Although the use of benzodiazepines has been declining, many individuals in the United States and other countries, particularly elderly patients, continue to use these agents
(6–
9). Simon et al.
(6) reported that in 1992, 2.8% of the members of a large U.S. health maintenance organization (HMO) used benzodiazepines during a 6-month period and benzodiazepine use increased with patient age. Other studies conducted between 1989 and 1997 in a variety of Western countries reported that 10%–17% of elderly community residents use benzodiazepines
(8–
10). Moreover, Tu and colleagues
(7) reported that benzodiazepine use, although declining, remained substantial among elderly Canadians: in 1993, 25.1% of elderly individuals in the Canadian province of Ontario used benzodiazepines, whereas in 1998, 22.5% used these medications. In many studies, a high proportion of benzodiazepine recipients used these medications for long-term treatment, defined as ≥60 days of use or as receiving benzodiazepines at each of several waves in a multiyear panel study
(6,
9).
Although benzodiazepine use is widespread, the benefits of prescribing these medications for depressed patients are unclear. Most randomized, controlled trials examining benzodiazepines as the primary pharmacological treatment for depression have concluded that these medications are less effective than antidepressants, as they address sleeplessness and restlessness but not the other core depressive symptoms
(13). Fewer studies have examined the effectiveness of combination treatment with both antidepressants and benzodiazepines, compared to antidepressant treatment alone. However, a recent meta-analysis completed by Furukawa and colleagues
(14) reported some benefits from combination treatment. They found that patients who received combination treatment dropped out of treatment less often than patients who received antidepressants alone. Patients who received combination treatment also experienced greater improvements in depressive symptoms at 1 and 4 weeks, although not after 6–8 weeks of treatment.
The literature includes conflicting reports about the risks arising from long-term benzodiazepine use
(15). Long-term users can develop withdrawal symptoms if benzodiazepines are tapered rapidly or discontinued abruptly
(15). Cognitive impairments indisputably occur with the acute administration of benzodiazepines; however, studies differ on the significance of cognitive impairments among long-term users. Some studies report continued cognitive difficulties with chronic use
(16), whereas others report only modest impairments among healthy long-term users
(17). Several observational studies have linked chronic benzodiazepine use with the subsequent development of dementia
(18), although one nested case-control study reported a decreased risk of Alzheimer’s disease among chronic benzodiazepine users
(19). Presumably because of the cognitive and psychomotor effects of benzodiazepines, many but not all studies have found benzodiazepines to be associated with increased rates of motor vehicle crashes, falls, and hip fractures among elderly patients
(20–
26).
However, little is known about the use of benzodiazepines among depressed patients treated in mental health settings and about how closely providers adhere to guideline recommendations. In this study, we examine the prevalence of benzodiazepine use among a large sample of depressed patients treated by U.S. Department of Veterans Affairs (VA) mental health providers. We examine the number of days’ supply of benzodiazepines that are dispensed to users, benzodiazepine dosing, and patient characteristics associated with benzodiazepine use.
Method
The study was conducted by using de-identified data from the VA National Registry for Depression, which is maintained by the VA Serious Mental Illness Treatment, Research, and Evaluation Center in Ann Arbor, Michigan. The registry includes data on demographic characteristics, inpatient and outpatient service use, medication use, health care costs, and mortality among veterans who received a depressive disorder diagnosis in VA mental health settings from 1997 through the present. The VA Ann Arbor Health System Institutional Review Board approved the study, with a waiver of informed consent for access to protected health information, given minimal risk to patients and the determination that the research could not be practicably conducted without a waiver.
Study Population
Patients were included in the study if they received any of the ICD-9-CM codes for depressive disorders (296.2x, 296.3x, 296.90, 296.99, 300.4, 311, 293.83, 301.12, 309.0, or 309.1) in a specialty mental health setting during the first 3 months (October 1 to December 31, 2000) of the study year, fiscal year 2001 (October 1, 2000, to September 30, 2001). Mental health settings were defined by using VA clinic and bed section codes. Patients who received a diagnosis of bipolar I disorder in addition to a depressive disorder diagnosis during the study year were excluded from the sample (N=12,581). The final sample included 128,029 veterans.
