Empirical information concerning the relationship of spirituality to mental health is essential for understanding the role of religious values, beliefs, and practices in coping with the exigencies of life. The present study used the Spiritual Well-Being Scale
(1) and a pilot Index of Spiritual Involvement to examine associations between spirituality and personality variables and psychiatric disorders in a representative sample of Vietnam-era twin veterans. Conclusions are then drawn regarding the potential utility of these instruments for use in a program of genetic epidemiologic research on coping with major life stresses such as combat.
Method
The study sample consisted of 100 male twin pairs (49 monozygotic and 51 dizygotic) from the Vietnam Era Twin Registry
(2). The Vietnam Era Twin Registry is a nonclinical, population-based cohort, not conditioned on any medical or psychiatric disorder or treatment-seeking behavior. Because of the selective process for entry into the military, members of the Vietnam Era Twin Registry are somewhat healthier than the general population. Vietnam Era Twin Registry members are drawn from all 50 states, ensuring that the sample is geographically and demographically diverse.
Although all Vietnam Era Twin Registry members were on active duty during the Vietnam era, the current study encompasses only twins who did not serve in Vietnam, thereby eliminating the potential complicating influence of combat trauma and simplifying the interpretation of associations between spirituality and mental health variables in this preliminary investigation. Twins ranged in age at the time of study from 41 to 54 years (mean=47.2, SD=3.2). Half of the subjects were active members of an organized religious group, 36% were nonactive members, 1% were participants in nontraditional religious or spiritual groups, 6% had no interest or involvement in religion, 3% identified themselves as agnostic, and 4% identified themselves as “other.” Written informed consent was obtained from all subjects after complete description of the study.
The Spiritual Well-Being Scale
(1) consists of 10 items on religious well-being and 10 items on existential well-being. The scale defines religious well-being as a “vertical dimension” of spiritual well-being that refers to “one’s sense of well-being in relationship with God.” It defines existential well-being as a “horizontal dimension” that “connotes one’s perception of life’s purpose and satisfaction apart from any specifically religious reference.”
We computed an Index of Spiritual Involvement as the sum of the standardized scores of four additional items primarily derived from the strength and practices items in the Index of Core Spiritual Experiences
(3). These four items are 1) a self-rating of the strength of one’s religious or spiritual orientation on a scale from 0 (no involvement whatsoever) to 100 (all-consuming involvement), 2) a rating from one’s twin of the strength of one’s religious or spiritual orientation on the same scale, 3) Index of Core Spiritual Experiences item 2, which concerns time spent on religious or spiritual practices, and 4) a rating of one’s own level of spirituality compared with that of “other people you have known, from the least spiritual [score=0] to the most spiritual [score=100].”
A modified version of Tellegen’s Multidimensional Personality Questionnaire
(4) was used to assess personality.
As part of an earlier assessment (1991–1992), DSM-III-R diagnostic information was obtained for axis I disorders from telephone administration of the National Institute of Mental Health Diagnostic Interview Schedule, version III, revised. For the current study, the Structured Interview for Disorders of Personality
(5) was used to assess DSM-IV personality disorders.
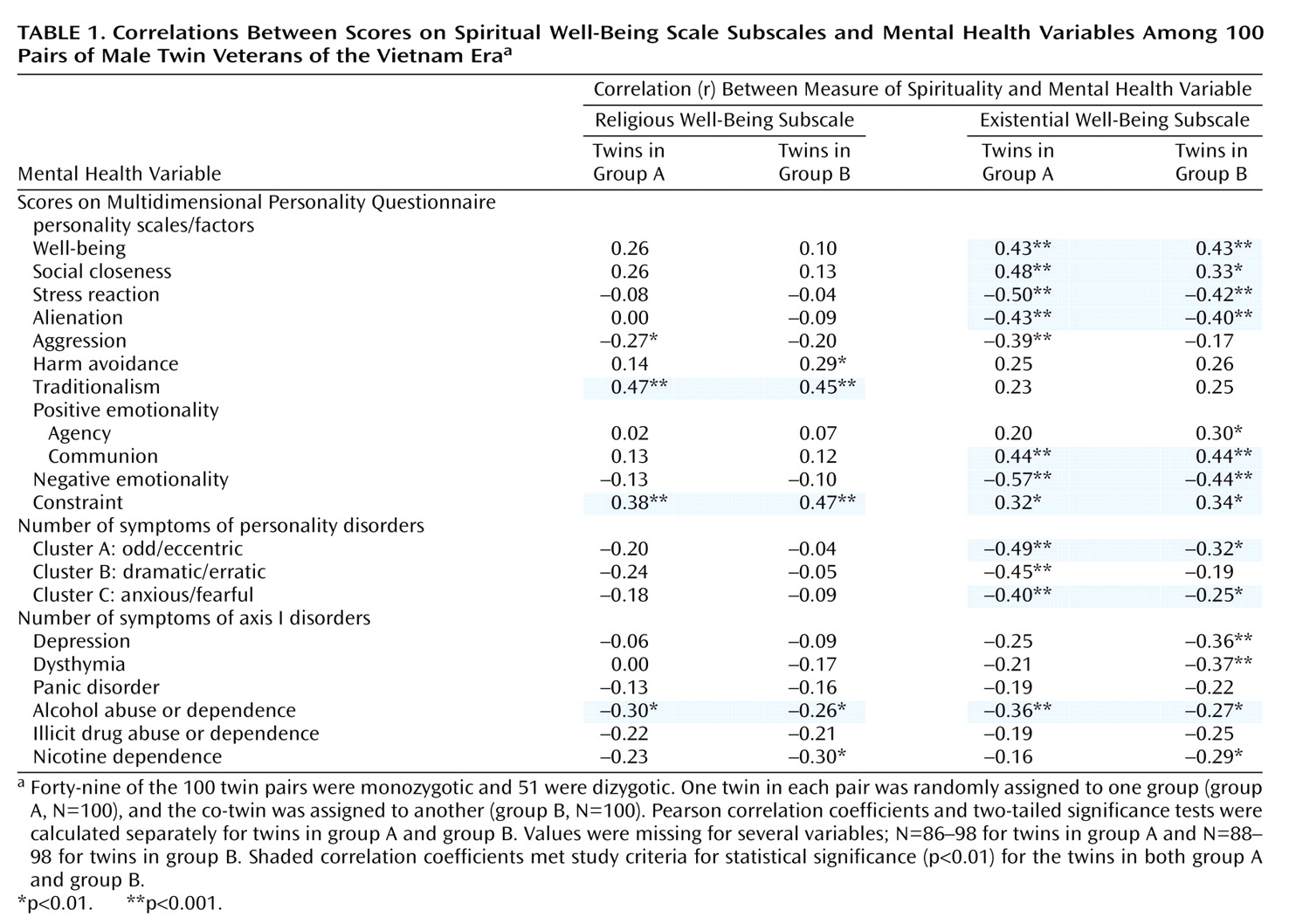
