Breast milk offers many advantages to developing infants. The American Academy of Pediatrics endorses breast milk as the best and only source of nutrition necessary for the infant during the first 6 months of life
(1). Breast-fed infants have lower rates of gastrointestinal disease, anemia, respiratory ailments, and otitis media
(2,
3). In addition, breast-feeding provides a unique opportunity for bonding between infant and mother
(4).
The vulnerability for psychiatric illness during the 3 months after delivery raises the possibility that psychotropic medications will be administered
(5,
6). Issues to address during analysis of the risks and benefits of psychotropic use during breast-feeding include documented benefits of breast-feeding, the potential adverse impact of untreated maternal mental illness on infant attachment and cognitive and behavioral development, and the effects of untreated mental illness on the mother
(7–
13). This article reviews the literature on the various classes of psychotropic medications in order to provide the basis for educated treatment planning.
On average, nursing mothers produce 600 to 1,000 ml of milk daily. Factors affecting medication concentration in breast milk are pH, protein content, and lipid content. These vary throughout the postpartum period and at different times during a single feeding, resulting in marked concentration variations in milk aliquots. Milk pH ranges from 6.35 to 7.65
(14). Mature milk is produced approximately 2 weeks after birth. The higher lipid content of hind milk (the milk ejected during the second half of a feeding) makes it likely that the second half will have a higher concentration of maternal medication than the first half (fore milk). Other major factors affecting medication concentration in breast milk include lactose, serum albumin, lysozyme, approximately 30 enzymes, prolactin, and minerals such as calcium and phosphates
(15).
The extent to which an infant is exposed to medication is affected by the rate of absorption into maternal circulation, diffusion from maternal circulation to breast milk, and absorption of the agent by the infant. Taking medication immediately after breast-feeding minimizes the amount present in milk and maximizes clearance before the next feeding
(16). In vitro studies have demonstrated that full-term neonatal cytochrome P-450 activity is approximately one-half that found in adults
(17). Each liver enzyme system matures at a different rate in the developing infant. Thus, different substrates are metabolized at different points in maturation. For example, while glucuronyl transferase activity is mature enough to metabolize bilirubin 3 days after term, it cannot safely degrade chloramphenicol until at least day 10. Hepatic enzyme immaturity is even more pronounced in premature infants. Premature and full-term infants have a diminished capacity to metabolize medications for at least the first 2 weeks of life
(17).
While the ratio of kidney weight to body mass in infants is twice that in adults, the newborn kidney is functionally immature. With a glomerular filtration rate only 30%–40% of adult values and tubular secretion 20%–30% of adult function, renal excretion is considerably diminished. Consequently, compounds eliminated through the kidney tend to accumulate in the infant, causing toxic exposure over time
(18). For full-term infants, the glomerular filtration rate seen in adults is achieved between the second and fifth months of life
(19).
Since the newborn blood-brain barrier is also immature, lipid-soluble agents can be 10–30 times more concentrated in the CSF than in serum
(20) and may be higher in infants for a given plasma concentration compared to adults
(21). Because body fat storage sites are limited in the neonate, central nervous system concentrations of lipid-soluble substances are greater in newborns than in older infants
(22).
Despite the pharmacokinetic complexity and variability of the individual compartmentalized processes just described, most reports do not account for maternal, breast milk, or infant data. Frequently, infant exposure is estimated by measuring breast milk concentrations and assumed average daily milk consumption.
Method
This review comprises an analysis of 95 studies and reports covering 32 psychotropic agents used by nursing mothers. Of the studies, 66 measured infant serum concentrations. In some cases, infant serum concentrations reflected exposure both in utero and through breast milk. The wide range of variability in sensitivity and reliability of a given assay precluded meaningful statistical grouping of individual case reports. Most reports lacked data for concentrations relative to time of dose administration. The interval between medication dose administration and infant feeding times is rarely reported. Finally, where infant clinical status is documented, behavioral evaluation is rarely based on standardized clinical assessment.
To avoid overinterpretation of data with so many limitations, and since the clinical significance of infant serum concentrations of medications is unclear, detailed discussion is reserved only for data that suggest a possible connection between drug and deleterious effects in offspring. Guidelines for the use of psychotropic agents in breast-feeding mothers will be suggested.
