Individual Differences in a Husband and Wife Who Developed PTSD After a Motor Vehicle Accident: A Functional MRI Case Study
Initial Assessment
Case Presentations
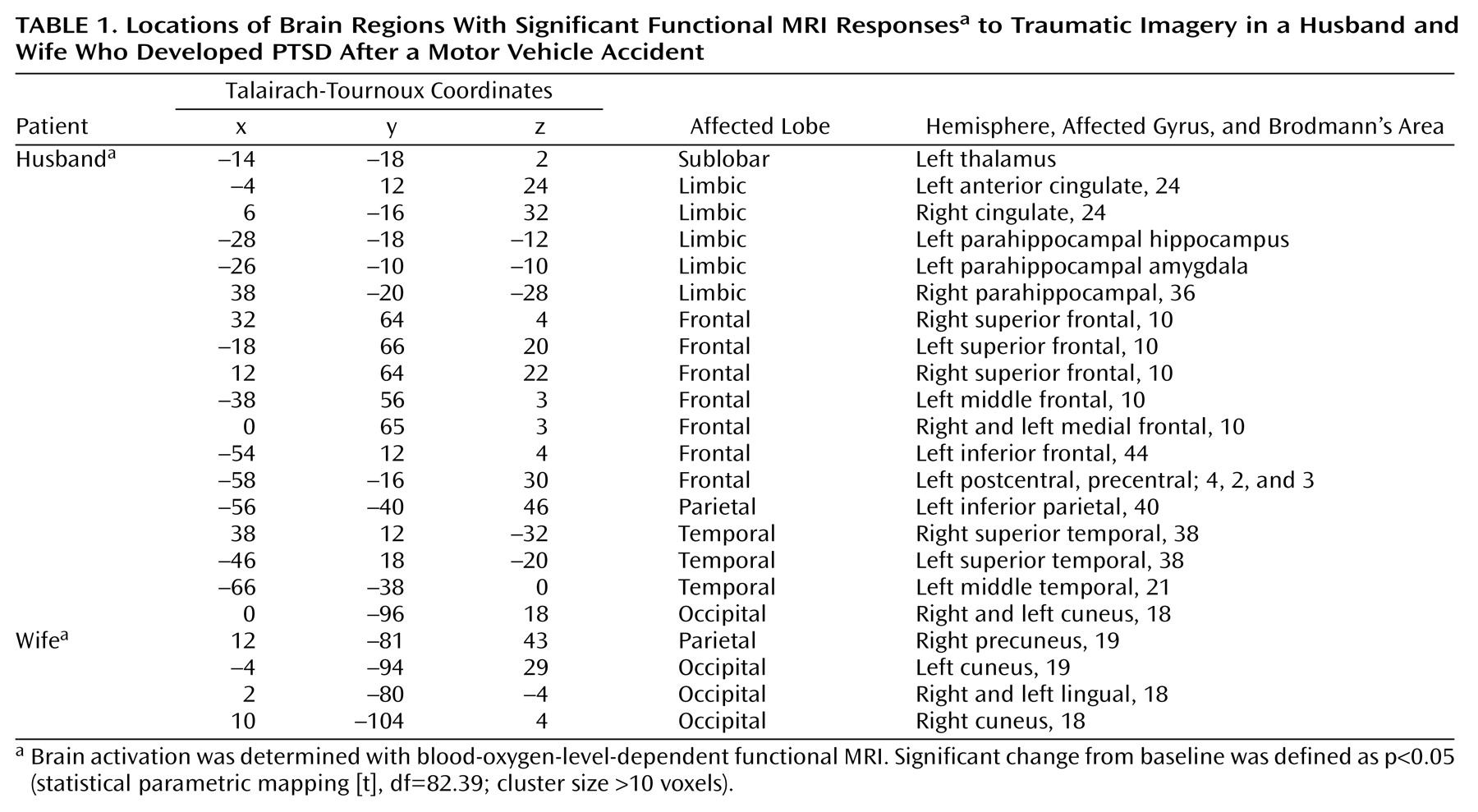
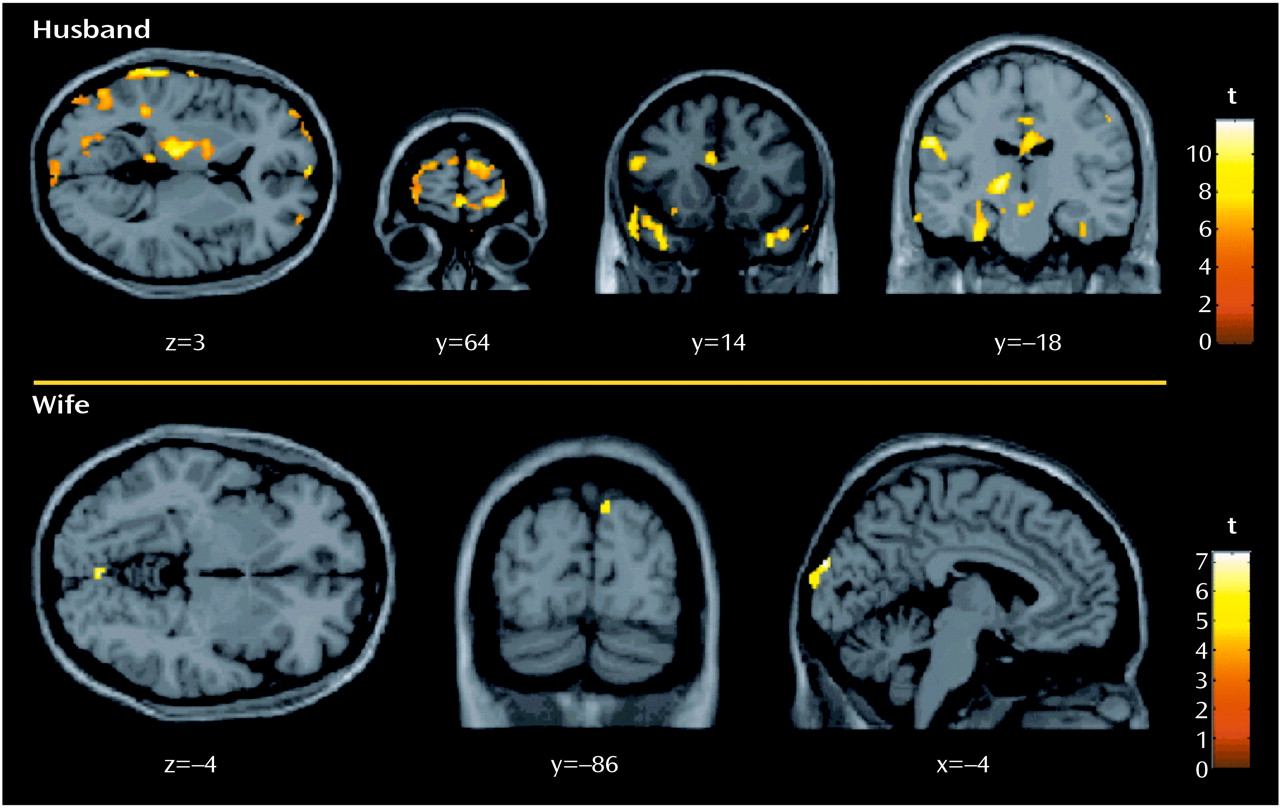
Mr. A, the husband, was a 48-year-old professional who was completely healthy until the accident. He reported feeling extremely aroused during the accident and was actively involved, both cognitively and behaviorally, in rescuing himself and his wife, ultimately breaking the windshield to allow their escape. The next day, he began experiencing flashbacks and nightmares, and his reexperiencing symptoms often included feeling as if the accident were recurring. He also became very psychologically and physiologically aroused when thinking or talking about the accident. He avoided driving on the highway where the accident occurred, as well as thoughts and conversations about it. His sleep was very poor and his concentration severely impaired, rendering him unable to function at work. Other hyperarousal symptoms were irritability and startle reactions. He reported no past or present substance abuse, past psychiatric history, or current medical problems and was not taking any medications. He reported no family psychiatric history, described his childhood as uneventful, stated he had a good relationship with his parents, and reported no history of neglect or emotional, physical, or sexual abuse. He was sociable as a child and adolescent, completed an undergraduate accounting degree, and had since worked as an accountant.Ms. A, the wife, was a 55-year-old professional who was healthy until the accident. She described being “in shock” during the accident and, although trapped but not pinned in the car, reported, “I could hardly move because I was completely frozen.” Like her husband, she began experiencing flashbacks and nightmares the next day and often felt as if it were recurring, although for her, this involved feeling “numb” and “frozen.” She avoided driving and reading newspaper stories about the accident. Her sleep was extremely poor, her concentration was significantly impaired, and she was highly irritable and easily angered. Her work functioning was completely impaired (she sold her business several months