Cognitive Function and Cerebral Perfusion During Cocaine Abstinence
Case Reports
Case 1
Ms. A, a 34-year-old woman, entered treatment 4 days after her last use of cocaine. She had a 19-year history of cocaine abuse: 10 years of intranasal use and 9 years of crack cocaine use. During the 3 months before her admission, she reported using varying amounts (0.5–1.5 g) of cocaine about 3 days per week. Her recent use of alcohol had been limited to about 1 pint of liquor on each day of cocaine use. She reported two previous substance abuse treatments: the first led to no sustained abstinence, and the second she did not complete.
Cognitive behavior therapy
Ms. A placed herself in the early-late stage of recovery on the basis of the Jellinek chart, a self-assessment instrument for staging the progress of addiction (8). From the outset, Ms. A was forthcoming with self-disclosure and receptive of feedback in group therapy, making excellent use of the group in learning how to handle stress. She had no difficulty identifying the consequences of her use, the most obvious external example being her inability to parent her two children.During her second week in treatment, she reported a sporadic craving for cocaine and recognized that these cravings were playing a significant role in her perception of recovery and treatment. This was evidence of a fairly sophisticated ability to draw inferences. However, although she acknowledged the fallacy of her previous perceptions of drug use—“It will make things better”—she was less aware of the degree of denial that occurred in response to her craving for cocaine, manifested in statements such as, “I can control it.”During her third week in treatment, she remained active in group therapy and was often viewed by peers as a leader within the group. This contrasted significantly with her perception of herself as one consumed with insecurity; the feedback she received highlighted one of the greatest barriers to maintaining abstinence: her low self-esteem. She was able to discuss how her chronic feelings of shame and guilt were exacerbated by, but not entirely caused by, her addiction. After reflecting on her relationships, she agreed to a family therapy session and then chose to end the self-described “enabling” relationship she had with her boyfriend.As noted, her cognitive state was impressive at admission and remained so throughout her treatment. She demonstrated the ability to draw inferences, to challenge unproductive thoughts, to recognize cravings and strategize responses to them, and to retain information. There was clearly a commitment on Ms. A’s part to assume responsibility for her recovery by changing thoughts, behaviors, and relationship dynamics. Although some of this profile may reflect familiarity with treatment, she clearly benefited from a high level of motivation combined with the capacity to integrate new concepts and information and readiness to change. At discharge, Ms. A had been clean and sober for 36 days. She was referred for ongoing treatment and entered a halfway house at discharge.
Neuropsychological testing
This right-handed woman had 13 years of formal education. She performed in the average range on most tests but did show mild impairment in tests that measured simple auditory attention, complex auditory processing, and simple motor repetition. On retesting, her performance fell in the average range on all measures. On her last examination day, Ms. A performed in the average range on most measures but scored above average on one motor test and a complex auditory processing task (the Paced Auditory Serial Addition Task) and below average on a verbal learning and memory task (the Auditory Verbal Learning Test). On this last task, mild impairment was noted both in learning and recall after both long and short delays, indicating lack of concentration or effort or both.Overall, Ms. A demonstrated mild gains in performance over a 28-day study period; these were most likely due to the effects of practice. The results of the last day of testing show that although she showed significant improvement on some tasks, her effort was inconsistent during that session.
