Eating disorders pose a considerable threat to young adult women’s health and adjustment because they are associated with significant psychosocial impairment and adverse health outcomes, such as loss of bone mass, infertility, and high rates of suicide or death, resulting from complications of starvation
(1). To date in the United States, epidemiological studies of anorexia nervosa and bulimia nervosa have focused on white women and girls, and information about the prevalence of eating disorders in ethnic minority groups is unknown
(2). Several studies have examined rates of behavioral symptoms of eating disorders in ethnic minority populations in which black women have been studied the most. Results suggest that black women are less likely than white women to report dieting and vomiting but equally or more likely to report binge eating
(3). The lower rates of dieting and vomiting have been thought to reflect a lower risk for black women of developing anorexia nervosa or bulimia nervosa, disorders in which inappropriate methods of weight control represent core clinical features (DSM-IV). The similar
(4,
5) or slightly higher
(6) rates of binge eating in white and black women have been thought to reflect comparable risk for developing binge eating disorder, a disorder characterized by recurrent binge eating and the absence of inappropriate weight-control efforts. Most of these studies used self-report questionnaires, a method associated with high false positive identification of eating disorders symptoms, especially binge eating
(7–
9), or have relied on samples of convenience and provided incomplete information about participation rates, raising concerns about the generalizability of results.
The introduction of binge eating disorder into DSM-IV as a disorder in need of further study has prompted efforts to diversify eating disorders study populations because field studies, unexpectedly, reported comparable rates of binge eating disorder in white and black women
(10,
11). Moreover, subsequent studies found a strong association between binge eating disorder and obesity
(12). Given the high rates of obesity in ethnic minority populations, experts have hypothesized that binge eating disorder is a significant problem among these groups
(3). This study examined the prevalence of eating disorders, including binge eating disorder, in a geographically diverse community sample of young adult white and black women who had participated in a 10-year longitudinal study with an exceptional retention rate (89%) and who were assessed by using a state-of-the-art case-finding method.
Results
The sample included 2,046 women, representing 86.0% of the initial NHLBI Growth and Health Study cohort (California: 92.4%, N=820; Ohio: 77.5%, N=675; District of Columbia: 88.7%, N=551). Of the 1,166 white girls and 1,213 black girls enrolled in the first year of the NHLBI Growth and Health Study, 985 white women (84.5%) and 1,061 black women (87.5%) consented to participate in the present study. Most of the nonparticipants had been lost to follow-up before this study. Of the women included in NHLBI Growth and Health Study year 10, 98.3% (2,046 of 2,082) participated in the present study. By design, the NHLBI Growth and Health Study had enrolled two specific age cohorts, ages 9 and 10. For budgetary reasons, the present study collected data over 3 years, with participants’ ages ranging from 19 to 24 years. The average age was 21.3 years (SD=0.7) for the white women and 21.5 years (SD=0.7) for the black women.