after the accident). She reported no past or present substance abuse but reported a postpartum depression after the birth of her first child and a past history of mild panic disorder. She had no medical problems and was not taking any medications. She reported no family psychiatric history but described her childhood as quite “traumatic.” That is, although she reported no history of physical or sexual abuse, her father died when she was 9 years old, and she described her mother as a very “cold” and “distant” woman with whom she did not feel safe. She was sociable while growing up, and her school performance was above average. She graduated from business school and ran a business for several years before the accident.In response to script-driven imagery of the accident, the husband reported a vivid memory that included thinking about how to escape, breaking the windshield, and feeling very anxious and “jumpy.” His heart rate increased 13 bpm from baseline. His experience corresponded to higher BOLD signals from the prescript baseline in anterior frontal, anterior cingulate, superior and medial temporal (including left amygdala), left thalamic, and parietal and occipital regions (Figure 1 and Table 1). Six months later, after a course of exposure-based treatment, he no longer had PTSD.In marked contrast—but consistent with reliving her original peritraumatic response—the wife reported feeling extremely “numb” and “frozen” while recalling the traumatic memory, and her heart rate did not change from baseline. Increases in BOLD signal intensity from baseline were only found in occipital regions (Brodmann’s areas 18 and 19) (Figure 1 and Table 1). Of importance, there were no differences in baseline brain activation between her and her husband, and her neural responses to script-driven imagery of sad and anxious memories were similar to his (data not shown). After 6 months of treatment, including prolonged exposure, she still had clinically significant PTSD. It is interesting to note that Foa (8) suggested emotional numbness to be one of the factors contributing to a lack of successful processing of trauma.
Discussion
Footnote
References
Information & Authors
Information
Published In


History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).