Three medications—lithium, divalproex, and olanzapine—have demonstrated efficacy in the treatment of acute bipolar mania in two or more randomized, placebo-controlled trials
(1–
8). In addition, carbamazepine and chlorpromazine were superior to placebo in treatment of acute mania in small clinical trials
(9,
10). Despite the array of medications available to treat acute mania, many patients fail to respond adequately to monotherapy with these agents or experience treatment-limiting side effects
(11).
Ziprasidone is an atypical antipsychotic agent with a unique receptor-binding profile. It is a potent antagonist of both serotonin 2A (5-HT
2A) and dopamine D
2 receptors, with an affinity for 5-HT
2A receptors approximately 1,000-fold higher than that for D
2 receptors. Ziprasidone also has high affinity for 5-HT
1A receptors, where it acts as an agonist, and for 5-HT
1D and 5-HT
2C receptors
(12). In addition, ziprasidone appears to inhibit reuptake of serotonin and norepinephrine
(12). Studies in individuals with schizophrenia and schizoaffective disorder have shown that ziprasidone improves positive, negative, and associated depressive symptoms
(13–
15). In an analysis of ziprasidone’s thymoleptic activity in patients with schizoaffective disorder (bipolar and depressive subtypes), ziprasidone exerted dose-related reductions in manic and depressive symptoms compared with placebo
(16). Pooled tolerability data from placebo-controlled trials demonstrated a favorable overall tolerability for ziprasidone
(17), and the agent appears to be less likely to induce weight gain than other atypical antipsychotics, including clozapine, olanzapine, quetiapine, and risperidone
(18).
Based on preliminary evidence of the efficacy of ziprasidone in improving mood symptoms, as well as psychotic symptoms
(13–
16), we conducted a large, randomized, controlled trial evaluating the efficacy and tolerability of ziprasidone as monotherapy for acute bipolar mania.
Method
Design
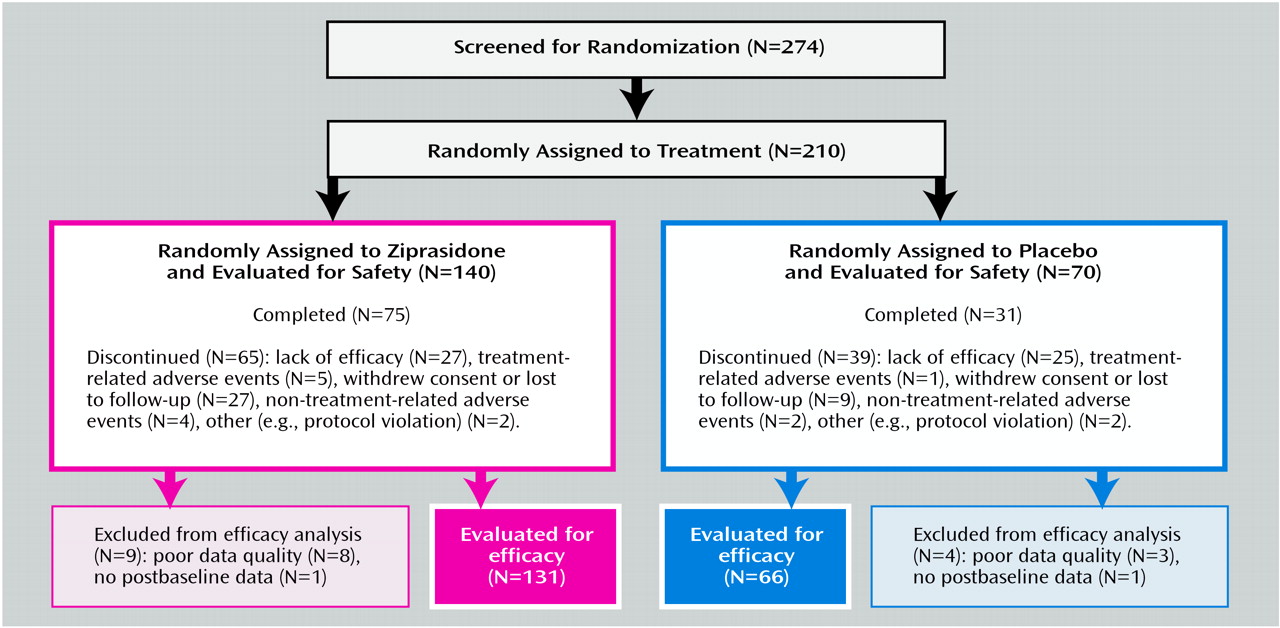
The efficacy and tolerability of oral ziprasidone was assessed in a 3-week, double-blind, placebo-controlled, randomized, parallel-group, multicenter trial (21 U.S. and three Brazilian sites) involving 210 inpatients.
