Data from several epidemiologic studies show that a majority of individuals who experience a panic attack will also have an episode of major depression during their lifetime
(1–
3). The likelihood of this co-occurrence is even stronger among those who meet the full criteria for panic disorder
(1). A substantial minority of individuals who experience an episode of major depression also experience panic attacks
(1,
2). The functional disability and risk of suicidal behavior associated with comorbid panic and depression far exceed those associated with either disorder alone
(4).
Most clinical and epidemiologic data suggest that the onset of anxiety usually precedes the onset of depression
(1,
2). In the National Comorbidity Survey, a majority of respondents with lifetime panic-depression comorbidity (43.4%) experienced their first panic attack before the first onset of major depression
(1). Wittchen et al.
(5) found that anxiety preceded onset of depression in a majority of subjects with comorbid anxiety and depression in clinical and epidemiologic samples.
Despite the availability of efficacious treatments
(6), panic is often undiagnosed and untreated
(7). Delay in diagnosis and treatment of several chronic medical conditions is clearly associated with a greater risk of subsequent associated morbidity (e.g., untreated hypertension is associated with greater risk of coronary disease
[8]). Similarly, a longer length of time from onset of panic to first treatment is associated with higher rates of comorbidity at first psychiatric treatment contact and less favorable treatment outcomes among panic disorder patients in psychiatric settings
(9). It is not known, however, whether treatment of panic attack reduces the risk of developing major depression.
The purpose of the current study was to investigate the effects of treatment of panic attack on the subsequent risk of first onset of major depression. We hypothesized that treatment of a panic attack will have a protective effect on the risk of major depression.
Method
The National Comorbidity Survey (N=8,098) is based on a national probability sample of individuals 15 to 54 years old in the noninstitutionalized population. There was an 82.4% response rate. Weights are described in detail elsewhere
(10,
11).
The group under study consisted of the respondents who endorsed having a panic attack (lifetime prevalence) (N=425). Panic attack and panic disorder are collapsed because there is no meaningful cutoff point in epidemiologic and clinical data that distinguishes panic attack from panic disorder in terms of panic attack symptoms or associated social morbidity
(12). Diagnoses were generated from a modified version of the World Health Organization Composite International Diagnostic Interview
(13), a structured interview designed for use by lay interviewers.
At the end of the diagnostic sections for each of five types of disorders, respondents were asked whether they ever told a medical doctor other than a psychiatrist (M.D., D.O., or a student in training to become an M.D. or D.O.), a mental health specialist (a psychiatrist, psychologist, or social worker), or any other professional (a nurse, minister, priest, rabbi, or counselor) about the problems discussed in that section of the interview. Positive responses were followed by probes for the age when the respondent first told each type of professional. Age at first treatment was quantified by the variable documenting earliest age at which the respondent told a professional about a panic attack.