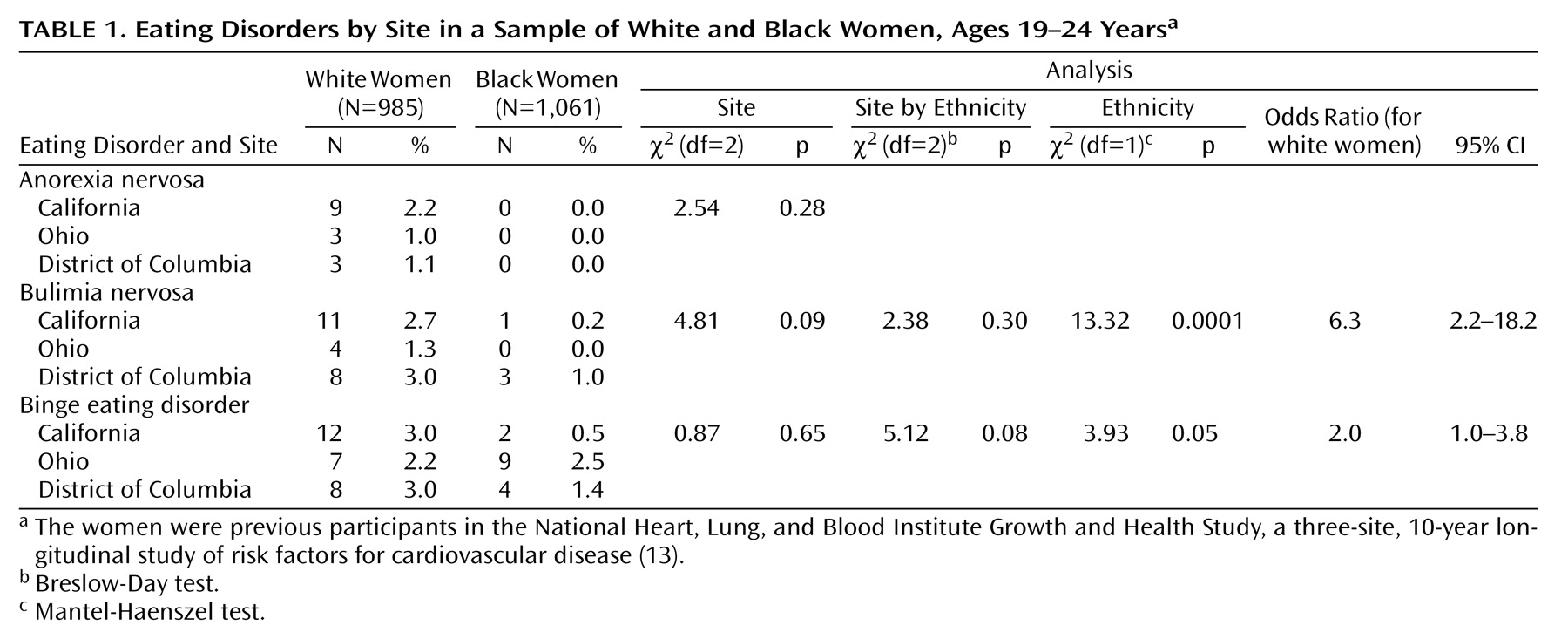
A total of 76 women (57 white, 19 black) met lifetime criteria for at least one eating disorder (
Table 1). Of the women with an eating disorder, 15 women (1.5%) met the criteria for anorexia nervosa (all were white), 27 (1.3%) for bulimia nervosa (23 white, 2.3%, four black, 0.4%), and 42 (2.1%) for binge eating disorder (27 white, 2.7%, 15 black, 1.4%). No participant met the criteria for all three disorders; six women met the criteria for anorexia nervosa and bulimia nervosa, and two met the criteria for bulimia nervosa and binge eating disorder (not concurrent).
As previously reported
(13), on average the black households had lower family incomes and lower educational levels than the white households. Nevertheless, in each ethnic group, wide ranges of income (less than $10,000 to $75,000 or more) and educational levels (less than a high school diploma to a graduate degree) were represented. White women with an eating disorder did not differ significantly from white women without an eating disorder on parental education (eating disorder: 8.8% had high school or less; 29.8% had some college; 61.4% had a college degree; no eating disorder: 19.1% had high school or less; 31.0% had some college; 49.9% had a college degree) (χ
2=4.52, df=2, p=0.11) or family income (eating disorder: 5.4% made less than $10,000; 7.1% made $10,000 to <$20,000; 32.1% made $20,000 to <$40,000; 55.4% made $40,000 or more; no eating disorder: 7.1% made less than $10,000; 9.0% made $10,000 to <$20,000; 31.5% made $20,000 to <$40,000; 52.3% made $40,000 or more) (χ
2=0.54, df=3, p=0.91).
Black women with an eating disorder did not differ significantly from black women without an eating disorder on parental education (eating disorder: 36.8% had high school or less; 47.4% had some college; 15.8% had a college degree; no eating disorder: 30.4% had high school or less; 47.5% had some college; 22.2% had a college degree) (χ2=0.60, df=2, p=0.74) or family income (eating disorder: 5.9% made less than $10,000; 41.2% made $10,000 to <$20,000; 29.4% made $20,000 to <$40,000; 23.5% made $40,000 or more; no eating disorder: 27.0% made less than $10,000; 19.7% made $10,000 to <$20,000; 29.7% made $20,000 to <$40,000; 23.6% made $40,000 or more) (χ2=6.67, df=3, p=0.08).