Inclusion and Exclusion Criteria
Men and women >18 years of age with a primary DSM-IV diagnosis of bipolar I disorder and a current manic or mixed episode, confirmed by the Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-P)
(19), were eligible for study participation. Patients were required to have a Mania Rating Scale
(20) total score ≥14, with a score ≥2 on at least four items at screening and at baseline (within 12 hours before the first dose of double-blind medication).
Patients with schizophrenia, schizoaffective disorder, or acute bipolar I disorder with a current depressed episode were excluded from the study. Other exclusion criteria included DSM-IV-defined substance or alcohol abuse or dependence within the preceding 2 months and treatment with clozapine within 12 weeks, a depot antipsychotic within 4 weeks, or a monoamine oxidase inhibitor within 2 weeks of study baseline. Patients considered at high risk for suicide or violence were also excluded.
Women of childbearing age were eligible if they had undergone bilateral tubal ligation, hysterectomy, or bilateral total oophorectomy, were 1 year postmenopausal, or had tested negative at screening on a serum pregnancy test and had agreed to use investigator-approved contraceptive methods throughout the study. At screening, eligible patients were without clinically significant laboratory and ECG abnormalities and were 80% to 140% of ideal weight for sex, height, and frame as established in the Metropolitan Life Insurance Height and Weight Tables
(21).
Patients with a history of clinically significant and currently relevant hematologic, renal, hepatic, gastrointestinal, endocrine, pulmonary, dermatologic, oncologic, or neurologic (including seizures or epilepsy) disease were excluded. Also ineligible were subjects with a history of significant cardiovascular disease, bypass surgery, or concurrent cardiovascular disease, including uncontrolled hypertension, hypotension, congestive heart failure, angina pectoris, or recent myocardial infarction (within the past 6 months). Anyone with a history of chronic hepatitis or with serologic evidence of acute or chronic hepatitis (positive hepatitis B surface antigen [HBsAg]) or hepatitis C antibodies and elevated liver enzymes, as well as those known to be infected with the human immunodeficiency virus, was also excluded.
Other reasons for exclusion included a history of hypersensitivity to antipsychotic compounds, a history of neuroleptic malignant syndrome developing from the administration of antipsychotic compounds, use of phencyclidine at any time during the 30-day period immediately preceding screening, use of any investigational drug within 4 weeks before screening, and treatment with ziprasidone in a previous clinical trial.
This study was conducted in compliance with the ethical principles originating from the 1989 Declaration of Helsinki. After complete description of the study, written informed consent was obtained from all participating patients.
Treatments
During screening, patients discontinued all psychotropic drugs except lorazepam, temazepam, and medications to manage movement disorders. Benzodiazepines other than lorazepam or temazepam were permitted only with the approval of a clinician employed by the sponsor (Pfizer Inc.) to monitor the study. Patients received single-blind placebo during a 1–7-day washout period. Patients were then randomly assigned in a 2:1 ratio to receive oral ziprasidone or placebo over a 3-week, double-blind treatment phase. Before the start of the study, we prepared a randomization list indicating the treatment assignment for each subject number. Drug treatment cards were numbered for each patient entering the double-blind phase, and the investigator or pharmacist allocated numbers to patients in sequence of entry into the study.
Ziprasidone (given with meals) was started at 40 mg b.i.d. on day 1, increased to 80 mg b.i.d. on day 2, and adjusted by a maximum of 40 mg/day within the range of 80–160 mg/day during the course of the trial. Placebo was given as matching capsules.