Results
Antidepressants
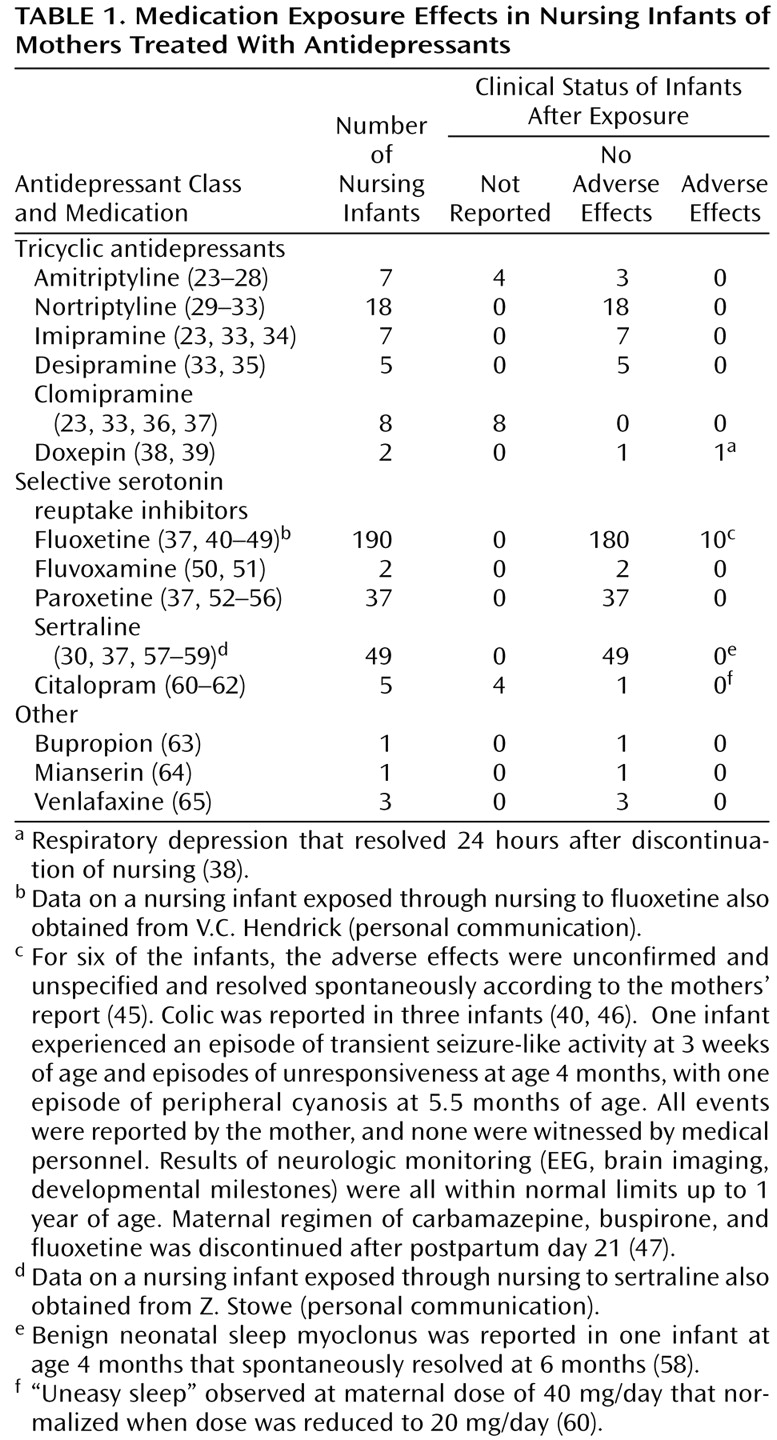
Data from studies of breast-feeding and antidepressants are summarized in
Table 1.
Tricyclic antidepressants
Infant serum levels of parent and active metabolites reported in studies of tricyclic antidepressants ranged from nondetectable to less than 28 ng/ml. Despite widely ranging milk-to-plasma ratios and variable infant serum levels of amitriptyline and nortriptyline (either as parent drug or as a metabolite of amitriptyline), there were no reports of adverse effects in the breast-fed infants. Similarly, no adverse effects were reported for the seven infants exposed to imipramine, the five infants exposed to desipramine, or the eight infants exposed to clomipramine.