Study Measures
Patient demographics
Data on patients’ age and ethnicity (African American, Asian, American Indian, white, Hispanic, or unknown) were obtained from national VA databases. Patients were categorized into three age groups consisting of 1) patients age 44 years or younger, 2) patients age 45–64 years, and 3) patients age 65 years or older.
Benzodiazepine use
We considered patients to have used benzodiazepines as outpatients if they filled a prescription for any of the following medications on an outpatient basis: alprazolam, chlordiazepoxide, clonazepam, clorazepate, diazepam, estazolam, flurazepam, halazepam, lorazepam, oxazepam, prazepam, quazepam, temazepam, or triazolam. We noted whether benzodiazepines were prescribed on an “as needed” (p.r.n.) basis or as regular doses.
The number of days’ supply dispensed with each prescription fill is included in the VA pharmacy database and is based on the number of tablets/capsules dispensed and physicians’ directions for dosing. We calculated the total days’ supply of benzodiazepines that each patient received by adding the number of days’ supply dispensed with each benzodiazepine prescription fill during the year. The days’ supply for patients’ final fills were truncated at their date of death or at the end of study year.
Conservatively, we assumed that patients for whom benzodiazepines were prescribed on a p.r.n. basis took the maximum allowable dose—an assumption that resulted in the fewest calculated days’ supply. We also conservatively assumed that physicians had increased the dose of benzodiazepines rather than giving additional days’ supplies of medication when patients filled a second benzodiazepine prescription during an interval entirely covered by the days’ supply from a previous prescription. However, when new prescriptions overlapped but extended beyond the end date of a previous prescription, all of the additional days’ supply was added to the total days’ supply. Among individuals with overlapping prescriptions, the average overlap was 9 days.
We calculated both the mean prescribed benzodiazepine dose and the mean apparent benzodiazepine dose for all users. We also calculated the prescribed and apparent doses of benzodiazepines for three mutually exclusive subsets of users: 1) patients receiving only regular-dose benzodiazepine prescriptions, 2) patients receiving both regular-dose and p.r.n.-dose prescriptions, and 3) patients receiving only p.r.n.-dose prescriptions. Benzodiazepine doses were expressed in diazepam-equivalent milligrams by using conversion factors within the ranges suggested by several sources
(29–
31).
The mean prescribed benzodiazepine dose represents the dose prescribed/recommended by the physician, based on the physician’s dosing directions. The prescribed dose was calculated by adding all of the diazepam-equivalent milligrams dispensed during the year and dividing by the number of days that each prescription would “cover,” given the physician’s directions for dosing. Thus, a patient who filled two prescriptions—one for 30 10-mg tablets of diazepam, with directions to take one tablet per day (30-day supply at 10 mg/day) and a second prescription for 120 10-mg tablets of diazepam, with directions to take one tablet twice per day (a 60-day supply at 20 mg/day)—would have received a total of 1500 mg (300+1200 mg) prescribed to last 90 days (30+60 days) or a mean dose of 16.6 mg/day of diazepam equivalents.
Because patients taking benzodiazepines may have gaps between prescriptions, may not use their medications as prescribed, or may receive p.r.n. prescriptions that give them considerable autonomy in the amount and timing of their doses, we also calculated the mean apparent benzodiazepine dose for patients who filled more than one prescription for benzodiazepines (N=40,595). The mean apparent dose represents the dose that patients “apparently took,” given the total amount of benzodiazepines dispensed and the timing of their refills. The apparent dose was calculated by dividing the total milligrams of diazepam equivalents dispensed from the date of the first prescription fill for benzodiazepines until the date of the last fill divided by number of days between these fill dates. Thus, a patient who received 100 10-mg tablets of diazepam on January 1, 2001 (his first fill), another 100 5-mg tablets of diazepam on March 1, 2001 (his second fill), and a final fill on June 1, 2001, would have received a total of 1500 mg (1000+500 mg) over the course of the 151 days between January 1 and June 1, 2001, for a mean apparent dose of 9.9 mg/day.