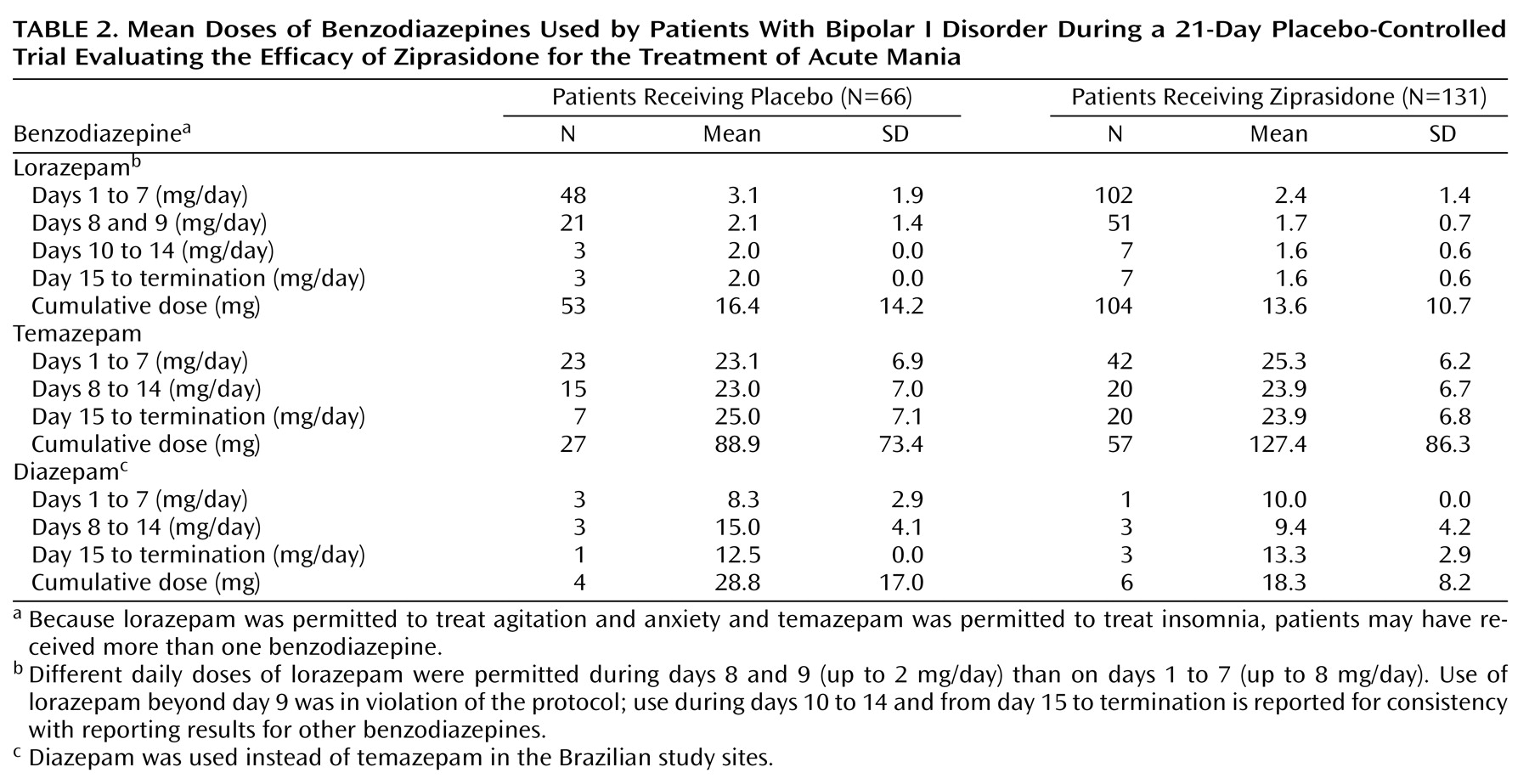
Lorazepam was permitted to treat agitation and anxiety (up to 8 mg/day from day 1 to day 7, up to 2 mg/day on days 8 and 9, and then discontinued). Temazepam (up to 30 mg/day) or, in the three Brazilian study centers, diazepam (up to 15 mg/day) was permitted as needed up to 3 days a week for insomnia throughout the study. None of these medications was permitted within 4 hours of study assessments, and a record was kept of the frequency of administration and the dose administered. The only other related medications allowed during double-blind treatment were benztropine and propranolol, which were given as needed for the management of Parkinsonian side effects and akathisia, respectively.
Evaluations
Efficacy
Efficacy was assessed by using the following instruments: Schedule for Affective Disorders and Schizophrenia, Change Version (SADS-C
[20], which contains the Mania Rating Scale), Positive and Negative Syndrome Scale
(22), investigator-rated Clinical Global Impression (CGI) severity scale
(23), investigator-rated CGI improvement scale
(23), and Global Assessment of Functioning Scale
(23). Raters were blind to patients’ study medication. The SADS-C, CGI severity scale, and CGI improvement scale were administered at screening (except for the CGI improvement scale), at baseline (day 1, within 12 hours before the first dose), and on days 2, 4, 7, 14, and 21 (or at study termination, within 12 hours after the final dose). The Positive and Negative Syndrome Scale and Global Assessment of Functioning Scale were administered at baseline and on days 7, 14, and 21 (or at study termination). Sites were standardized on use of the SADS-C at an investigator meeting where videotaped interviews were rated and discussed.