Perfusion imaging
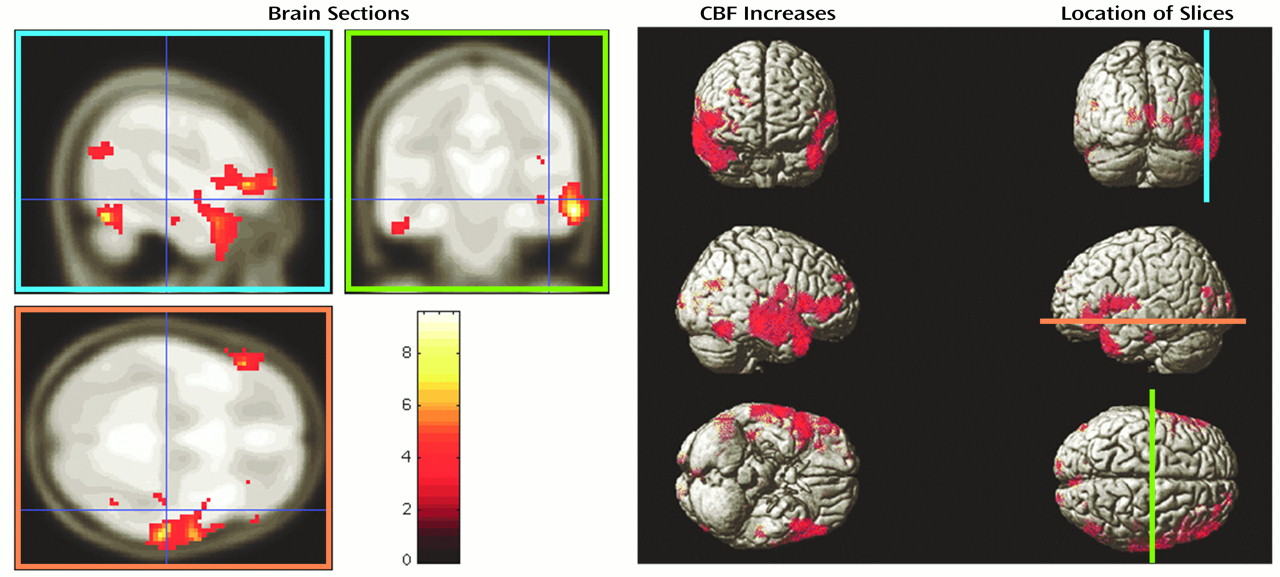
Statistically significant increases in CBF as determined by the use of statistical parametric mapping from baseline to 2 weeks for Ms. A are shown in Figure 2 (9, 10). The total number of regions that improved was not greater than that obtained by chance (i.e., the set-level inference was not significant); however, some individual brain regions showed significantly increased perfusion in both degree and spatial extent. The largest such cluster included the majority of the right temporal lobe. The other significant areas of improvement included the corresponding contralateral region, the left temporal pole, and the frontal opercular cortex bilaterally.
It is interesting to note that Ms. A’s performance on cognitive testing would predict changes in cerebral function in areas related to auditory and language processing. The psychometric test results showed some impairment in measured simple auditory attention and complex auditory processing at baseline, which had normalized by the time of the second test session administration and which was also the time of the second scan, analysis of which is presented here. This convergence of outcome data provides support for the correlation of biological and psychological processes.
Case 2
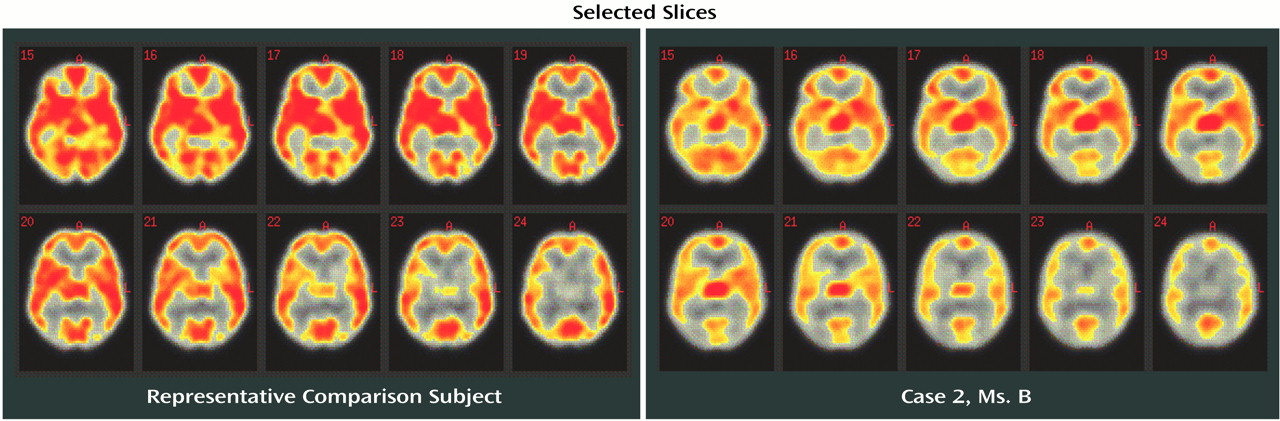
Ms. B, a 32-year-old woman, entered treatment 6 days after her last use of cocaine. She had a 12-year history of cocaine use: 6 years of intranasal cocaine use and 6 years of crack cocaine use. During the 3 months before her admission, she reported using 4–6 g of cocaine per week. Despite a past history of alcohol abuse at ages 18–20, her use of alcohol in subsequent years was described as infrequent. Although she reported an extensive treatment history, her longest period of abstinence was estimated at “a few months.”