We used Pearson’s chi-square tests to determine sociodemographic differences between respondents who were or were not treated for panic among those who experienced onset of panic attack before the onset of major depressive disorder (lifetime) and those who experienced panic attacks without experiencing lifetime major depressive disorder. A Cox proportional hazard model was then used to calculate unadjusted and adjusted hazards ratios (with 95% confidence intervals [CIs]) estimating the effect of treatment of panic attacks on the risk of developing major depressive disorder.
Results
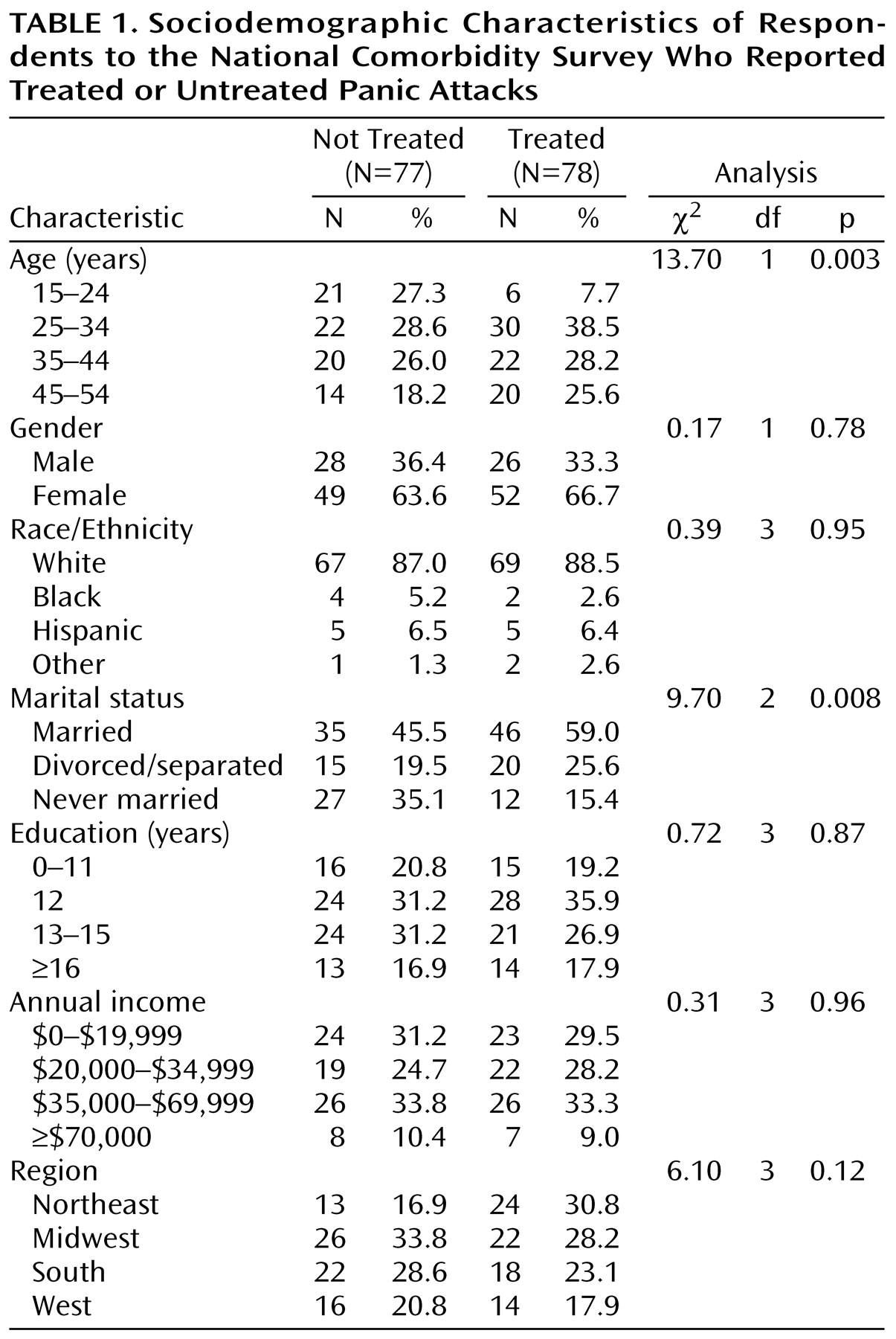
Compared with respondents who experienced panic attacks and did not receive treatment, those who were treated were older, more likely to be married, and less likely never to have married (
Table 1).
Approximately one in five (19.2%) of those who were treated for panic developed major depression. By contrast, nearly half (44.7%) of those who had not been treated developed major depression (χ2=11.5, df=1, p=0.001). Consistent with these results, Cox proportional hazard analyses produced unadjusted and adjusted hazards ratios showing that individuals who were treated for panic were at lower risk for major depression; the unadjusted hazards ratio was 0.43 (95% CI=0.27–0.69), and the adjusted hazards ratio was 0.47 (95% CI=0.28–0.78). Similar results were produced when the model was rerun to estimate the risk of major depression only among individuals who met full criteria for panic disorder: the unadjusted hazards ratio was 0.52 (95% CI=0.30–0.91), and the adjusted hazards ratio was 0.58 (95% CI=0.32–1.00).
Discussion
Treatment of panic attack may be a roadblock or a detour on the pathway from panic symptoms to major depression. In this regard, it is interesting to note that panic and major depression share a recommended first-line psychopharmacological treatment, i.e., selective serotonin reuptake inhibitors
(6). Alternatively, professional help-seeking may reflect unmeasured individual characteristics that protect against the development of major depression
(14). For example, telling a health care professional about panic attacks may indicate a capacity for accurate cognitive self-appraisal that helps decrease the risk of future psychiatric comorbidity
(15–
17). It is also possible that a tendency to develop depression independently reduces the likelihood of seeking treatment.
These results are preliminary and need to be interpreted within the context of several limitations. First, retrospective reports of age at onset of disorder and first treatment are subject to recall bias, although there is no reason to suspect that this would differ by group. Second, the measure of treatment for panic attacks is limited to self-report of having spoken with a health care professional about panic attacks. No information is available on the nature or effectiveness of the services provided. Third, variations in services that individuals in these groups went on to receive or had previously received could contribute to observed differences. Fourth, the crude estimates of percentages of those who developed major depression in the treated and untreated groups are unadjusted for time effects or other confounders. Finally, some of the covariates (education, marital status, and income) are time-dependent and may not be the same at the time of the onset or treatment of the disorder.
This study provides evidence for a prophylactic effect of treatment of panic attacks on the risk of major depression in the community. The findings reveal a possible pathway for prevention of depression through treatment of panic. Since we have no data on the nature or effectiveness of the treatments provided, the mechanism through which this occurs remains unknown. These data should encourage clinicians, policy makers, and health care administrators to increase efforts aimed at the detection and treatment of panic.