Lower than normal thalamic volumes in schizophrenia have been shown by MRI
(1) and autopsy
(2) studies. The pulvinar constitutes one-quarter of the thalamus, is disproportionately large in primates, and has a unique developmental trajectory
(3). Three pulvinar nuclei are generally recognized
(4,
5): the inferior pulvinar, which is visual and projects to extrastriate cortex; the medial pulvinar, linked mainly to association areas of the temporal and inferior parietal lobes, and the lateral pulvinar, which shares features with both the medial and inferior pulvinar.
We know of two stereological studies of the pulvinar in schizophrenia. Byne et al.
(6) measured the right pulvinar and found a lower volume and fewer neurons than in comparison subjects. Danos and colleagues
(7) examined the medial pulvinar and found bilaterally low volumes. Small pulvinar size is also indicated by MRI findings
(8,
9). We sought to extend the evidence for pulvinar involvement in schizophrenia.
Method
Full details of the subjects and tissue processing have been reported previously
(10), as have the methods for thalamic morphometry
(11). Briefly, we studied 16 men (mean age=62 years, SD=15) and 11 women (mean age=73, SD=16) with DSM-IV schizophrenia or schizoaffective disorder and 15 male (mean age=67, SD=14) and 13 female (mean age=73, SD=14) normal comparison subjects. Their handedness was unknown. Pairs of formalin-fixed, wax-embedded 25-μm sections were taken at 2.5-mm intervals from a point anterior to the pulvinar and throughout its extent, and they were stained with cresyl violet or Weil’s myelin stain. The final group sizes ranged from 21 to 25 subjects because of missing or damaged thalamic blocks. The investigators were blind to subject details. All brains were free of neurodegenerative pathologies
(10).
Under a dissecting microscope, the inferior pulvinar was identified and excluded. The remaining pulvinar was divided into medial pulvinar and lateral pulvinar on the basis of the prominent myelinated fiber bundles within the lateral pulvinar and the resulting columnar appearance of the neurons. Our definition of the medial pulvinar included the oral nucleus. The volumes of the medial and lateral pulvinar were estimated by using the Cavalieri principle and adjusted by a factor (1.308) to correct for shrinkage during processing. Neuronal density was estimated by using the optical dissector method and Olympus CAST-Grid 2.0 software
(11) (Olympus, Albertslund, Denmark). Nuclei were examined by using a raster search pattern (1.2×1.2 mm
2 for lateral pulvinar, 1.5×1.5 mm
2 for medial pulvinar) covering the entire nucleus. The counting frame was 103×133 μm
2, with a 12-μm depth; nucleoli coming into focus within this depth were counted according to stereological rules. The number of neurons was estimated by multiplying the volume by the neuronal density. The observed coefficient of error
(12) ranged from 0.052 to 0.185.
Results
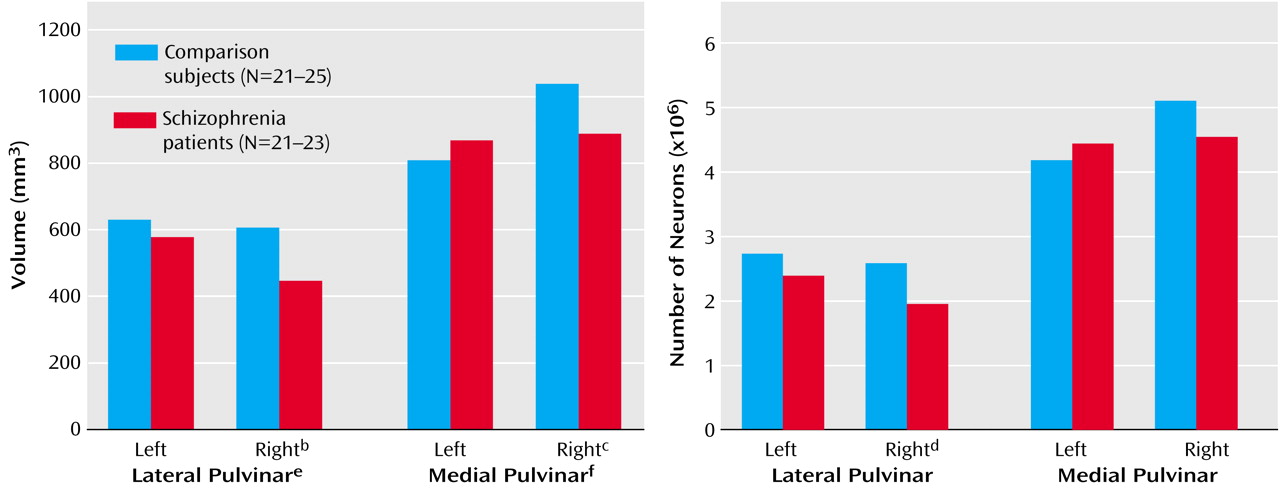
The mean volume of the left lateral pulvinar was 630 mm
3 (SD=188) in the comparison subjects and 578 mm
3 (SD=175) in the patients with schizophrenia; the mean volume of the right lateral pulvinar was 607 mm
3 (SD=208) in the comparison subjects and 447 mm
3 (SD=122) in the patients with schizophrenia (
Figure 1). Schizophrenia affected lateral pulvinar volume, as the patients had a 26% lower volume on the right but no significant difference on the left. The mean volume of the left medial pulvinar was 809 mm
3 (SD=240) in the comparison subjects and 868 mm
3 (SD=246) in the patients with schizophrenia; the mean volume of the right medial pulvinar was 1038 mm
3 (SD=231) in the comparison subjects and 888 mm
3 (SD=222) in the patients with schizophrenia. For the comparison subjects, the volume of the medial pulvinar was significantly greater on the right side than on the left (paired t test: t=6.60, df=16, p<0.001). There was a diagnosis-by-side interaction, with a 14% smaller right medial pulvinar in the schizophrenia patients.