For analyses examining whether patients increased their benzodiazepine dose during the year, patients’ first and last prescriptions of the year were converted into diazepam equivalents. Patients were then categorized into three groups: 1) those whose dose of diazepam equivalents decreased from the first to the last fill, 2) those whose dose remained stable, and 3) those whose dose increased.
We considered patients to have received antidepressants if they filled an outpatient prescription for a medication in the following VA national formulary drug classes: CN 601, 602, or 609 (antidepressants).
We used a modified version of the Charlson Comorbidity Index
(32) as a measure of medical comorbidity. The presence or absence of each of 19 medical conditions in administrative data during fiscal year 2001 was noted. Dummy variables were constructed for three categories of scores: 1) a Charlson score of 0 (indicating that the patient did not have any of these medical conditions), 2) a Charlson score of 1 or 2, and 3) a Charlson score of 3 or more.
For analyses of service utilization, we used a measure of psychiatric comorbidity as a covariate and categorized patients with depression into three groups: 1) those with depression alone, 2) those with a diagnosis of one of six specified psychiatric comorbidities (posttraumatic stress disorder [PTSD], other anxiety disorders, substance use disorder, dementia, schizophrenia, or bipolar II disorder), or 3) those with two or more of these specified comorbidities.
For analyses examining geographic variation in benzodiazepine use, we assigned VA medical centers to regions of the country (Eastern, Central, Southern, or Western) on the basis of a VA Health Services Research and Development Service regional map
(33).
Data Analysis
Patient characteristics and medication use were described with means (and standard deviations) and frequencies. T tests and chi-square analyses were used to compare the characteristics of benzodiazepine users and nonusers. Prescribed benzodiazepine doses were compared to apparent doses by using paired t tests. The significance of differences in benzodiazepine use by VA facility and by region of the country was determined by using chi-square analyses.
Multivariate logistic regression analyses were used to examine the relationship between the dependent variable, benzodiazepine use (yes/no), and independent patient-level variables entered simultaneously, including age group, sex, race, Charlson score category, presence of a concurrent PTSD diagnosis (yes/no), presence of concurrent anxiety disorder other than PTSD (yes/no), and presence of a concurrent substance use disorder (yes/no). Multivariate linear regression analysis was used to examine the relationship between prescribed benzodiazepine dose and the predictors listed previously.
We used multivariate logistic regression analysis to examine the relationship between the dependent variable, hospitalization in fiscal year 2001 (yes/no), and the independent variable, benzodiazepine use (yes/no), with adjustment for other factors likely to affect hospitalization, including age group, race, gender, and medical and psychiatric comorbidity. In a second model, an interaction term for benzodiazepine use and age group was included. We also used multivariate linear regression analyses to examine the relationship between the number of outpatient visits and benzodiazepine use, with adjustment for age group, race, gender, and medical and psychiatric comorbidity.