For doxepin, two single case reports revealed milk-to-plasma ratios of parent and metabolite compounds that were close to or greater than one and measurable serum metabolite concentrations. Respiratory depression occurred in one case
(38) but resolved 24 hours after discontinuation of nursing. Since the infant was not exposed to doxepin rechallenge through nursing, it is not possible to state definitively that respiratory compromise was due to doxepin. In the second case
(39), no adverse effects were noted in the infant.
Selective serotonin reuptake inhibitors (SSRIs)
Fluoxetine use by breast-feeding mothers has been evaluated in 11 published reports of 190 breast-fed infants (
Table 1). In 101 cases, infant sera concentrations were not tested. Of the remaining cases, levels of parent compound and metabolite varied from nondetectable to a single report of 340 ng/ml
(40). There were no clear associations between levels in infant sera, maternal dose, and infant age. No adverse effects were noted in 180 of the 190 cases. One study of four infants reported normal neurobehavioral development to 1 year of age
(44). Of some concern is a single case of a 6-week-old infant with serum concentrations of fluoxetine that were comparable to maternal concentrations
(40); adverse effects reported included excessive crying, decreased sleep, vomiting, and diarrhea that dissipated upon discontinuation of nursing. Adverse effects reported in other studies were transient and by maternal report
(45,
46) or were confounded by multiple medications
(47). Although a retrospective study indicated poorer weight gain for fluoxetine-exposed infants than age-matched control subjects, weights in the exposed infants were not statistically below the national mean
(48). These data highlight the importance of professional monitoring of the clinical status of nursing infants rather than relying on laboratory measurements of serum levels and maternal observations.
Fifteen published reports documented the use of the remaining SSRIs (fluvoxamine, paroxetine, sertraline, and citalopram) in breast-feeding mothers. For sertraline, infant serum levels were nondetectable or less than 5 ng/ml for parent compound; the metabolite concentrations that were measured in four reports were less than 10 ng/ml. In the six paroxetine reports, serum levels were measured in 27 of the 37 breast-fed infants: concentrations ranged from nondetectable for 24 of the infants to less than 20 ng/ml in the remaining three. Citalopram and desmethylcitalopram were measured in infant serum in two of the citalopram case reports
