Subjects
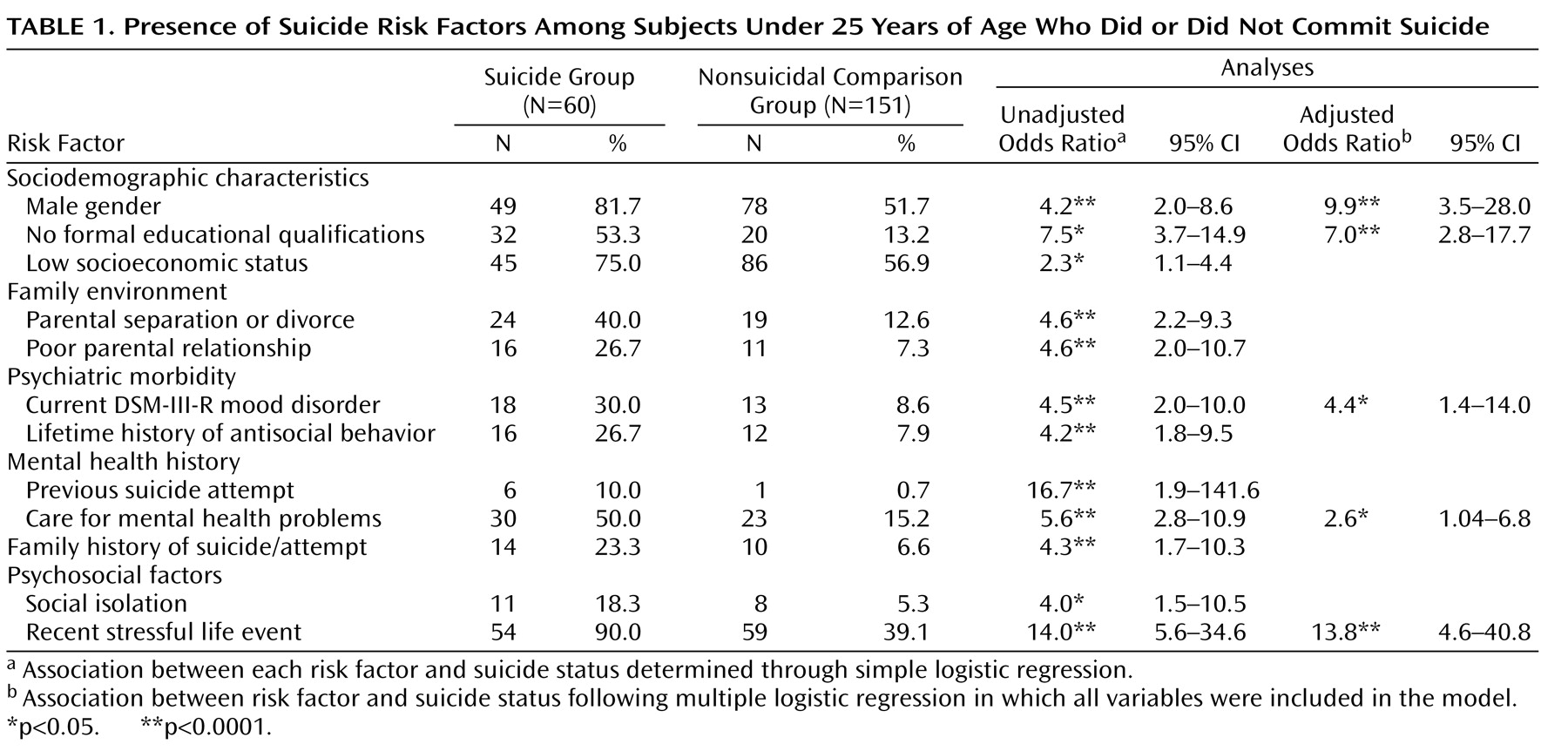
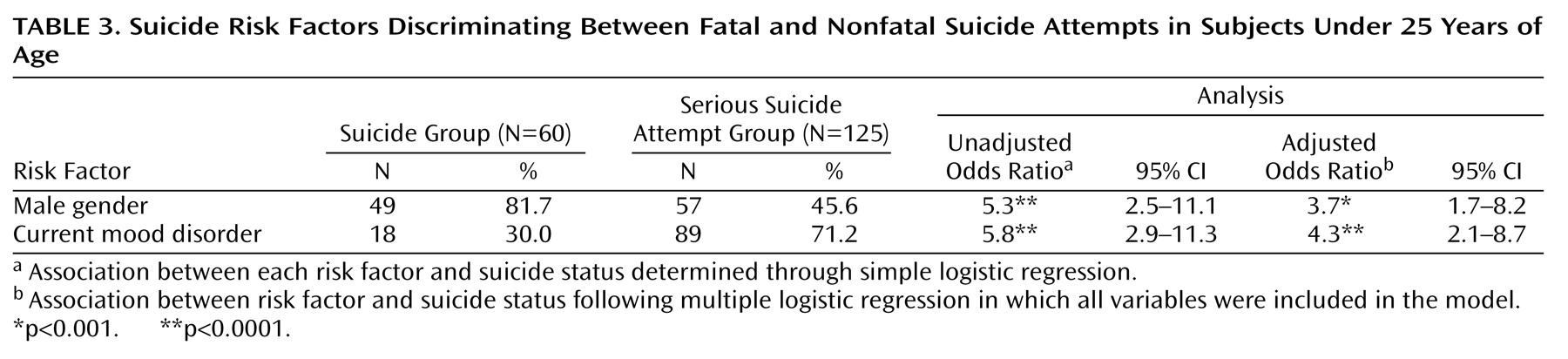
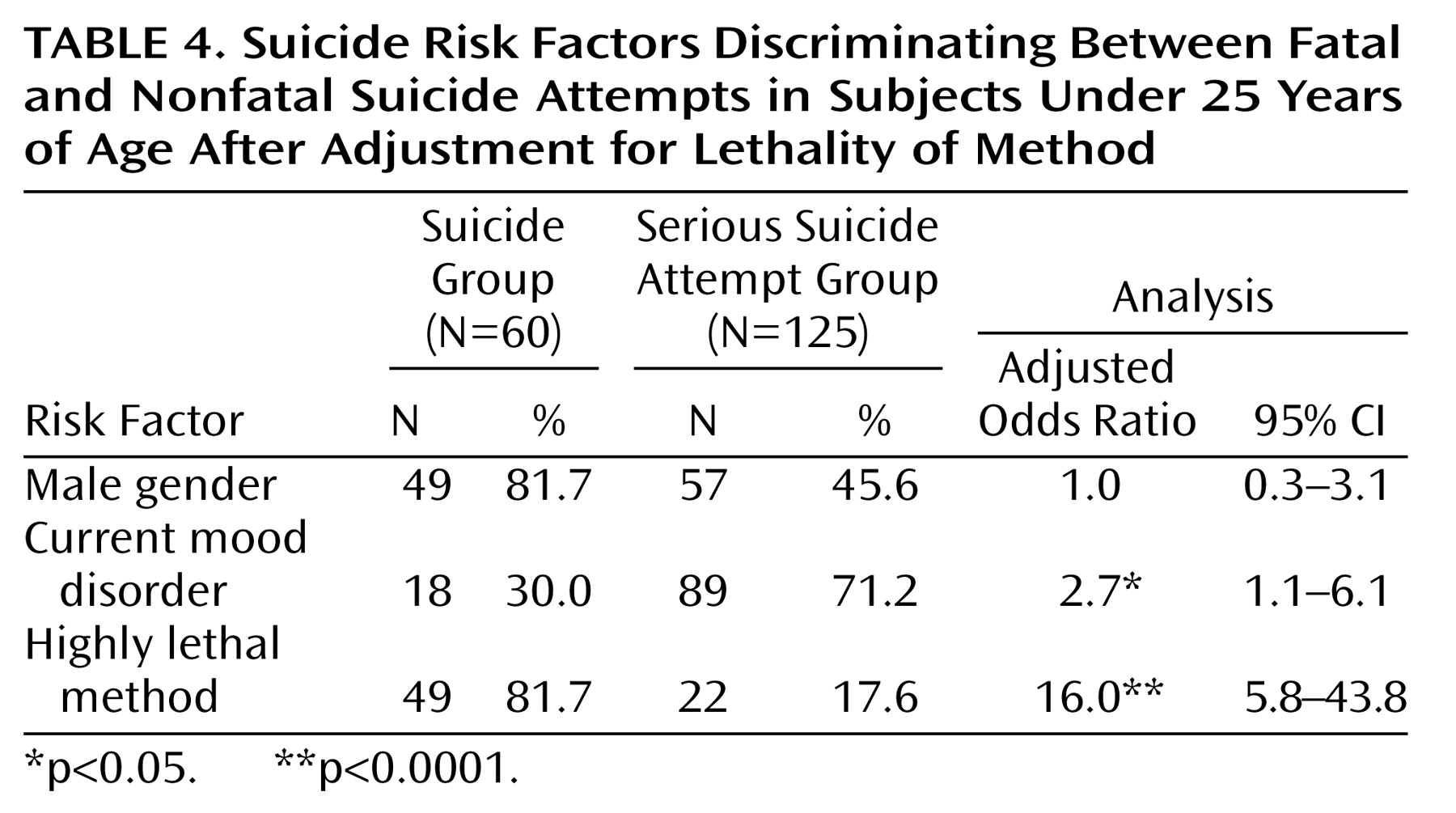
The suicide group was a consecutive series of 60 subjects under 25 years of age from the Christchurch city and Canterbury region in New Zealand who, according to coroners’ verdicts, committed suicide during the period from 1991 to 1995. Christchurch city has a population of 315,000, and the Canterbury region has a population (including Christchurch city) of approximately 430,000. During the study period, 64 individuals under 25 committed suicide; the families of 60 agreed to participate in the study, a response rate of 93.8%. Of these 60 individuals, 49 (81.7%) were male, and 11 (18.3%) were female. Their mean age was 19.98 years (SD=2.53, range=14–24). Methods of suicide included hanging (41.7%, N=25), vehicle exhaust gas (31.7%, N=19), self-poisoning (15.0%, N=9), and firearms (8.3%, N=5).