Safety and tolerability
All observed or reported adverse events, including illnesses with onset during the study or exacerbations of preexisting illnesses, were recorded. Adverse events were evaluated for severity, duration, and possible relation to the study drug.
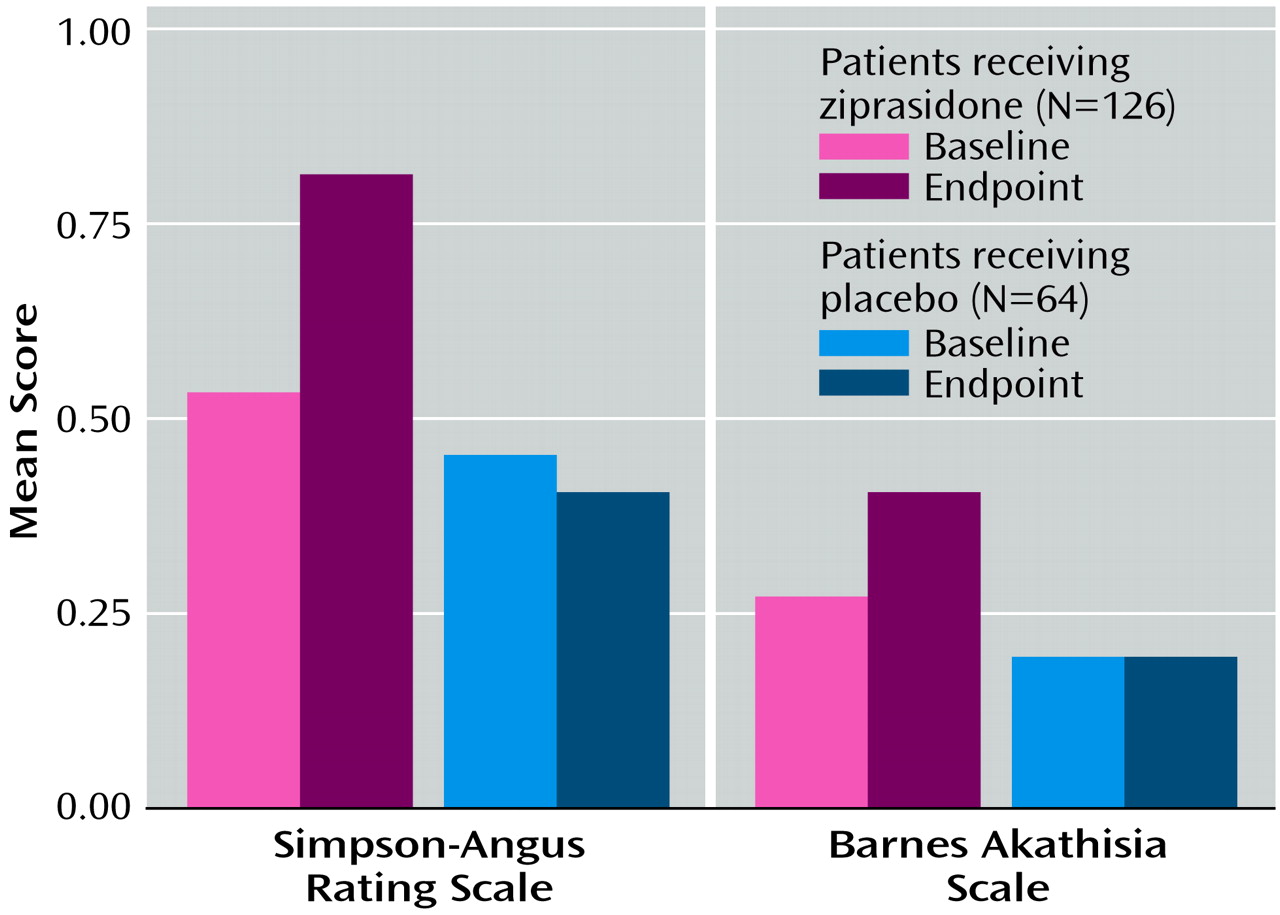
Parkinsonism was assessed with the Simpson-Angus Rating Scale
(24) at screening, baseline, day 7, and day 21 (or study termination). Akathisia was evaluated with the Barnes akathisia rating scale
(25) at the same times. Abnormal involuntary movements were assessed with the Abnormal Involuntary Movement Scale (AIMS)
(23) at screening, baseline, and study endpoint. Treatment-emergent dystonic movements were recorded as adverse events, and the use of concomitant therapy for movement disorders (benztropine or propranolol) was recorded.