(60,
61): concentrations ranged from 2.3 ng/ml to 12.7 ng/ml, and metabolite concentrations were nondetectable. Serum levels were not reported for fluvoxamine. No clear adverse effects were noted in the 49 infants exposed to sertraline, the 37 exposed to paroxetine, or the two exposed to fluvoxamine.
Other antidepressants
Although five infants exposed through nursing to bupropion, mianserin, or venlafaxine did not experience apparent adverse effects, more data are needed before conclusions can be made regarding their safety in breast-feeding. Since infant serum concentrations and clinical status were not reported for the novel antidepressant trazodone
(66) or the reversible monoamine oxidase inhibitor moclobemide
(67), the safety of these agents in exposed nurslings is unknown.
Anxiolytics
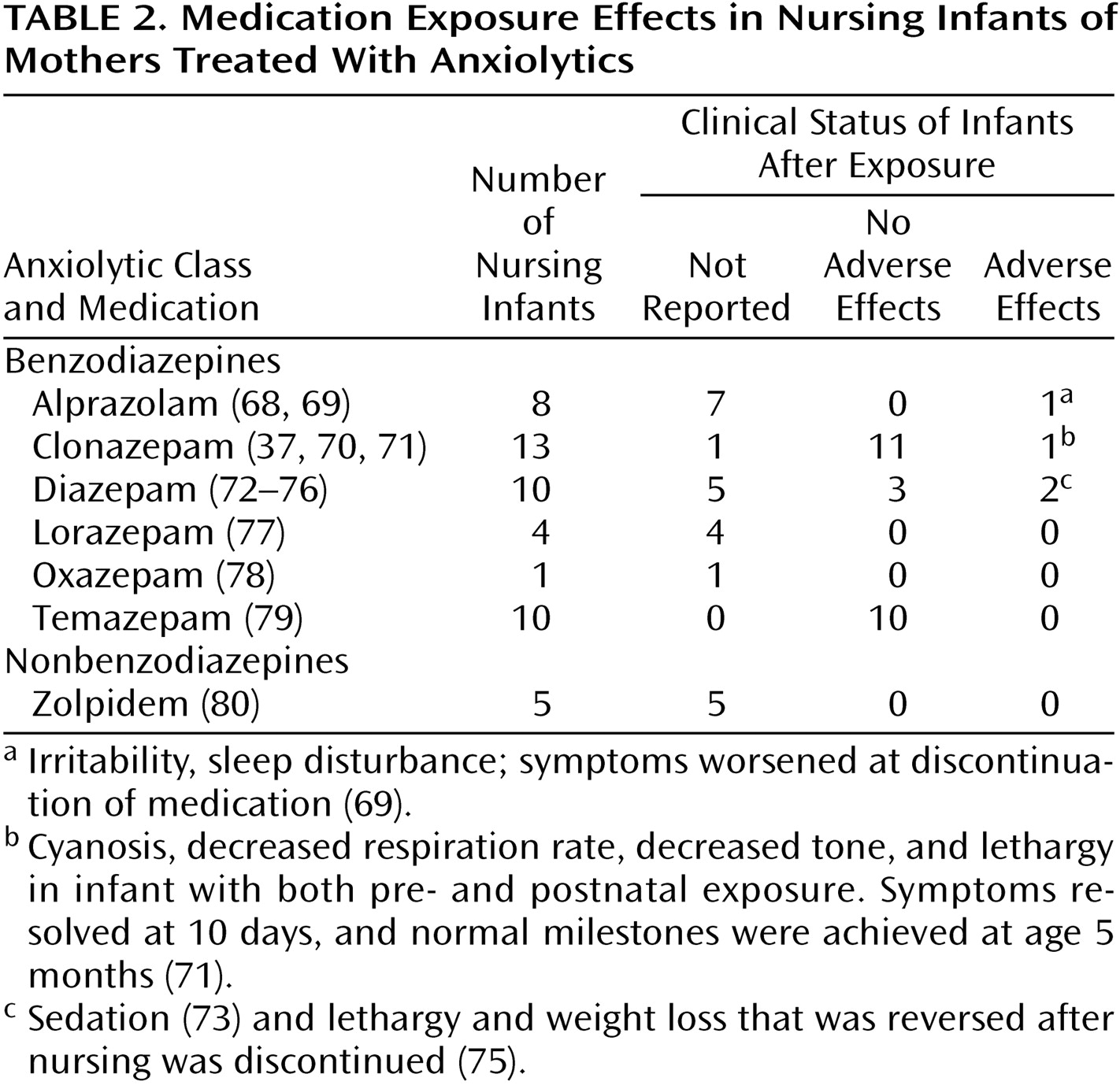
Studies with data on anxiolytic exposure in nursing infants are summarized in
Table 2.
For 12 of 13 infants whose mothers were on regimens of clonazepam, exposure was in utero as well as through breast-feeding. In one case of an infant exposed both in utero and through nursing to clonazepam (infant serum level <5 ng/ml), persistent cyanosis was noted at delivery and for the first 10 postpartum days
(71). By day 10 breathing normalized, and neurodevelopment appeared to be normal at 5 months
(71). For the remaining 11 infants for which clinical status was described, no adverse effects were noted
(37).
Only three of 10 infants exposed to diazepam through nursing had data for serum concentrations of parent and metabolite compounds, which varied from nondetectable to 243 ng/ml. Serum levels of both parent and metabolite compounds were lowest in the oldest nursling, an infant of 1 year of age
(72), which suggests that older infants have improved metabolic capacity. Clinical status was reported in five infants, with no adverse effects in three
(76) and normal development recorded in a fourth despite some apparent sedation
(73). In another case report, lethargy and weight loss was reversed following discontinuation of nursing
(75). For the 11 infants exposed to oxazepam or temazepam (and its metabolite, oxazepam), no adverse effects were noted.
The remaining reports of medication effects in infants exposed to anxiolytics through breast milk involved treatment with alprazolam, lorazepam, or zolpidem. Infant serum concentrations were not reported, and in the one case where clinical status was reported
(69), alprazolam withdrawal appeared upon medication tapering.