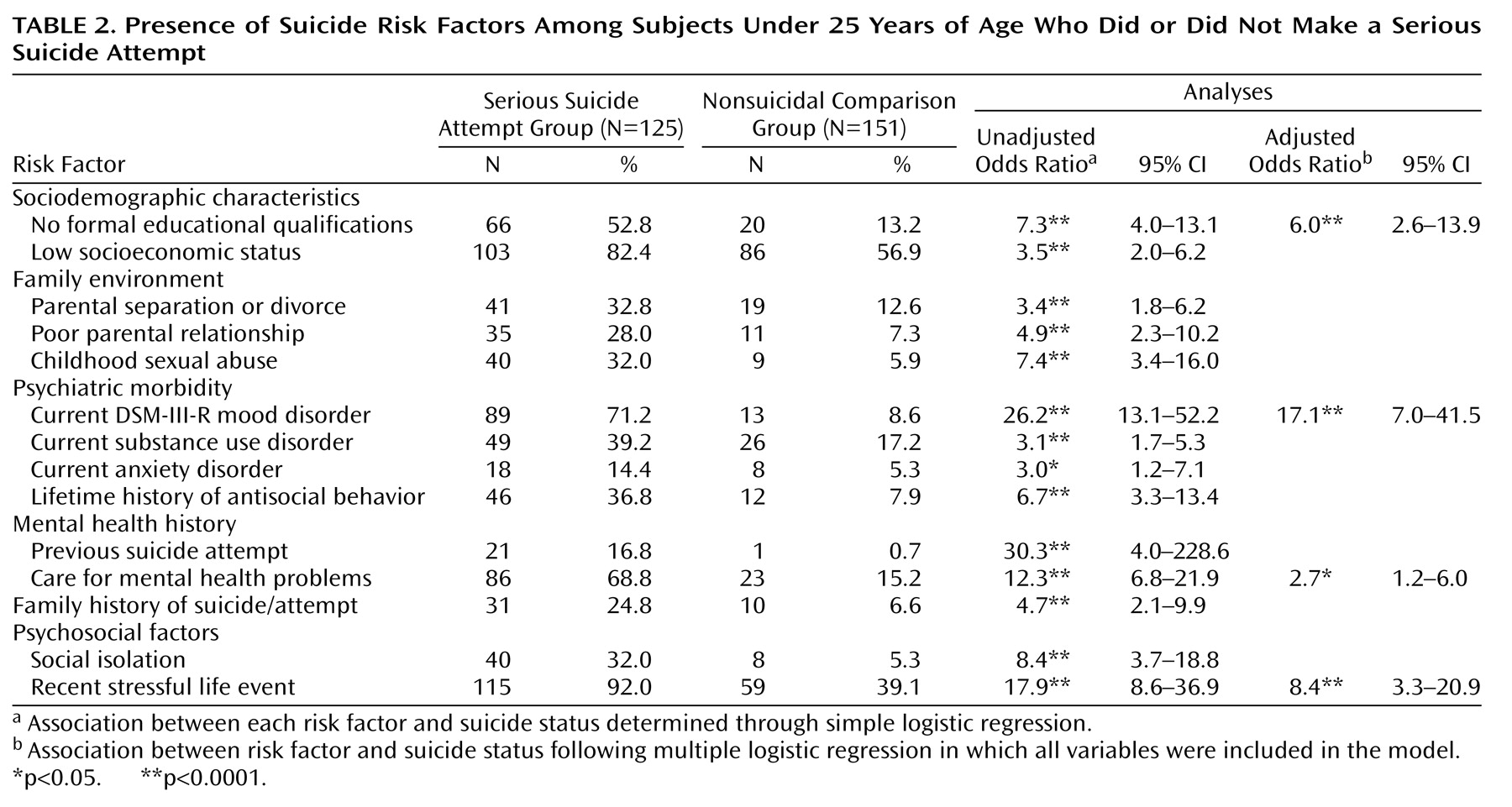
The medically serious suicide attempt group was a consecutive series of 125 individuals under 25 years of age from the Christchurch city and Canterbury region who made medically serious suicide attempts during the period from 1991 to 1994. A medically serious suicide attempt was defined as one that required hospital admission, via the sole regional Emergency Department, for >24 hours and met one of the following treatment criteria: 1) treatment in specialized units; 2) surgery under general anesthesia (superficial cuts that did not require surgical repair were excluded); or 3) extensive medical treatment, including antidotes for drug overdoses, telemetry, or