Results
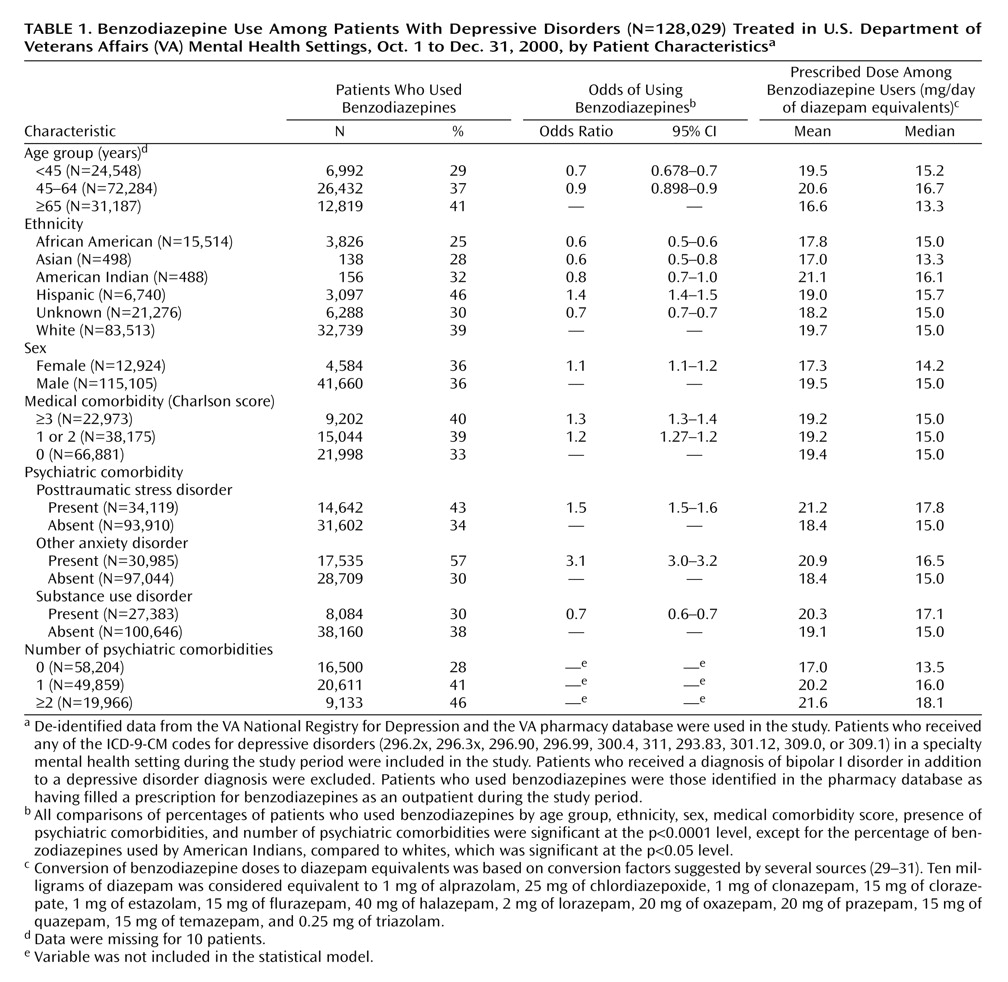
Table 1 shows data on the patients’ demographic characteristics and benzodiazepine use.
Patient Characteristics
In keeping with the VA population, 90% of the depressed veterans were male. Their mean age was 56 years (SD=13), and 24% were age 65 years or older. Most depressed patients had a comorbid psychiatric diagnosis; 27% had PTSD, 24% had an anxiety disorder other than PTSD, and 21% had a substance use disorder. Approximately 16% had two or more of these three comorbidities.
Benzodiazepine Use
A total of 46,244 (36%) of the depressed veterans and 12,819 (41%) of the elderly depressed veterans received a benzodiazepine prescription during the year. Almost all veterans who received a benzodiazepine prescription were also taking antidepressants; 89% of the overall sample and 94% of benzodiazepine users received antidepressants.
Most (60%) benzodiazepine users had a prescription for only regular doses of benzodiazepines; however, both p.r.n. and regular doses were prescribed for 21%, and only p.r.n. doses were prescribed for 20%. Clonazepam was the most frequently prescribed benzodiazepine, followed by lorazepam and diazepam.
Benzodiazepine users usually received supplies that would allow long-term use; 78% of all depressed users and 82% of elderly users received ≥90 days’ supply of benzodiazepines. Sixty-one percent of all users and 65% of elderly users received ≥180 days’ supply. Dispensing of less than a 30-day supply of benzodiazepines, a practice typically recommended by practice guidelines, occurred for only 6% of users. Patients who received only p.r.n. benzodiazepines were less likely to receive ≥90 days’ supply than were other users (62% versus 81%).
