of impulsiveness in decision making nor of a tendency to use only recently acquired information
(70,
79,
80), because deluded subjects are more cautious when the evidence is equivocal
(72,
76). It is not a consequence of a memory deficit, since the results are unchanged in the presence of a memory aid
(72). The contribution of IQ to the data-gathering bias has not been systematically studied, but most studies have controlled for any such effects by matching participants on brief measures of intelligence.
Once they have come to a hasty conclusion, how willing are people with persecutory delusions to alter their explanatory hypotheses in the face of contradictory evidence? Deluded subjects
were found to be willing to alter their hypotheses in the face of conflicting evidence from further presentations
(59,
70,
71,
76). This willingness to incorporate new information was more pronounced with emotionally salient material
(76). This finding accords with evidence from trials of cognitive behavior therapy for medication-resistant delusions
(18,
81), which suggests that subjects who are able to consider the possibility, however remote, that they could be mistaken about their beliefs are likely to benefit from treatment in terms of reduced preoccupation with, or conviction in, their delusional beliefs.
The methodological limitations of this body of research are similar to the shortcomings in the research on attributional bias: its failure to measure the dimensional severity of delusional beliefs, its failure to examine symptom specificity, and its cross-sectional nature. The psychometric properties of many of the tests have not been investigated. There does nevertheless appear to be convincing evidence that hasty decision making combined with a failure to gather and assess adequate feedback may, particularly when emotionally salient material is involved, contribute to the formation of erroneous inferences and therefore to formation of persecutory delusions. We have at least preliminary evidence that there are data-gathering biases in predelusional states
(78), suggesting that they may be implicated in delusion formation rather than simply maintenance of existing false beliefs.
Theory of Mind Deficit
The ability to infer the mental states (beliefs, thoughts, and intentions) of others in order to predict and explain their behavior has been conceptualized as the possession of a “mentalizing” ability or “theory of mind”
(82,
83). Persecutory delusions reflect false beliefs about the intentions and behavior of others that could arise from theory of mind deficits. Frith
(1) proposed that theory of mind deficits underpin the origin of delusions of persecution, delusions of reference, delusions of misidentification, third-person auditory hallucinations, some aspects of thought disorder (disordered pragmatics), and negative symptoms (asocial behavior, blunted affect). He hypothesized that theory of mind skills in people with persecutory delusions develop normally (in contrast to individuals with autism) but are “lost” during an acute psychotic episode.
Investigations of theory of mind deficits in deluded subjects have used different methods of assessment. In what may be the first study of its kind
(84), a “hinting” task was used in which subjects had to infer the intentions of characters in samples of indirect speech (e.g., the phrase “It’s very cold in here” should have been taken to mean “Please shut the window”). Difficulties in performing the task correctly were observed in patients with negative symptoms, thought disorder, or persecutory delusions but not in those with passivity features or those in symptomatic remission. However, the study was flawed by a failure to match the patient and comparison groups for IQ (an important confounding variable in theory of mind tasks).
A further set of studies used so-called first- and second-order theory of mind stories
(85). In a first-order story, a character has a false belief about the state of the world; in a second-order story, a character has a false belief about the belief of another character. Correct inference of the mental states of characters is required to understand the actions within the stories that are a result of false beliefs or intentional deceptions. Patients with persecutory delusions had impaired performance on questions concerning the mental states of the characters within the stories and, to a lesser degree, on reality questions (assessing their memory of the factual content of the stories). Patients with negative symptoms and those with thought disorder also showed impairment on questions regarding mental state, but this difficulty was significantly associated with more pronounced memory impairments. Patients with passivity features and those in symptomatic remission performed the tasks as well as normal subjects, indicating that any theory of mind deficit is a state rather than a trait variable. Three potential confounding variables were addressed. The findings in the deluded group could not simply be attributed to memory impairment, since a subgroup who answered the reality questions correctly still had difficulties on theory of mind tasks. Nor were the results a simple function of intellectual ability, as IQ-matched subsamples of deluded patients performed the second-order theory of mind tasks more poorly than psychiatric comparison subjects (see also reference
86). The results were equally unlikely to be accounted for by medication effects, since the patients in remission were receiving medication equivalent to that for the deluded group. Corcoran and Frith
(87) therefore concluded that patients with negative symptoms or thought disorder have the most severe theory of mind deficit (first- and second-order theory of mind task difficulties, poor understanding of conversational hints, and poor knowledge of speech pragmatics) in the context of more generalized cognitive impairment. Patients with persecutory delusions have a more context-dependent mentalizing deficit (second-order theory of mind difficulties, impaired understanding of hints).
Further studies, however, have cast doubt on the primacy or specificity of such theory of mind deficits in formation and maintenance of persecutory delusions. In an examination of the understanding of “physical” or “mental state” visual jokes
(88), patients with persecutory delusions showed a selective comprehension deficit regarding mental state stimuli, failing to infer the mental state of a character and thus failing to “get” the joke. However, they had no greater difficulty with this than depressed psychiatric comparison subjects. Patients with negative symptoms or thought disorder again showed the greatest mentalizing deficit and performed more poorly than the deluded group on the simpler “physical” jokes. Patients in symptomatic remission once more showed no greater difficulty with either set of jokes than normal subjects.