Laboratory assessments done only at screening included urine drug screening, hepatitis battery (HBsAg, hepatitis C antibodies), and plasma concentrations of lithium, carbamazepine, or valproate for patients receiving these medications at study entry. Tests performed at both screening and study endpoint included urinalysis, complete blood count with differential and platelet count, and blood chemistry, including thyroxine and thyroid-stimulating hormone. Blood pressure and pulse rate were measured at each visit, including screening, baseline, and study endpoint. A physical examination, including body weight measurement, and a 12-lead ECG were also performed at these times.
Data Analysis
The size of the study group was estimated on the basis of Mania Rating Scale parameters. A difference of 5 points on the Mania Rating Scale between treatment groups was deemed to be the smallest clinically relevant difference in endpoint values. The standard deviation of the Mania Rating Scale was expected to be less than 11.5. On the basis of these parameters, a study group of 200 subjects (133 taking ziprasidone and 67 taking placebo) was necessary to provide at least 80% power (alpha=0.05, two-tailed) to detect such a mean difference.
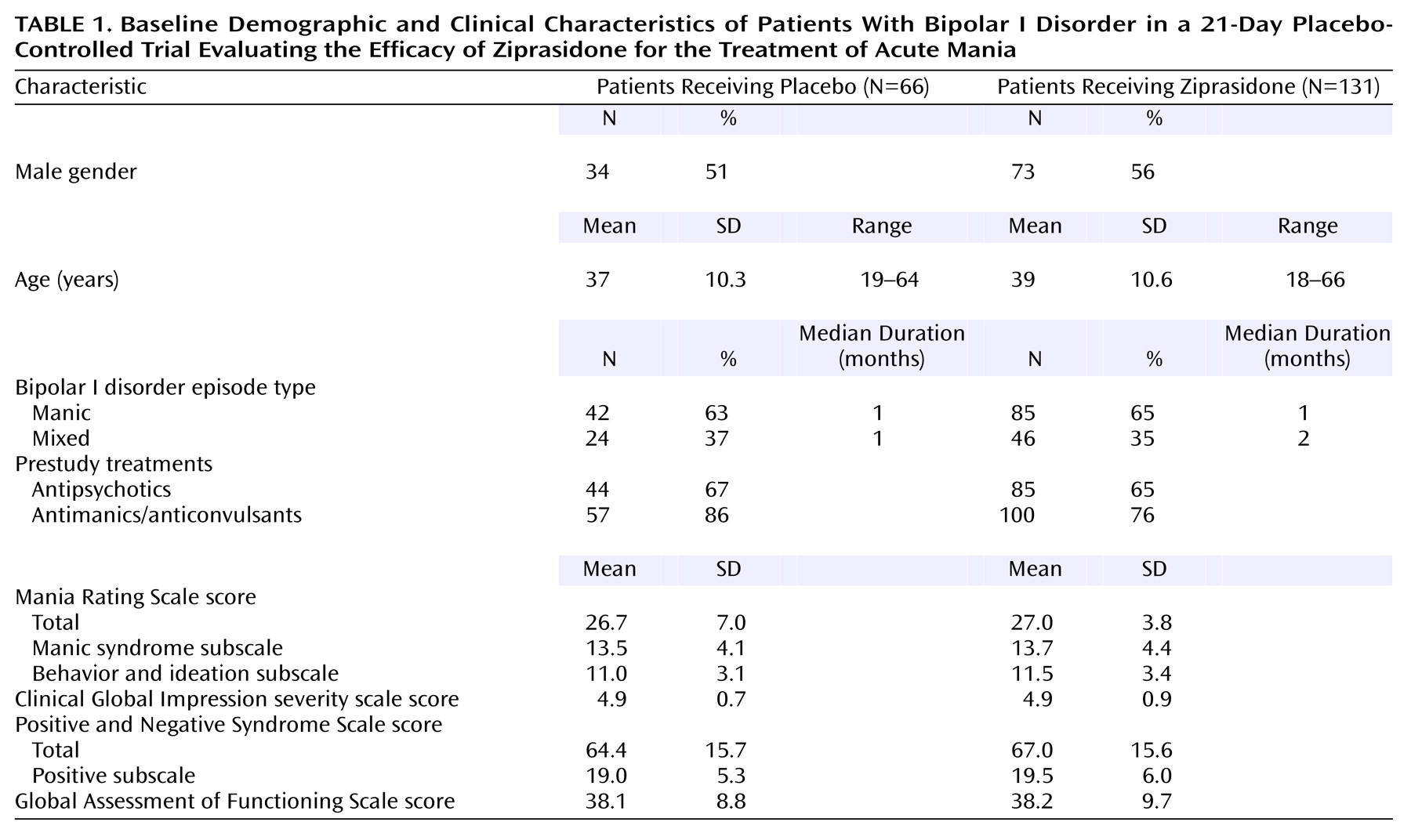
Background and demographic data were recorded and compared at baseline to ensure balance between the two treatment groups.