Antipsychotics
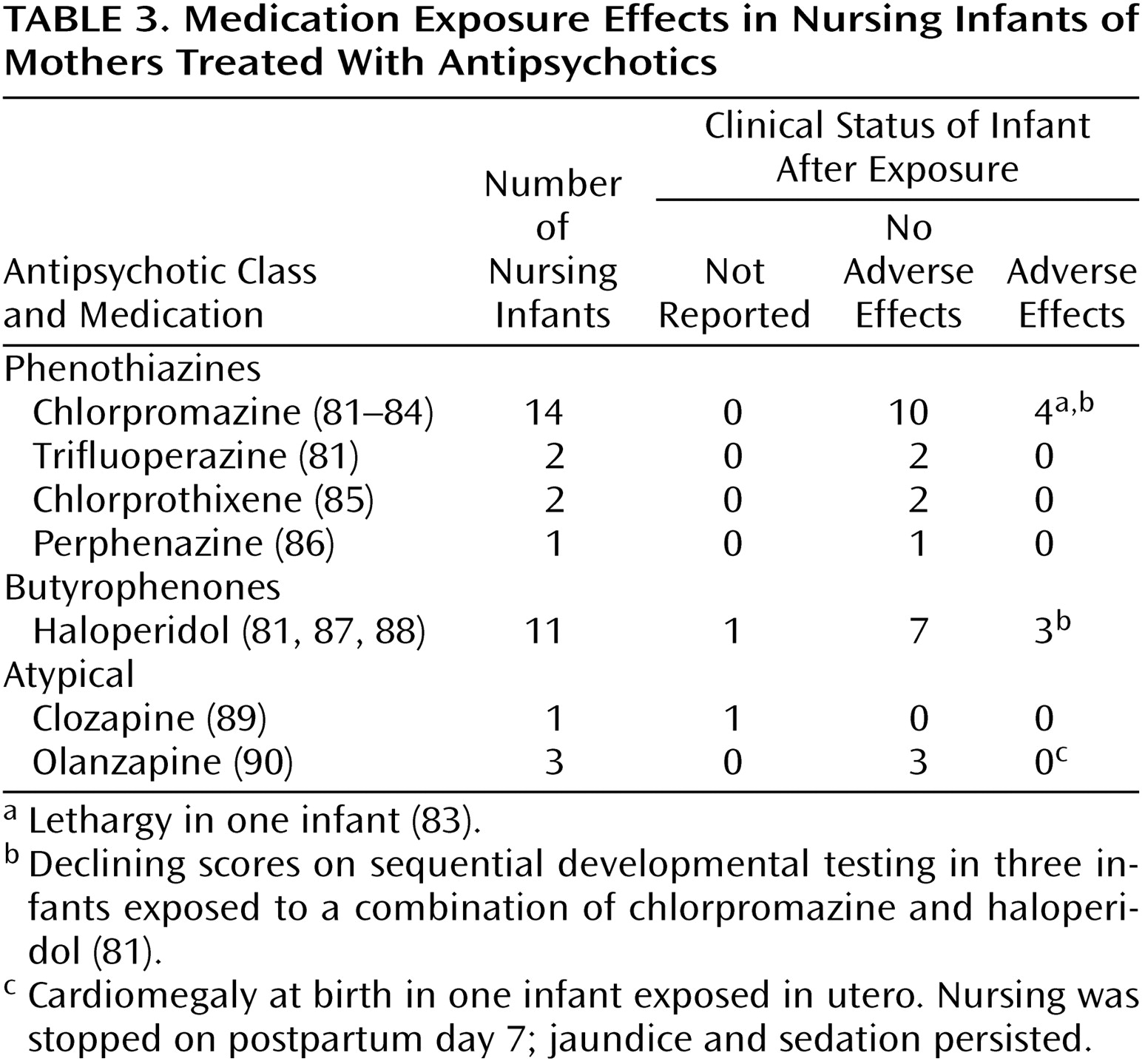
Ten reports have addressed infant exposure to antipsychotic agents through nursing (
Table 3). Of 34 clinical status reports of infants exposed to antipsychotics through breast milk, 25 showed no adverse effects. Lethargy was noted in one chlorpromazine-exposed infant
(83). Delayed developmental testing at 12–18 months of age was reported for three infants exposed to a combination of haloperidol and chlorpromazine; only one of the three infants had detectable serum levels of neuroleptic
(81). In a single case report of clozapine exposure during breast-feeding
(89), milk-to-plasma ratios for clozapine revealed that it was concentrated in milk, but since there were no data regarding infant serum levels, the relevance of this is unclear. The early data for olanzapine come from one report of three infants exposed both in utero and through nursing
(90); no adverse effects attributable to olanzapine ingestion through breast-feeding were noted.