Black women (47.8%, N=507) were significantly more likely than white women (34.2%, N=337) to have ever been obese (χ2=38.82, df=1, p<0.0001, odds ratio=1.8, [confidence interval] CI=1.5–2.1). Black women (28.7%, N=304) were also significantly more likely than white women (12.0%, N=118) to be currently obese (χ2=86.73, df=1, p<0.0001, odds ratio=3.0, CI=2.3–3.7). We further examined the rates of current obesity among white and black women with and without a diagnosis of binge eating disorder. Results were nonsignificant (Mantel-Haenszel χ2=2.76, df=1, p=0.10), but they showed more women who met the criteria for binge eating disorder than those without being classified as currently obese.
The interaction term for ethnicity-by-eating-disorder status was not significant (Breslow-Day χ2=0.01, df=1, p=0.72). Specifically, more white women who ever had binge eating disorder were currently obese (22.2%, 6 of 27) than the white women without a history of binge eating disorder (11.6%, 111 of 958), but this difference only approached statistical significance (χ2=2.80, df=1, p=0.09). The rate of current obesity among black women with binge eating disorder (40%, 6 of 15) was not significantly elevated compared to obesity in black women without binge eating disorder (28.4%, 297 of 1,046) (χ2=0.97, df=1, p=0.32).
Analyses testing for ethnicity, site, and ethnicity-by-site interaction effects were conducted for bulimia nervosa and binge eating disorder; because all participants with anorexia nervosa were white (N=15, 1.5%) and it was self-evident that there was an ethnic difference in the rate of this disorder, only site effects were examined (the odds ratio estimated by assigning a value of 0.5 for black women with anorexia nervosa was 32.8). No significant site differences in the rate of anorexia nervosa were detected. White women (2.3%) were significantly more likely than black women (0.4%) to meet the lifetime criteria for bulimia nervosa (pooled odds ratio=6.3, CI=2.2–18.2); no site differences or site-by-ethnicity interaction effects were detected. White women (2.7%) were more likely than black women (1.4%) to meet the lifetime criteria for binge eating disorder (odds ratio=2.0, CI=1.0–3.8); no significant site or site-by-ethnicity effects were found.
