Converging evidence from neuroimaging and histological studies implicates abnormalities in frontostriatal systems in adults with bipolar disorder
(1–
5). Few studies, however, have assessed these systems in adolescents with bipolar disorder. Preliminary magnetic resonance spectroscopic and morphometric data suggest the presence of frontal, striatal, and thalamic abnormalities in juvenile bipolar disorder
(6,
7). We report the first study, to our knowledge, to use functional magnetic resonance imaging (fMRI) to examine juvenile bipolar disorder. An event-related color-naming Stroop task, identical to that used in a study of adult bipolar disorder
(1), was employed to probe frontostriatal function and to permit investigation of potential similarities and differences in adolescents and adults with bipolar disorder.
Method
The study included 10 subjects aged 10–17 years with DSM-IV bipolar I disorder (including six female, one left-handed, and three unmedicated subjects) and 10 healthy comparison subjects aged 11–18 years with neither personal nor first-degree family history of axis I disorders (including six female subjects and one left-handed subject). None of the subjects had a neurological illness, history of head trauma, MRI abnormalities detected by a neuroradiological review performed by one of the authors (R.K.F.), medical illness (except one female bipolar disorder subject with treated hypothyroidism), history of substance or alcohol dependence, or substance or alcohol use within 24 hours of scanning. Diagnoses were established by the consensus of two examiners (A.M., J.K., or H.P.B.) on the basis of clinical interviews and administration of the revised Schedule for Affective Disorders and Schizophrenia for School-Age Children (Present and Lifetime versions)
(8). Structured interviews provided family history research diagnostic criteria. The Childhood Depression Rating Scale—Revised
(9) was administered immediately before scanning; the bipolar disorder patients’ mean score was 36.2 (SD=21.5, range=18–88).
Comorbid psychiatric diagnoses in bipolar disorder subjects included attention deficit hyperactivity disorder (ADHD) (N=2), oppositional defiant disorder (N=2), posttraumatic stress disorder (N=2), substance or alcohol abuse (N=2), obsessive-compulsive disorder (OCD) (N=1), generalized anxiety disorder (N=1), specific phobia (N=1), and learning disability not otherwise specified (N=1). Family history included at least one first-degree relative with bipolar disorder (N=3), major depressive disorder (N=3), or substance dependence (N=1) or a second-degree relative with bipolar disorder (N=1) or major depressive disorder (N=2). Medications included lithium (N=4), anticonvulsants (N=3), antidepressants (N=3), antipsychotics (N=2), stimulants (N=1), clonidine (N=1), and levothyroxine (N=1). After a complete description of the study, written informed consent was obtained from 18-year-old individuals and from guardians of individuals under age 18 years, who also provided written assent.
The Stroop activation paradigm, echoplanar imaging acquisition, and image processing were performed according to methods described previously
(1). Composite maps were used to compare the mean signal change (incongruent trials versus congruent trials) between the bipolar disorder and healthy groups at each pixel (significance threshold: p<0.005; cluster minimum: 20 adjacent pixels). Exploratory analyses investigated the effects of age and Childhood Depression Rating Scale—Revised scores on regional activation (correlation coefficient: r>0.70; cluster minimum: 20 adjacent pixels).
Results
The patient and comparison groups were similar in age (bipolar disorder group: mean=13.6 years, SD=2.8; comparison group: mean=14.6, SD=2.8; p=0.43); Stroop response accuracy, measured as the percentage of errors on incongruent stimuli (bipolar disorder group: mean=5.0, SD=11.3; comparison group: mean=16.7, SD=22.2; p=0.16); response times, measured by subtracting congruent response time from incongruent response time (bipolar disorder group: mean=203.7 msec, SD=43.5; comparison group: mean=202.6, SD=91.1; p=0.98); head displacement, measured by the maximum in x, y, or z planes across trials (bipolar disorder group: mean=1.1 mm, SD=0.5; comparison group: mean=0.9 mm, SD=0.4; p=0.31); and rotation (pitch, roll, or yaw) (bipolar disorder group: mean=1.2 degrees, SD=0.8; comparison group: mean=1.1 degrees, SD=0.6; p=0.85). All comparisons were made by means of t tests with unequal variance.