Mood Stabilizers
A recent study indicated that postpartum bipolar women who discontinued lithium before pregnancy were almost three times as likely to have a recurrence in the first postpartum month as bipolar control subjects
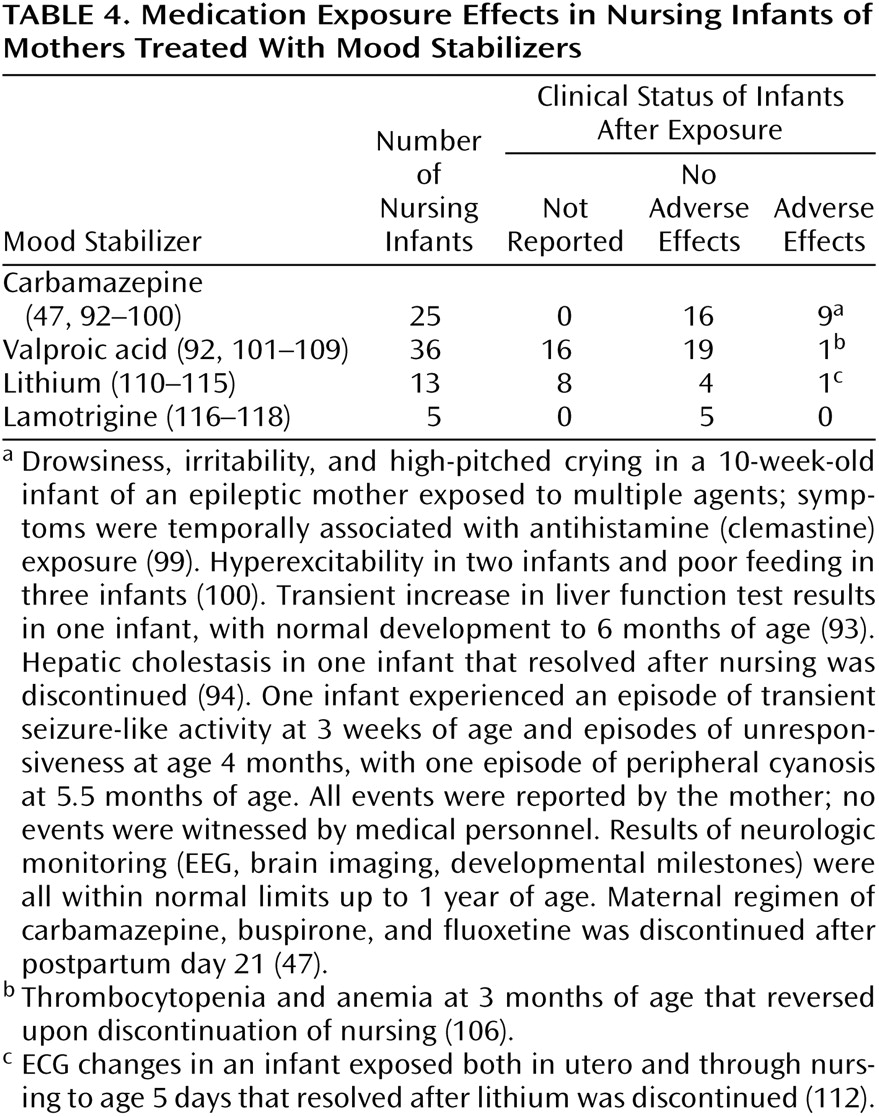
(91). Twenty-eight reports of the use of mood stabilizers in nursing mothers include 79 infants exposed to lithium, carbamazepine, valproate, or lamotrigine through breast-feeding (
Table 4). Of 25 cases of carbamazepine exposure in nursing infants, there were two cases of transient hepatic dysfunction
(93,
94). The etiology of reported instances of seizure-like activity
(47) and drowsiness, irritability, and abnormal crying
(99) was impossible to ascribe because of the exposure to a combination of agents through breast milk.
Of 36 valproate-exposed infants, no adverse effects were noted for 19, and clinical status was not reported for 16. Thrombocytopenia and anemia in an exposed 3-month-old infant reversed upon cessation of nursing
(106).