Efficacy analyses were performed on an intent-to-treat basis. All comparisons between the two treatment groups were analyzed for significance at the two-tailed 0.05 level. When appropriate, the last observation was carried forward to interpolate missing data.
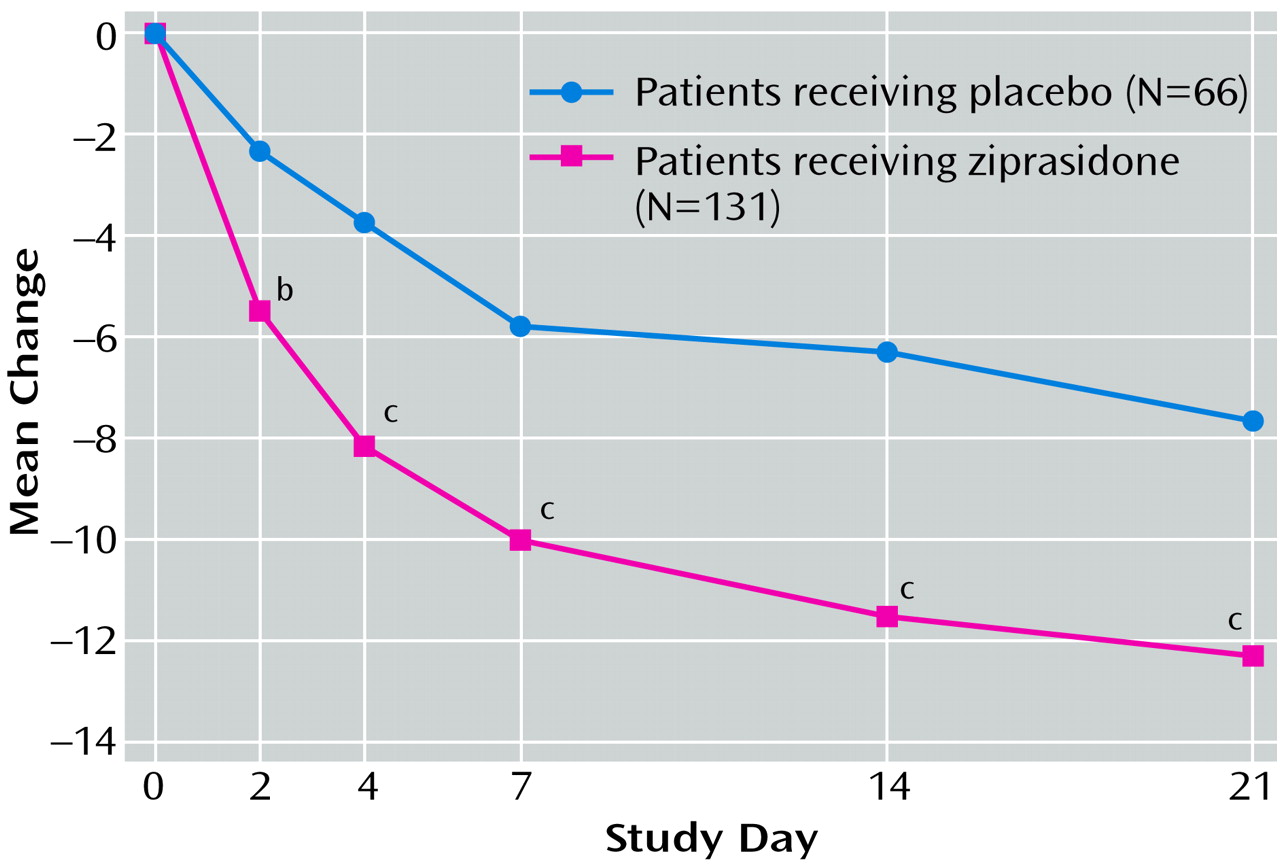
Primary efficacy analyses were the differences from baseline to endpoint in mean Mania Rating Scale and CGI severity scale scores between the ziprasidone and placebo groups. These variables were assessed by using analysis of covariance (ANCOVA) models that included terms for study center, treatment, and the center-by-treatment interaction, with the baseline score used as a covariate.