The left lateral pulvinar contained an estimated mean 2.74×10
6 (SD=0.97) neurons in the comparison subjects and 2.40×10
6 (SD=0.88) neurons in the patients with schizophrenia; the mean estimates for the right lateral pulvinar were 2.59×10
6 (SD=1.14) in the comparison subjects and 1.96×10
6 (SD=0.60) in the patients with schizophrenia (
Figure 1). In the left medial pulvinar there were a mean of 4.19×10
6 (SD=1.29) neurons in the comparison subjects and 4.45×10
6 (SD=1.16) in the patients with schizophrenia; in the right medial pulvinar the mean estimates were 5.11×10
6 (SD=1.16) and 4.55×10
6 (SD=1.66), respectively, giving a nearly significant diagnosis-by-side interaction for medial pulvinar neuronal number (F=3.86, df=1, 30, p=0.06).
The combined mean volume for the medial plus lateral pulvinar in the comparison subjects was 1431 (SD=74) on the left and 1628 (SD=82) on the right; in the patients with schizophrenia the mean values were 1443 (SD=73) and 1311 (SD=57), respectively. This gave a significant diagnosis-by-side effect (F=8.95, df=1, 26, p=0.006), with a significantly lower volume on the right (F=12.02, df=1, 34, p=0.002) but not the left (F=0.32, df=1, 38, p=0.57) in schizophrenia. There was a diagnosis-by-side-by-nucleus interaction (F=5.14, df=1, 26, p=0.04), confirming the differential effect of schizophrenia on the medial and lateral pulvinar. The combined neuronal number for medial plus lateral pulvinar (data not shown) also showed a diagnosis-by-side interaction (F=11.13, df=1, 26, p=0.003) and a lower number on the right side in schizophrenia (F=6.53, df=1, 34, p=0.02).
There were no effects or interactions involving sex, and there were no correlations of pulvinar volume or neuronal number with autopsy delay, fixation time, or neuroleptic exposure (data not shown).
Discussion
We confirmed low pulvinar volume in schizophrenia
(6,
7) and showed that the lateral and medial pulvinar are both affected. The same result in three studies, totaling 52 patients and 49 comparison subjects, represents an unusually consistent neuropathological finding, and it is convergent with MRI data
(8,
9). Demonstration of small thalamic volumes in neuroleptic-naive patients makes medication an unlikely explanation
(9,
13,
14). The findings support a role for the thalamus in schizophrenia
(3,
15,
16), although the pathogenesis of its structural involvement remains to be elucidated.
We believe that our asymmetry finding is novel. The right medial pulvinar was larger (28% overall) than the left in all 17 of the comparison subjects for whom both medial pulvinars were available (
Figure 1); the lateral pulvinar was symmetrical. In an earlier study
(17), rightward medial pulvinar asymmetry was found in six of nine brains, although another study
(7) indicated overall medial pulvinar symmetry in 11 subjects. The asymmetry we found may relate to the fact that the medial pulvinar, more so than the lateral pulvinar, is connected with asymmetrical areas of the superior temporal and inferior parietal lobes
(4,
5). The abnormalities in schizophrenia were limited to the right side and abolished the normal pulvinar asymmetry, furthering the notion that lesser cerebral asymmetry is important in schizophrenia
(10,
18,
19) and adding to the lateralized findings in these brains
(10,
20). They are also in agreement with findings of an MRI study showing smaller volumes in the right posterior thalamus
(9). However, most other lateralized abnormalities in schizophrenia affect the left side of the brain, and we have no explanation for the right-sided involvement of the medial pulvinar.