Of the 13 infants exposed to lithium, serum concentrations were found to be very high. One infant with a congenital heart murmur, cyanosis, and hypotonia had been exposed to lithium both in utero and through breast milk
(112). There were no adverse effects in four other infants, and clinical status was not reported for eight. No adverse effects were reported in five cases of lamotrigine exposure in nursing infants. We found no published data on gabapentin exposure through nursing.
Treatment Guidelines
General Issues
The decision to breast-feed while taking psychotropic medications is complicated. Considerations include known benefits of breast-feeding to infant and mother, wishes of the mother, risk of infant exposure to the medication, and the possibility that a severely depressed, anxious, or psychotic mother may forego treatment rather than give up breast-feeding.
Parents faced with this decision should be educated about possible side effects in their infants. As the association between infant drug levels and clinical status is unclear, clinical monitoring seems to be the best approach to minimize the risk to infants. Before initiating maternal medication, a pediatric evaluation should assess infant baseline behavior, sleep, feeding, and alertness. Metabolism and elimination are more efficient in older infants, who generally sleep for longer intervals, permitting dosing of the mother just after nursing and before the baby’s longest sleep interval. The pediatrician should be educated about potential side effects of medication exposure and interactions with other medications typically prescribed to infants (e.g., antibiotics, nonsteroidal anti-inflammatory agents, acetaminophen). Caution should be exercised when prescribing hepatically metabolized medications (such as acetaminophen) to breast-fed infants whose mothers are treated with psychotropics, since infants with immature liver function may have difficulty eliminating several medications through the same hepatic enzyme system. Mothers taking agents such as paroxetine, fluoxetine, or fluvoxamine should abstain from caffeine, since its metabolism is inhibited by these antidepressants.
The choice of medication depends on diagnosis, past history of the mother, side effect profile, dose flexibility, and pharmacokinetic characteristics that minimize accumulation of the agent in milk and infant serum. Dosage should be as low as possible while still achieving psychiatric remission. Doses so low as to constitute ineffective treatment represent needless exposure by infant to medication.
If a medication is administered on an as-needed basis, short-acting agents are probably preferable. It is best to use medications in which the parent compound does not metabolize into several generations of active compounds. Formula supplementation reduces infant exposure while retaining some breast-feeding benefits.
It is important to note that low or even negligible infant serum medication levels are not necessarily reassuring, since access to the brain and target cell sensitivity may be greater in young infants. Infant clinical status is the most important parameter to follow. Parents should be alerted to the side effect profile of medications, and monthly pediatric clinical monitoring is important to ensure general health and normal pediatric development.
Postpartum Depression
Depression in the postpartum period is disabling. If cognitive behavior therapy or interpersonal therapy is not helpful, or if the condition warrants aggressive early treatment, consideration should be given to ECT. Once diagnosed, postpartum psychiatric disorders are frequently managed with psychotropic medications. As noted by Wisner et al.
(119), the use of antidepressants by nursing mothers is often acceptable so long as the mother-infant pair is carefully monitored. Data on the use of tricyclics by nursing mothers suggest that while parent compound levels in infant serum are often below the limits of detection of most commercial laboratories, metabolite levels in infant serum are sometimes detectable. The single case of respiratory distress in an infant exposed to the sedating antidepressant doxepin
(38) suggests that it is best to avoid this agent in nursing mothers.
The emerging data for SSRIs is important, since this class comprises the most commonly prescribed antidepressants. The data for fluoxetine are variable and somewhat difficult to interpret. The few adverse effects were generally transient and not verified by medical personnel or objective tests. The lack of adverse effects in 180 fluoxetine-exposed infants justifies its continued use if it has been prescribed antenatally or if there is a history of preferential efficacy with this agent. A previous report suggests that there is little central serotonin reuptake inhibition in infants breast-fed by mothers taking sertraline
(120). Although the gradient of antidepressants such as paroxetine tends to increase from fore milk to hind milk
(52), the extent to which this is reflected in infant serum depends on the extent of nursing at any single feeding. Furthermore, the lack of adverse effects in 86 breast-fed infants exposed to sertraline or paroxetine and the uniformly low or nondetectable infant serum levels in these infants suggest that these are good choices for nursing mothers with postpartum depression. In the case of sertraline, serum levels peak in infants between 7 and 11 hours after maternal dosing; refraining from nursing during this time period may significantly reduce infant exposure
(57). Similar peak levels have not been reported for paroxetine or fluoxetine. As the data for fluvoxamine and citalopram are sparse, these agents are not primary treatment options for breast-feeding mothers.