Some patients with chronic schizophrenia had theory of mind problems in picture-sequencing and story-telling tasks
(89), in which correct sequencing in the “mental state” stories required subjects to infer false beliefs in story characters. However, there was no evidence to link this difficulty with the reality distortion symptom cluster (delusions/hallucinations). The patient group with persecutory delusions had general sequencing difficulties, and when the effects of these sequencing difficulties were partialed out, the subjects appeared to have relatively intact mentalizing. Patients with psychomotor poverty (flattened affect, social withdrawal, alogia) had deficits in both general sequencing and mentalizing.
Simplified theory of mind stories (based on reference
90) were subsequently developed to reduce the information processing load for acutely unwell psychotic patients. An acutely unwell schizophrenic group (the majority of whom had persecutory delusions) performed significantly less well than IQ-matched depressed or schizoaffective disorder patients on second-order false-belief tasks and on a metaphor task designed to assess first-order skills
(91). These differences disappeared when the clinical groups were reassessed after symptomatic remission, and this change again indicates a state rather than trait deficit. However, when the data were reanalyzed to compare subjects with schizophrenic or schizoaffective disorder who had persecutory delusions to subjects without persecutory delusions, there were no significant differences in task performance. The results suggest that the problems with theory of mind were not related to persecutory delusions per se but instead were related to the global severity and extent of symptoms (see also reference
92).
Studies using nonverbal stimuli, i.e., comic strips
(93–
95), driven by the hypothesis that the mentalizing deficit is specific to the disorganization symptom cluster, demonstrated that schizophrenic subjects with high levels of thought disorder had specific difficulties in attributing intentions to others, but a “paranoid” subgroup and a subgroup with low levels of thought disorder did not. However, the few subjects with persecutory delusions were inadequately characterized, in that the data were not analyzed in terms of “high” or “low” levels of persecutory delusional ideation.
Finally, using a false-belief picture-sequencing task, Langdon and Coltheart
(96) demonstrated selective theory of mind deficits in nonclinical subjects with high schizotypal ratings, a finding that is consistent with continuity models of psychosis proneness. The “poor mentalizer” subgroup had psychotic-like traits (ideas of reference, suspiciousness, magical thinking, unusual perceptions) as well as asocial or idiosyncratic behaviors (social anxiety, no friends, constricted affect), suggesting that defective mentalizing is linked to both reality distortion and psychomotor poverty.
The studies in the complex literature on theory of mind used differing experimental designs with uncertain psychometric properties in differing subject groups, and thus simple conclusions cannot be drawn. Groups of patients with schizophrenia certainly perform theory of mind tasks more poorly than psychiatric and nonpsychiatric comparison subjects. Any theory of mind deficit is a state rather than a trait variable. The deficit is more pronounced with second-order tasks, which tend to tax all participants to a greater degree. Performance on theory of mind tasks is clearly related to current IQ and memory, but there remains a degree of specificity of poor performance to selected schizophrenic subgroups that cannot be explained by the effect of IQ or deficits in memory alone. Patients with negative symptoms and thought disorder are consistently shown to have a theory of mind deficit, but this is in the context of more general cognitive impairment in this group. Only two studies have provided unequivocal support for a theory of mind deficit in subjects with persecutory delusions
(84,
85). Ultimately, while theory of mind deficits are present in some patients with persecutory delusions, they are not specific and appear more closely related to the symptom clusters of disorganization and psychomotor poverty than to reality distortion.
Neurocomputational Models
The cerebral cortex can be viewed as a computational surface that creates and maintains dynamic maps of important sensorimotor and higher-level aspects of the organism and its environment, reflecting the organism’s experience
(147). One such abstract feature map central to the formation of the persecutory delusion would be the self-schema (an ordered map containing information about the self, relationships with others, and social situations). Its functions could potentially be modeled by a particular type of neural network, the self-organizing feature map
(148). Representations in these cortical and neuronal network maps can change dynamically according to the importance and frequency of the input (experience), a feature known as neuroplasticity. General operational characteristics of these maps can be fine-tuned according to the specific processing needs of the moment, a feature known as neuromodulation.
In Spitzer’s scheme
(149), acute persecutory delusions may be caused by dysfunctional neuromodulation. He noted that dysregulation of dopamine transmission occurs in schizophrenia during periods of illness exacerbation
(150) and that this functional dopamine excess may increase the signal-to-noise ratio in the processing of “noisy” social data, leading to the attachment of self-salience to potentially threatening environmental cues together with a reduction in activation of alternative hypotheses concerning interpretations of these environmental cues. Chronicity of these delusional ideas is accounted for by a disturbance in neuroplasticity: the abstract feature map (self-schema) incorporates the new information in line with the high degree of importance accorded to it and becomes distorted in a way that will reinforce future persecutory interpretations of “noisy” data.
While Hoffman’s pioneering computational models of schizophrenic symptoms
(151–
153) did not specifically focus on persecutory delusions, they nevertheless posited that other positive symptoms could arise as a result of disruptions in parallel distributed processing within the neuronal network caused by breakdowns in corticocortical interactions (in this case by modeled neurodegenerative changes in the form of excessive synaptic pruning). A consequence of this excessive pruning is the emergence of functionally autonomous subpopulations of neurons, the so-called “parasitic foci.” Thus, paranoid delusions of the idée fixe type could arise as a result of a parasitic focus involving narrative memory: a cortical network subserving this narrative memory could become functionally autonomous such that the same output (delusional idea) is slavishly reproduced, the reciprocal connections allowing modification by outside experience having been fatally compromised. By extending these ideas, it is possible to envisage such structural alterations contributing to the altered neuroplasticity subserving chronic persecutory delusions as envisaged by Spitzer.