repeated tests or investigations. In addition, individuals who attempted suicide by methods with a high risk of fatality, specifically, hanging or gunshot, who were hospitalized for >24 hours but did not meet the preceding treatment criteria, were also included in the group of persons with serious suicide attempts.
In total, 132 individuals made serious suicide attempts during the study period. Of these, 129 agreed to participate in the study, with 125 (96.9%) agreeing to interview information being obtained from a significant other. Of these 125 individuals, 57 (45.6%) were male, and 68 (54.4%) were female. Their mean age was 19.31 years (SD=3.1, range=13–24). Methods of serious suicide attempt included self-poisoning (77.6%, N=97), vehicle exhaust gas (11.2%, N=14), hanging (2.4%, N=3), and firearms (2.4%, N=3).
The comparison subjects for this analysis were a stratum of the comparison series from the larger study of suicidal behavior, which had been selected from regional electoral rolls. An age- and gender-stratified sample was obtained for six age strata (18–24, 25–29, 30–39, 40–49, 50–59, ≥60), with the number of subjects in each age-and-gender stratum proportional to the known age-by-gender distribution of the population 18 years of age and older. A total of 153 subjects 18–24 years of age were selected as part of the stratified sample. Of these, 151 agreed to information being obtained from a significant other, a response rate of 98.7% for significant other informants. Of these, 51.7% (N=78) were male, and 48.3% (N=73) were female. Their mean age was 21.43 years (SD=1.52, range=18–24).