Cognitive behavior therapy
Ms. B also placed herself in the early-late stage on a Jellinek chart of stages of addiction. For Ms. B, participation during group therapy was limited, despite peer and staff encouragement to involve herself. Initially, she recognized only the obvious consequences of her abuse: legal trouble resulting from a possession charge and the subsequent involvement of the Department of Children and Families. Her denial of the scope and severity of her addiction was at least partly related to an apparent inability to draw inferences, a relatively sophisticated cognitive process. Her first treatment plan was designed to address this deficiency.During her second week in treatment, her participation during group therapy improved significantly. She identified with more clarity the progression of her drug use and the parallel progression of its consequences. She described what she would gain—control of her life, resumption of parental duties, employment, better health, all of which would improve her overall self-esteem and lose—nothing—if she eliminated drugs from her life. In response to this new recognition of cause and effect relationships, the next period of treatment focused on her underlying perceptions about drug use and the relation of those perceptions to her continued motivation to use. At this point she developed her second treatment plan, focusing on relapse-prevention planning.During her third week in treatment she remained active in group therapy, although she frequently needed prompting to reveal more about herself and her progress in recovery. She identified her tendency to keep problematic issues to herself so as not to risk relapse. Her hesitancy to share information was not due to an inability to understand the nature of therapy for substance dependence. Indeed, she was able to identify relapse warning signs and effective coping strategies for them, but her motivation to address them proactively was inconsistent and, at times, nonexistent. She reported considerable past difficulty in sustaining motivation for recovery, due to, as she saw it, a nonsupportive family. However, she had never utilized self-help techniques or another support system to her advantage. In the hope of reinforcing motivation, therapy again focused on reasons to remain clean. Although she appeared genuinely “tired” of her life as it has been, her passive and at times apathetic attitude toward abstinence were significant barriers to her recovery. She declined an opportunity for family therapy, stating she had “heard it all before.”In order to overcome her passivity, further treatment addressed her patterns of thinking. This revealed that most of her thoughts reflected low self-esteem and low self-expectations. She was able to acknowledge that as long as she remained an active substance abuser, she would be unable to regain control of her life and realize her goals, such as custody of her child. She was encouraged to challenge her automatic, self-defeating thoughts and to communicate honestly with peers in treatment and self-help. Utilizing peer relationships in this way may have been complicated by the fact that she was the only woman in her treatment group. However, she was encouraged to make use of her clinician and other clinicians in the program who were female when this appeared to present an obstacle to her.At discharge, Ms. B had been clean and sober for 30 days. As noted, her cognitive state had improved significantly, as evidenced by her ability to draw inferences, challenge unproductive thoughts, identify and strategize for high-risk situations and relapse warning signs and by her ability to retain information. Despite all that she gained cognitively, her ability to assume responsibility for her recovery by proactively changing thoughts, behaviors, and relationship dynamics was questionable. She was referred to another partial day program at discharge.
Neuropsychological testing
This 32-year-old, right-handed woman had 12 years of formal education. In the first test session, she performed in the average range on measures of simple auditory attention and concentration, visuomotor integration, verbal fluency, and learning. On tests that demanded a strong motor effort, her performance was slow (moderate or moderately severe impairment). In addition, her performance in retrieving verbal information after a long delay and on a complex working memory task were significantly below average (mild to moderate impairment). On her second testing session, she maintained her performance on most tests, yet demonstrated improvement on most motor coordination measures and on one task that requires visual scanning (digit vigilance). Her scores on indices of learning and memory were generally lower on repeat testing at 2 weeks than in her first testing session, consistent with the results of other research in cocaine-dependent individuals, suggesting persistence of declarative memory problems over other cognitive deficits (1). At her last examination, Ms. B performed in the average range on most measures. Exceptions to this were similar to the ones found in session 2: relative impairments were noted on both delayed memory and on complex mental control tasks. Further gains from the second session were noted on a simple motor repetition (finger oscillation) task.Overall, Ms. B demonstrated mild to moderate gains in performance over the 28-day period, but especially on movement-related tasks. Some of the improvements demonstrated by Ms. B were undoubtedly due to the effects of practice. However, she did not exhibit consistent gains across trials (as one would expect with similar effort); therefore motivation must be considered a mitigating factor. This possibility was more apparent for tasks that demand greater effort.