Patients were identified as responders (decrease in Mania Rating Scale score ≥50% from baseline to specific time point) or nonresponders (decrease in Mania Rating Scale score <50% from baseline to specific time point) at each nominal protocol visit and endpoint visit (day 21 or termination). The treatment groups were compared by using a Cochran-Mantel-Haenszel test statistic with stratification by center.
Secondary efficacy analyses included the difference between the ziprasidone and placebo groups in mean changes from baseline to endpoint in scores on the manic syndrome subscale and behavior and ideation subscale of the Mania Rating Scale, the positive and total scores on the Positive and Negative Syndrome Scale, and the Global Assessment of Functioning Scale score. Groups were compared with respect to these variables by using ANCOVA, as described earlier. The mean CGI improvement scale scores at endpoint for the ziprasidone and placebo groups were also compared by using ANCOVA models.
Descriptive statistics were applied to clinical and laboratory safety data for each within-group parameter. These were then evaluated on the basis of tabular and graphic displays.
Discussion
In this study, ziprasidone was effective and well tolerated in patients with acute mania. Compared with placebo, ziprasidone treatment produced rapid and sustained improvement from baseline in the primary outcome measures of the Mania Rating Scale and CGI severity scale scores, with significant changes in these indices observed as early as the second day of treatment. Ziprasidone treatment was associated with significant improvement in scores on the manic syndrome and behavior and ideation subscales of the Mania Rating Scale by day 2. The mean change in Mania Rating Scale scores from baseline to endpoint in the ziprasidone group represented a 45% improvement. This change is comparable with the 37% and 51% reductions in the Young Mania Rating Scale score previously observed in 3-week and 4-week placebo-controlled trials of olanzapine in acute mania
(3,
4). Similarly, a median 54% decrease was observed in a 3-week placebo-controlled trial of valproate
(2). In a 3-week trial of divalproex, lithium, and placebo, both the divalproex group and the lithium group exhibited an approximately 35% improvement in the Mania Rating Scale score
(1). However, magnitudes of improvement exhibited by agents in different trials must be compared cautiously, particularly when different instruments for rating mania have been employed.
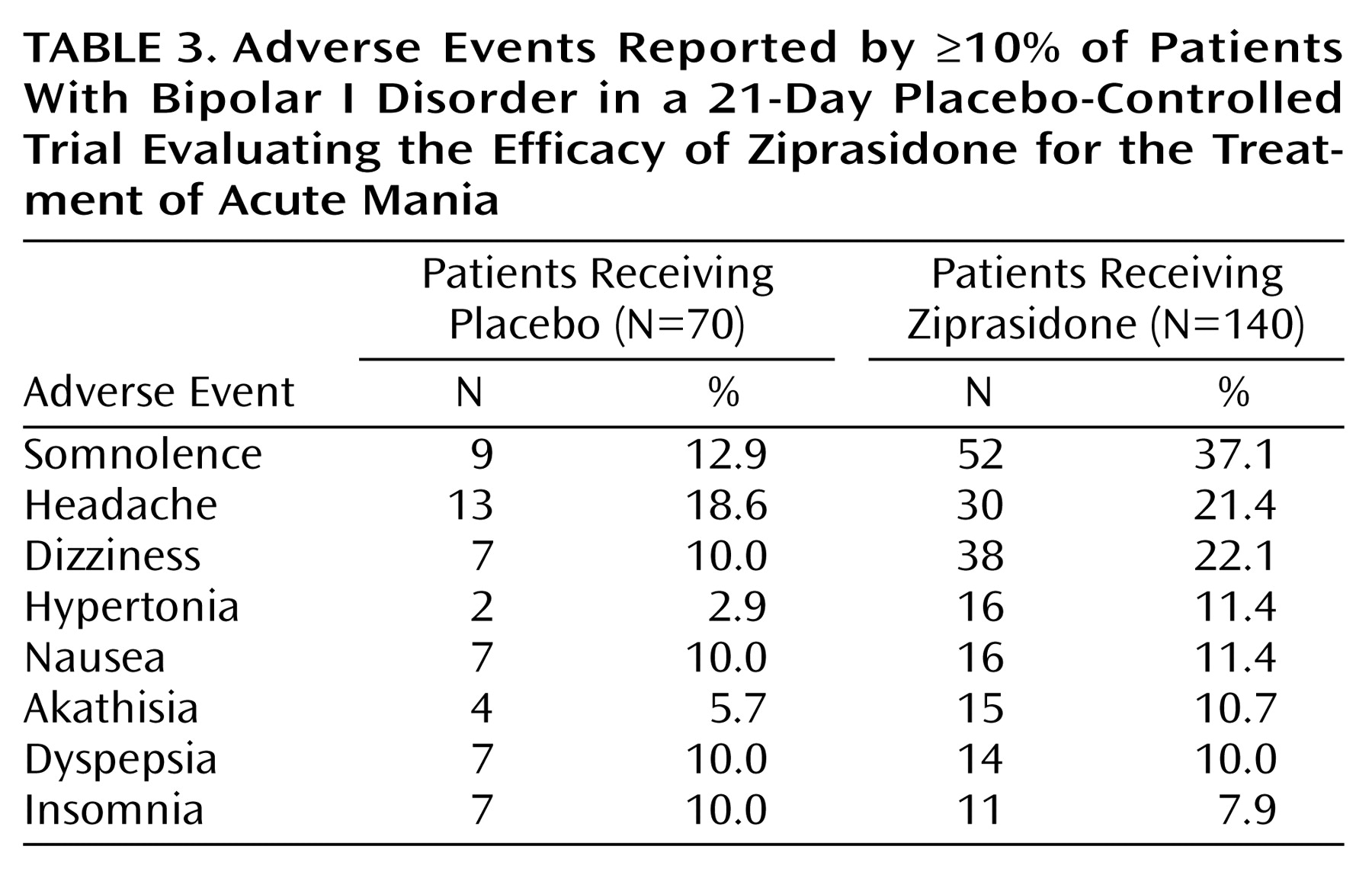