Among benzodiazepines users, the mean prescribed dose of benzodiazepines was 19.3 mg/day of diazepam equivalents and the median prescribed dose was 15.0 mg/day of diazepam equivalents. Patients’ apparent doses were lower than their prescribed doses; the mean and median apparent doses were 15.4 mg/day and 11 mg/day, respectively. The subset of patients who had only p.r.n. doses had both smaller prescribed doses (mean=16.0 mg/day) and smaller apparent doses (mean=10.8 mg/day).
Among users with two or more refills, 21% had an increase in their dose of diazepam equivalents during the year, 63% continued to take a stable dose, and 16% had a decrease in their dose.
Benzodiazepine use varied significantly by region of the country. Patients who received treatment in VA facilities located in the Southern region were more likely to receive benzodiazepines than those in the Eastern, Central, and Western regions. Benzodiazepine use also varied significantly at the facility level. In the facility with median benzodiazepine use, 35% of depressed patients received benzodiazepines. However, in the facility with the least benzodiazepine use, only 11% of depressed patients received benzodiazepines, compared to 67% of depressed patients in the facility with the greatest benzodiazepine use.
Characteristics of Depressed Benzodiazepine Users
Table 1 reports the prevalence of benzodiazepine use among depressed patients and the mean and median prescribed doses among users by age group, race, sex, medical comorbidity, and psychiatric comorbidity.
Table 1 also summarizes the results of a multivariate logistic analysis of the relationship between benzodiazepine use and patient characteristics and gives odds ratios for use by pertinent subgroups.
As
Table 1 shows, several patient-level characteristics were associated with benzodiazepine use. Older patients were more likely than younger patients to use benzodiazepines: 41% of depressed patients age 65 years or older received benzodiazepines, compared to 37% of patients age 45–64 years and 29% of patients age 44 years or younger. However, older users received lower benzodiazepine doses than younger users. African Americans were much less likely and Hispanics more likely to receive benzodiazepines than whites, and African American users received lower doses of benzodiazepines than white users.
Depressed patients with a concurrent diagnosis of PTSD or other anxiety disorder were more likely to receive benzodiazepines than were patients without these comorbidities. Fifty-seven percent of patients with comorbid anxiety received benzodiazepines, compared to 30% without a comorbid anxiety diagnosis. Patients with concurrent substance use disorders were less likely to receive benzodiazepines than were patients without substance use disorders. Among benzodiazepine users, patients with comorbidities received somewhat higher doses than those without comorbidities.
Medical Services Use
In multivariate analyses examining the relationship of the main effects of benzodiazepine use and hospitalization during fiscal year 2001, benzodiazepine users had both a moderately higher risk for medical hospitalization (odds ratio=1.36; 95% confidence interval [CI]=1.31–1.41) and a slightly higher risk for psychiatric hospitalization (odds ratio=1.14; 95% CI=1.09–1.19), compared to nonusers. In a second model that added an interaction term for benzodiazepine use and age group, benzodiazepine use was associated with a higher risk for psychiatric and medical hospitalization among younger than among older patients.
In multivariate analyses, benzodiazepine users and nonusers did not differ significantly in overall numbers of outpatient visits. However, depressed benzodiazepine users had more outpatient medical visits than depressed nonusers (a mean of 26 visits compared to 21 visits, p<0.0001 [t test]).
Discussion
This study, which examined the use of benzodiazepines among depressed patients treated in specialty mental health settings, expands on previous reports of high levels of benzodiazepine use in the community and in primary care. Slightly more than a third of depressed patients treated in specialty mental health settings in the VA health care system received benzodiazepines, and the majority of users received ≥180 days’ supply. Benzodiazepines were almost always given in combination with, rather than instead of, antidepressants. This pattern of use is inconsistent with guideline recommendations.
It is unclear why so many depressed patients seen in specialty mental health settings receive supplies of benzodiazepines that would allow long-term use. However, we suspect that providers prescribe long-term treatment with benzodiazepines for a number of reasons.