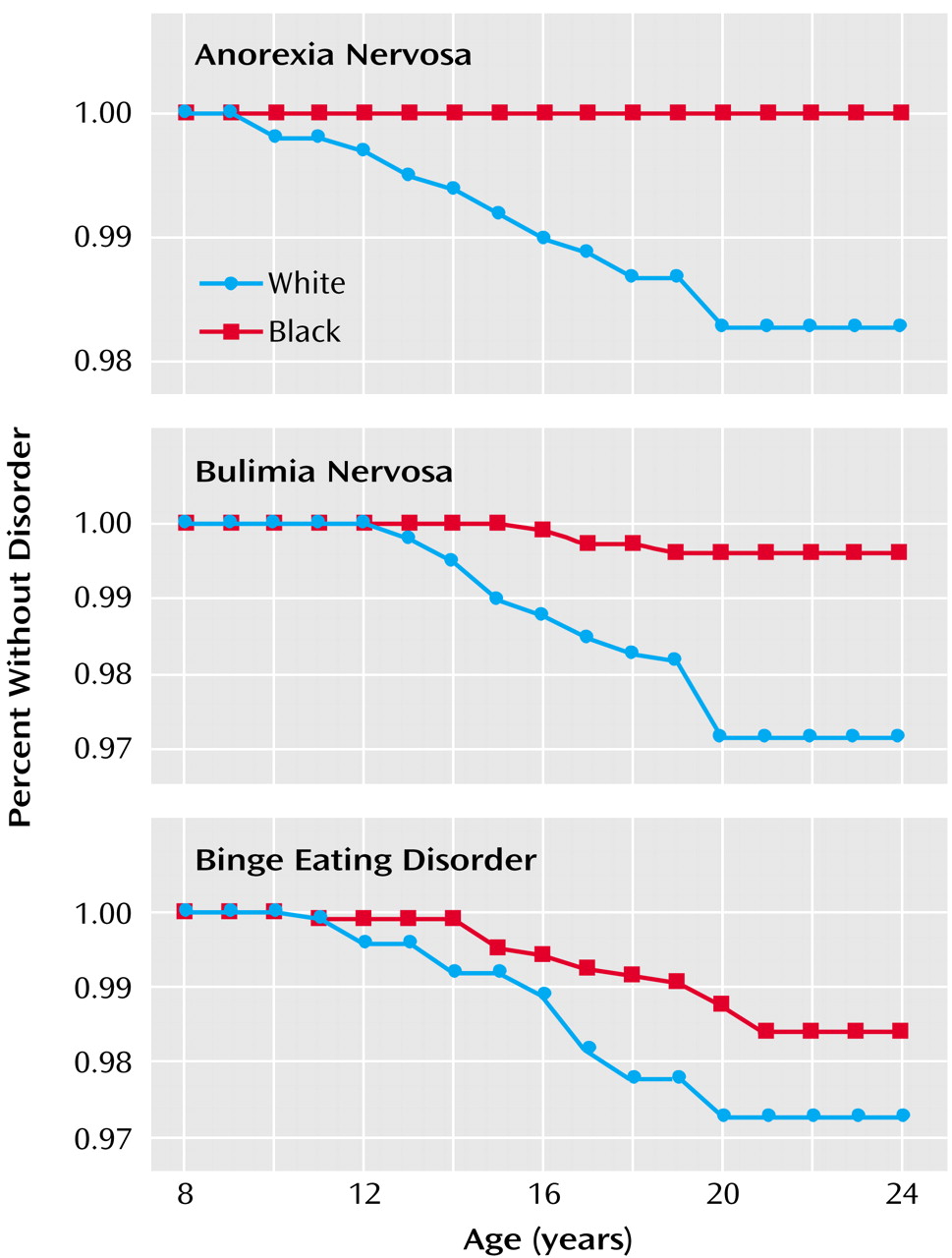
For descriptive purposes, separate survival curves were generated for the white and black women with bulimia nervosa and binge eating disorder and for the white women with anorexia nervosa, as shown in
Figure 1. For anorexia nervosa, the average age at onset was 15.4 years (SD=3.4); for bulimia nervosa, it was 16.6 years (SD=2.4) for white women and 17.3 (SD=1.3) for black women; for binge eating disorder, the average age of onset was 16.4 years (SD=2.7) in white women and 17.3 years (SD=2.9) in black women. Of the 76 women who ever had an eating disorder, 16 (28.1%) of the white women and one (5.3%) of the black women reported having received treatment for an eating disorder. When we excluded the 15 white women with anorexia nervosa, the eating disorder with the highest reported rates of treatment
(19), 11 (26.2%) of 42 white women reported that they had received treatment.
Discussion
Consistent with epidemiological studies in North America, Europe, and Australia
(2), our results suggest that all eating disorders are relatively uncommon and that anorexia nervosa is the least common, while binge eating disorder is the most common of the three eating disorders. The prevalence and ages of onset of anorexia nervosa and bulimia nervosa observed in our sample of white women were well within the ranges reported in other studies of white women in the United States and Canada
(20–
24). For example, the number of white women with anorexia nervosa and bulimia nervosa observed in this study (15 and 23 of about 1,000 women, respectively) was comparable to the lifetime prevalence rates (1.4% and 2.5%) in a community sample of similar ages recruited in Oregon
(22). Research has shown that late adolescence is the period of greatest risk for the onset of anorexia nervosa and bulimia nervosa and that onset after age 21 is rare
(20–
24). Nevertheless, in our sample of more than 1,000 black women (ages 19–24), no case of anorexia nervosa was detected, and the odds of detecting bulimia nervosa were six-fold greater for white women than for black women. We caution that our results need to be replicated by an independent research team before further conclusions can be drawn about differential risks for these eating disorders.