The healthy and bipolar disorder groups demonstrated distributed patterns of activation in regions previously reported to be associated with the Stroop task in adults, including the dorsal anterior cingulate; dorsolateral prefrontal, inferior prefrontal, and posterior association cortices; thalamus; and striatum
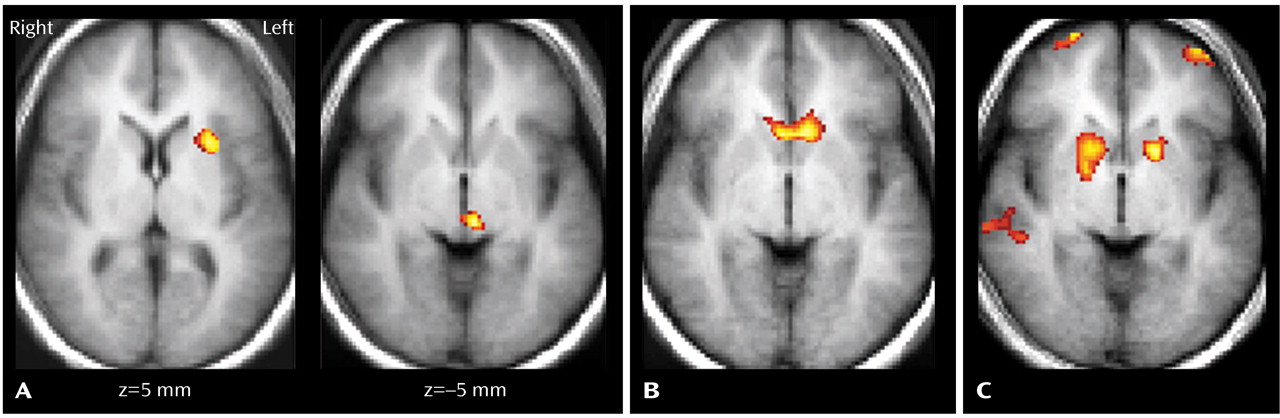
(1). The signal was increased in the bipolar disorder group, compared with the healthy group, in regions of the left putamen and inferior thalamus (
Figure 1). In the bipolar disorder group, Childhood Depression Rating Scale—Revised depression scores correlated positively with signal increases in the ventral striatum (
Figure 1). In both groups, age correlated positively with signal increases in the dorsal frontal and posterior association cortices, but only the healthy group demonstrated bilateral age-related increases in signal in the rostroventral prefrontal cortex and striatum (
Figure 1).
Discussion
During performance of an event-related fMRI color-naming Stroop task, increased signal was detected in the left putamen and thalamus of adolescents with bipolar disorder, compared with healthy adolescents. These regions are components of the frontostriatal circuits in which functional and anatomical disturbances have been implicated in the pathophysiology of bipolar disorder
(1–
7). Increased signal in the ventral striatum was associated with more severe depressive symptoms in the bipolar disorder group. Deficient activation in the rostroventral prefrontal cortex, which was reported previously for adults with bipolar disorder
(1,
2), was not detected in these adolescents with bipolar disorder. An association of age with increasing task-related signal changes was detected in this prefrontal region in the healthy comparison adolescents but not in the bipolar disorder group, suggesting that a progressive divergence in the activity of this region over adolescence may contribute to the larger group differences in its activity that were detected in adulthood.
Abnormalities in the striatum and thalamus have been reported in imaging studies of other disorders, such as ADHD, OCD, and Tourette’s disorder, in which the pathophysiologies are believed to involve disturbances in circuits subserving motivation and regulatory self-control
(10,
11). These conditions share some diagnostic features with bipolar disorder in children, which we speculate may be attributable to a common dysfunction in subcortical circuits. The adult bipolar disorder phenotype, moreover, may be difficult to recognize until late adolescence, when a progressive, age-related divergence in the maturation of prefrontal portions of the frontostriatal circuits
(12) produces a greater differentiation of executive functioning between these diagnostic groups.
These preliminary results are limited by the small number of subjects in this study. Alternative explanations for the absence of prefrontal abnormalities detected previously in studies of adults with bipolar disorder include the possibilities that the frontal abnormalities in adults are the consequence of repeated disease episodes, disease chronicity, or greater medication exposure. Patterns of functional abnormalities in adolescents and adults with bipolar disorder could also represent two distinct pathophysiological subtypes in bipolar disorder. Potential confounding factors in this study include medication influence on task performance or signal change, as well as the presence of comorbid disorders.
This study demonstrates the feasibility of investigating juvenile bipolar disorder by using fMRI methods. The findings suggest that the presence of frontostriatal abnormalities may be common to adolescents and adults with bipolar disorder. Future investigation of developmental disturbances in frontostriatal circuits may contribute to our understanding of the pathophysiology and progression of bipolar disorder across the lifespan.