Subjects selected from electoral rolls were mailed a letter of introduction explaining the study. The study interviewer then called at subjects’ homes, discussed the study, and arranged to return to conduct an interview. Each subject nominated a significant other who knew him or her well. This individual was then contacted and interviewed in person.
The study was approved by ethics committees of the Canterbury Area Health Board and the Southern Regional Health Authority. Written informed consent was obtained from all study participants after the aims and procedures of the study had been fully explained.
Risk Factors
Trained, experienced interviewers personally conducted a semistructured interview with each subject’s significant other to retrospectively construct a life history and to obtain information about risk factors for suicidal behavior.
Lethality of method
Method of suicide or suicide attempt was classified into two groups: highly lethal (hanging, vehicle exhaust gas, firearms, jumping) and less lethal (self-poisoning, cutting, and all other methods).
Sociodemographic characteristics
Two areas were assessed: socioeconomic status and educational level. Socioeconomic status was measured with the scale for socioeconomic status in New Zealand
(30), which ranks the population into six groups on the basis of occupation. For the purposes of this analysis, socioeconomic status was dichotomized to give a measure of “low socioeconomic status,” defined as membership in socioeconomic status classes 5 and 6. Educational level was also dichotomized to give a measure of “no formal educational qualification,” defined as no secondary school or tertiary or trade qualification.
Family environment
The presence or absence of three items was determined: 1) parental separation or divorce; 2) poor parental relationship (i.e., parents were viewed as having gotten along “not very well” or “poorly”); and 3) childhood sexual abuse. This last item was measured by asking each significant other if, to their knowledge, the subject had been “physically or psychologically forced by anyone to engage in any unwanted sexual activity, such as unwanted sexual touching of his/her body or sexual intercourse,” a definition previously used by Murphy (1985 news release from St. Cloud State University). Those who responded positively to this question were then asked further questions relating to this issue. Subjects were classified as having a history of childhood sexual abuse if there was a positive response to the initial question and subsequent questioning established a history of childhood sexual abuse.
Stressful life events
The short list of Threatening Life Experiences
(31) was used as a basis to evaluate life events that had occurred during the previous year. For the purposes of the present analysis, measures of life events were classified into a series of categories of related events: serious interpersonal difficulties, serious financial problems, serious problems with the law or police, and serious work-related problems. Subjects were classified as having a recent stressful life event if they had experienced at least one event in any of these four categories.
Psychiatric morbidity
The interviews with significant others regarding each subject included a modified version of the Structured Clinical Interview for DSM-III-R—Patient Version
(32) to generate DSM-III-R diagnoses of selected mental disorders. The information was integrated in a diagnostic conference to produce, for each subject, best-estimate diagnoses of mental disorders (according to DSM-III-R criteria). In the present analysis, four diagnostic groupings were used for disorders in the month preceding the suicide event (or interview): 1) mood disorders (major depression, bipolar I disorder, bipolar II disorder); 2) substance use disorders (alcohol, cannabis, or other psychoactive substance abuse or dependence); 3) anxiety disorders (panic disorder, agoraphobia, obsessive-compulsive disorder, simple phobia, social phobia); and 4) antisocial disorder (conduct disorder or antisocial personality disorder). For antisocial disorder, a lifetime history was obtained. Multiple axis I diagnoses were permitted.
The reliability of the best-estimate diagnostic procedure was ascertained by reevaluation of a random sample of 20% of the entire group. The test-retest agreement was high, with kappa coefficients
(33) for the principal diagnostic categories (mood disorders, substance use disorders, anxiety disorders, antisocial disorders) ranging from 0.95 to 0.99.
Mental health history
Two areas were assessed. The first was previous suicide attempts, or whether the subject had a history of at least one previous suicide attempt during his or her lifetime. The second was a history of contact or care for mental health problems, or whether the subject had at least one admission to a psychiatric hospital or substance abuse clinic during the previous year or a lifetime history of outpatient psychiatric treatment.
Social interaction
The Interview Schedule for Social Interaction
(34) was used as a basis to evaluate the extent of current social interaction. For the purposes of this analysis the measure was dichotomized to give measures of high and low social interaction.