Ziprasidone was well tolerated. The adverse events that were reported most frequently in the ziprasidone group, and more frequently in the ziprasidone group than in the placebo group, were somnolence, headache, and dizziness. Reports of movement disorders were uncommon, and observed changes on objective rating scales were generally comparable between the ziprasidone- and placebo-treated patients. Ziprasidone was not associated with weight gain or clinically significant ECG changes. The mean increase in QTc interval in this study was similar to the increase observed in clinical trials of ziprasidone in patients with schizophrenia and schizoaffective disorder
(13–
15). No patient had a QTc interval ≥500 msec while taking ziprasidone.
The tolerability profile of ziprasidone in this study is consistent with its pharmacologic activity and the generally favorable profile described for this agent in trials of patients with schizophrenia and schizoaffective disorder
(13–
15). These trials indicated a low incidence of specific adverse events commonly associated with antipsychotics such as weight gain, postural hypotension, anticholinergic side effects, and extrapyramidal symptom side effects
(13–
15,
17). The low incidence of extrapyramidal symptoms observed with ziprasidone compared with typical antipsychotics is a characteristic shared by other atypical agents
(26–
28) and has been attributed to the higher affinity of these drugs for 5-HT
2A receptors than for D
2 receptors
(29).
In this study, the ziprasidone- and placebo-treated patients displayed a comparable requirement for supplementary benzodiazepine medication, as measured by both mean daily doses and cumulative doses. Thus, had the beneficial effects of ziprasidone in improving manic symptoms been due largely to the use of benzodiazepines, the placebo-treated patients would have experienced similar improvements. Instead, compared with placebo recipients, ziprasidone-treated patients demonstrated significant improvements on outcome measures as early as day 2 of treatment.
In summary, this double-blind, placebo-controlled study demonstrated that ziprasidone is effective and well tolerated in patients with bipolar I disorder who are experiencing acute mania. Ziprasidone therapy produced rapid and sustained improvement from baseline compared with placebo on all primary and the majority of secondary efficacy measures, thus demonstrating its capacity to ameliorate a wide range of symptoms in patients with mania. Significant improvements were typically observed by the second day of treatment and were maintained for the duration of the trial. Ziprasidone was generally well tolerated, was associated with a low rate of extrapyramidal symptoms, and was not associated with weight gain or clinically significant ECG abnormalities. These results suggest that ziprasidone is effective as monotherapy in the treatment of patients with bipolar mania.