To eliminate statistical dependencies, one twin in each pair was randomly assigned to one group (group A, N=100) and the co-twin was assigned to another (group B, N=100). Pearson correlation coefficients were then calculated separately for each group. To control the type I error rate, correlations were considered statistically significant only if they reached the level of alpha=0.01 in both group A and group B. Because of the small sample size and low rate of most psychiatric disorders (under 10% except for alcohol and nicotine dependence), symptom counts rather than diagnoses were used in those analyses.
Results
Table 1 shows the associations that met study criteria for statistical significance. Most of the significant associations involve existential well-being. In contrast, religious well-being was significantly positively correlated only with traditionalism and constraint and significantly negatively correlated only with alcohol abuse or dependence. Similarly, spiritual involvement (not shown in
Table 1) was significantly correlated only with traditionalism (r=0.38, N=81, p<0.001, for twins in group A; r=0.46, N=86, p<0.001, for twins in group B) and constraint (r=0.35, N=79, p<0.01, for twins in group A; r=0.45, N=83, p<0.001, for twins in group B).
The final group of analyses examined genetic and environmental influences on spirituality and used regression models
(6) and the full sample of 100 twin pairs. Family environment accounted for 45% of the variance in spiritual involvement, and the nonfamily environment and genetic factors accounted for 32% and 23%, respectively. Genetic factors accounted for 37% of the variance in religious well-being scores, family environment explained 10% of the variance, and the nonfamily environment explained 53%. Variability in existential well-being scores was explained by either genetic factors (36% of the variance) or nonfamily environment (64%).
Discussion
The differences we observed between religious and existential well-being help clarify the potential utility of these and related constructs (such as spiritual involvement) for future genetic epidemiologic research on coping with stress in this Vietnam-era veteran population. The multiple significant correlations between existential well-being and the personality variables investigated here (including clusters of personality disorder symptoms) are consistent with the interpretation of this “horizontal” dimension of spirituality as a measure of “life purpose, life satisfaction, and positive and negative life experiences”
(7). The significant negative association with alcohol abuse and dependence was also notable but did not distinguish existential from religious well-being.
In comparison, the “vertical” aspects of spirituality that explicitly or implicitly involved religious beliefs and practices (religious well-being and spiritual involvement) were significantly associated with only a few personality variables. This suggests that this dimension reflects characteristics of the individual not associated with the measures of psychopathology that we used
(8). Religious beliefs and practices might be related to other characteristics, such as coping with adversity, not included in our pilot study.
In contrast to these findings, our analyses of genetic and environmental influences did not differentiate clearly between these aspects of spirituality. In fact, both religious and existential well-being had similar estimates of heritability. There was less evidence of a genetic influence on spiritual involvement, but these results are only suggestive in view of the relatively small sample size. It will be the task of future research to clarify the relationship of these multiple aspects of spirituality and to use that knowledge to help understand and alleviate a range of mental health concerns.