Previous studies of adult women have reported similar
(4) or even higher
(5,
6) rates of binge eating in black women than in white women. For example, the Coronary Artery Risk Development in Young Adults study
(4) reported that in a representative sample of women ages 18 to 30, 2.0% of white women and 2.2% of black women were identified by a questionnaire method as having binge eating disorder. In this study, significantly fewer black women (1.4%) than white women (2.7%) met the criteria for binge eating disorder, although the odds ratio of 2.0 suggested that this was only a small effect. Compared to anorexia nervosa and bulimia nervosa, the onset of binge eating disorder has been reported to occur later, with onsets observed later than the age of 21 years in a considerable subset of women
(25). Our sample was younger than those included in previous studies that examined ethnic differences in rates of binge eating or binge eating disorder. Future studies are needed to address the question of whether with increasing age black women “catch up” with white women in terms of actual rates of binge eating disorder.
Consistent with other studies, we found significant ethnic differences in lifetime and current rates of obesity. Although the rates of current obesity clearly were elevated among white and black women with binge eating disorder compared to women without binge eating disorder, these differences failed to reach statistical significance. Our sample was quite small for examining the association between a diagnosis of binge eating disorder and obesity that had been found in patient samples
(1) and in some
(4)—but not all—
(26) community-based studies of binge eating disorder. Moreover, our sample was relatively young, and the possible adverse effects of binge eating disorder on body weight may become more pronounced with increasing age
(27).
Few women reported a history of treatment for their eating disorders, and black women with eating disorders were particularly unlikely to have received treatment. Our results add to a growing literature that documents low treatment rates in general and marked ethnic differences in seeking and receiving treatment for an eating disorder
(28,
29). These differences do not appear to be a function of ethnic differences in the symptom severity of eating disorders
(25). The reasons for ethnic differences in mental health services use are complex
(30). Given that eating disorders are uncommon, it is plausible that health care providers are unfamiliar with eating disorders in ethnic minority groups and are therefore less likely to assess patients for the presence of an eating disorder. Several studies have shown that binge eating disorder is associated with obesity and psychiatric impairment
(10–
12), regardless of ethnicity
(25). Effective treatments have been developed
(31), and efforts are needed to increase the identification of and treatment rates for eating disorders.
Several limitations of this study need to be noted. Our study recruited participants who had been involved in a previous study that, by design, included only white and black girls. Consequently, the important question of prevalence of eating disorders in ethnic minority groups such as Asian American, Latina, or Native American women could not be addressed. Because of the small number of participants with eating disorders, we did not test whether the differences in ethnic groups observed in demographic variables contributed to the ethnic group differences in risk for an eating disorder. We noted that within ethnic groups, neither parental education nor family income was significantly associated with eating disorder status. The role of socioeconomic variables as possible risk factors for the development of an eating disorder is a matter of considerable debate
(32), and conclusive answers have been elusive because of the challenges involved in establishing community-based samples with adequate power.
Several strengths of the study also need to be acknowledged. We included a geographically and socioeconomically diverse sample of black and white women and achieved excellent participation over a long time period. Two major sources of potential bias regarding ethnic group differences in eating disorders can likely be ruled out. One, the uniformly high participation rate suggests that the present study did not favor differential detection of an eating disorder in either group. Two, diagnoses were based on operationalized criteria and measured with reliable interviews that were administered by highly trained staff.
Results of this epidemiological study suggest that, among young adults, black women are less likely than white women to have experienced an eating disorder. These differences were more pronounced for anorexia nervosa and bulimia nervosa than for binge eating disorder. Reported rates of treatment were low in both groups, but black women were particularly unlikely to have received treatment specifically for an eating disorder. Health professionals need to be alert to the possibility of eating disorders in adolescent girls, and research is needed to identify barriers to accessing treatment. Given the association of obesity and binge eating disorder, screening for binge eating disorder in white and black girls and women could lead to timely identification and prevention of the development of obesity.