Perfusion imaging
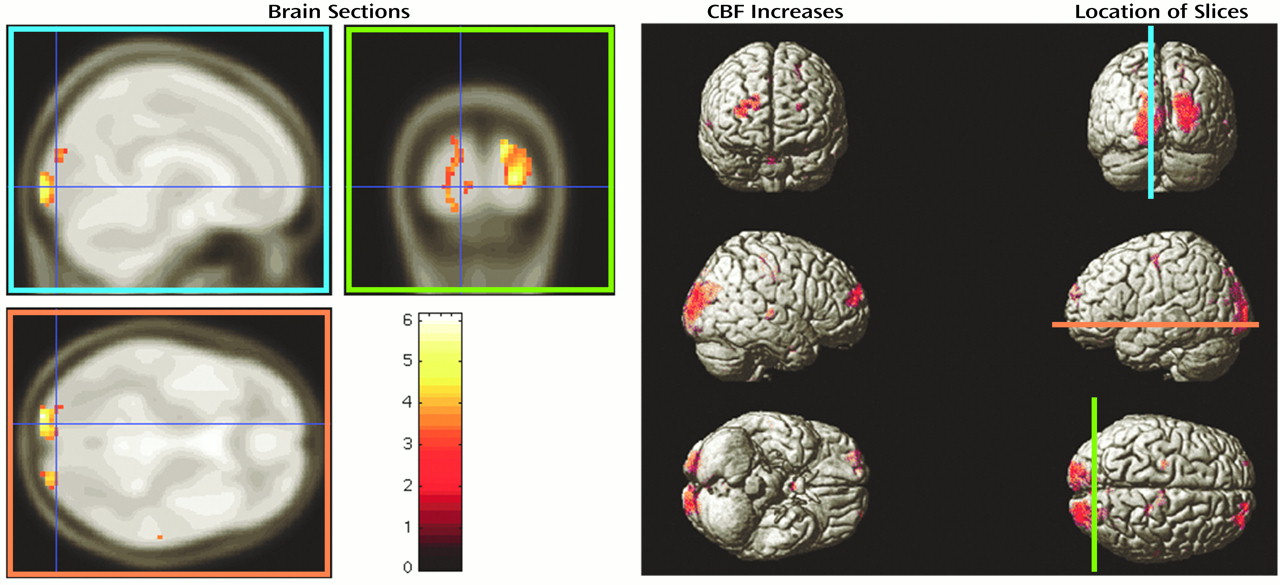
Increases in CBF from baseline to 2 weeks for Ms. B are shown in Figure 3. The number of regions of change, the set-level inference, is significant at the 5% error level. Several individual regions are also significant in degree of change in perfusion and in spatial extent: left and right occipital poles (including some visual association cortex), and a region of the right dorsolateral prefrontal cortex.
When we compare the results of previous cognitive and motor tests with areas of change in perfusion, we note a correspondence of these regions with the improvement noted in visual scanning tasks and hand-eye coordination. Although the perfusion imaging shows an increase in perfusion in the dorsolateral prefrontal cortex, the performance on memory tasks was worse on repeat testing; this divergence may reflect a greater demand on a brain region involved in performing working memory tasks. In addition to these specific regional findings, it is the overall (set-level) significance that we emphasize here. This is an index of the proportion of all cortical tissue with greater perfusion over this test period and provides evidence in this second case that the effect of abstinence on cerebral perfusion was distributed across the entire brain.
Discussion
Conclusions
Footnote
References
Information & Authors
Information
Published In


History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).