Postpartum Bipolar Disorder
Treatment of bipolar disorder invariably requires mood stabilizers. Maternal use of lithium and carbamazepine has been associated with serious difficulties in nurslings. There has been a single recorded case of serious blood abnormalities following exposure to sodium valproate through breast milk
(106), and this agent has been associated with hepatotoxicity when directly administered to infants
(121,
122). Therefore, when administering valproate to breast-feeding mothers, pediatric clinical status, liver enzymes, and platelets should be carefully monitored.
Lithium increases the risk of thyroid dysfunction, cyanosis, poor muscle tone, and ECG changes in infants
(19,
114,
123). Because renal clearance is decreased in infants up to at least 5 months of age, use of lithium during breast-feeding is not advisable. Nevertheless, for the bipolar patient who invariably decompensates when lithium is discontinued, use by a nursing mother may be reasonable so long as infant clinical status is carefully monitored and serum concentrations of lithium in the infant are followed.
While the American Academy of Pediatrics suggests that carbamazepine exposure appears safe for breast-feeding infants, two cases of hepatic dysfunction
(93,
94) and one case of transient seizure-like activity
(47) suggest that it is advisable to monitor liver enzymes, bilirubin, and WBC counts frequently and to assay for carbamazepine levels in exposed infants. There are limited (although reassuring) data on lamotrigine exposure through breast milk and no data for the use of gabapentin by nursing mothers. Since these agents are not first-line medications for bipolar disorder, their use in breast-feeding should be reserved only when no other alternatives remain for effective treatment.
Postpartum Anxiety Disorders
Postpartum anxiety may be ameliorated with nonpharmacologic interventions (e.g., cognitive behavioral therapy, progressive relaxation techniques, environmental stress reduction). When possible, securing a nanny is helpful to reduce sleep deprivation. Occasional low doses of short-acting benzodiazepines such as temazepam or oxazepam are probably safe
(124). Reports of adverse side effects for diazepam and withdrawal with alprazolam suggest that these should not be a first option if a benzodiazepine is administered to a breast-feeding mother. Tricyclics (with the exception of doxepin) or SSRIs are also good options for the treatment of panic disorder in breast-feeding mothers.
Postpartum Psychosis
Postpartum psychotic symptoms should be treated with antipsychotics. Psychotic women may be so dysfunctional that they are unable to breast-feed their infants. In cases of infant exposure to antipsychotics through breast-feeding, infant clinical status should be regularly monitored for antipsychotic side effects such as somnolence, muscle rigidity, or tremors. The reports of developmental decline in infants nursed by mothers receiving antipsychotic combinations suggest that a monotherapeutic regimen should be maintained
(81). Clozapine-induced fatal agranulocytosis in adults and the lack of data on infant clinical status make it imprudent for mothers treated with this agent to breast-feed their infants. Of note, conception is possible while breast-feeding, and the method of birth control should be documented during the risk-benefit discussion.
Conclusions
Women with postpartum psychiatric disorders often face the dilemma of whether or not to use psychotropic medication while continuing to breast-feed their infants. In such cases, it is important to safeguard the mental health of the mother while at the same time optimizing the emotional and physical well-being of the infant. All psychotropic agents enter breast milk. While these medications pass into infant circulation to varying degrees, a clear relationship between concentration of these medications (and their active metabolites) on infant physiology, behavior, and development is unknown. Therefore, rather than basing decisions regarding the use of medications during breast-feeding on serum levels, it is prudent to carefully monitor the clinical status of infants who are breast-fed by mothers taking psychiatric medications. In the event that the parents or pediatrician become concerned that the infant’s behavior, activity level, or achievement of developmental milestones may be related to medication exposure, serious consideration should be given to weaning. Studies are needed that relate measured levels of medications and metabolites in the sera of breast-fed infants to clinical status and that carefully note infant age and maternal and infant weights at the time of blood sampling. Accurate assessments may then be made of comparative levels of drug exposure on a per-kilogram basis in infant and mother. Clinical status and behavior of these infants should be carefully observed by using standardized pediatric instruments. In this way, more definitive conclusions may be made about the clinical significance of infant serum concentrations and infant daily exposure.