First, it is likely that many patients find benzodiazepines helpful and request these medications from their physicians. In qualitative studies, general medical physicians reported that they prescribe long-term benzodiazepines because they are continuing prescriptions initiated by other physicians or are responding to patients’ requests and avoiding disruptions in the relationship with the patient
(34,
35). Physicians may also begin treatment with benzodiazepines for early symptom relief and then fail to reassess the patient’s need for the medication or may feel reluctant to discontinue the medication if the patient is doing better. Alternatively, physicians may simply find that their depressed patients stay in treatment longer when given combination antidepressant and benzodiazepine treatment and that the symptoms of patients who receive combination treatment respond sooner than those of patients treated with antidepressants alone.
Premature discontinuation of antidepressant treatment is a major problem in the care of depressed patients, with repports indicating that 30%–70% of depressed patients end their antidepressant treatment early
(36,
37). A recent meta-analysis found that patients given combination treatment were more likely to continue in care, compared to patients given antidepressants alone, and that patients who received combination treatment experienced greater improvements in symptoms at 1 and 4 weeks, although not at 6–8 weeks
(14). Several studies have suggested that clonazepam may augment antidepressants’ effectiveness in the short term, although again, this benefit is less clear over the long term
(38,
39). Data from laboratory studies have also indicated that benzodiazepines affect γ-aminobutyric acid pathways that might be important in the genesis and maintenance of depressive disorders
(40).
We found that physicians generally prescribed a moderate dose of benzodiazepines for their depressed patients (mean=19.3 mg/day of diazepam equivalents; median=15.0 mg/day). The patients’ mean apparent benzodiazepine dose was even lower, suggesting that patients receiving refills may have taken lower doses than prescribed or may have used benzodiazepines intermittently.
In our study, prescriptions for benzodiazepines were associated with several patient-level factors. As in community studies, we found that benzodiazepines were prescribed more frequently for depressed white and Hispanic patients than for African American patients. Reasons for these differences are unclear, given that benzodiazepines do not appear to be less effective or more problematic in the treatment of African Americans, compared to other ethnic groups
(41,
42). One potential explanation might be that physicians were responding to different symptom presentations, with depressed African Americans presenting with less anxiety. However, multivariate analyses that adjusted for concurrent anxiety disorders also demonstrated this difference in treatment of African Americans.
As in previous studies
(6,
11), we found benzodiazepine use to be more common among older patients than among younger patients. This repeated finding is surprising, given that physicians must balance the risks and benefits of prescribing benzodiazepines, and the risks appear to increase with the patient’s age. It is possible that a higher percentage of older patients, compared to younger patients, have had exposure to benzodiazepines and that older patients are thus more likely to request these medications. Older patients may also perceive greater benefit from benzodiazepine use or have more difficulty in discontinuing these medications once they have been started
(43). It is reassuring that although benzodiazepine use is more common among older patients, they receive lower doses.
Benzodiazepine use also varied with patients’ clinical characteristics. As reported in previous studies, providers were more likely to prescribe benzodiazepines to patients with higher levels of medical comorbidity, perhaps because these patients are seen more frequently or have higher levels of distress. Providers were also more likely to prescribe benzodiazepines for patients with concurrent anxiety disorders, who might experience more symptom relief from these medications, and less likely to prescribe these medications for patients with concurrent substance use disorders, who might experience more problematic use. Nevertheless, in this sample, a substantial percentage (30%) of depressed patients with comorbid substance use disorders received benzodiazepines as outpatients, a finding that raises concern.
We note that the use of adjunctive benzodiazepines varied considerably by geographic region and by VA facility, suggesting that local practice patterns in addition to patient factors were important in determining the prevalence of combination treatment.
Although we found a modest association between benzodiazepine use and increased rates of hospitalization adjusted for age, it is surprising that we also found that benzodiazepine use was associated with a greater increase in hospitalization among younger users, compared to older users. However, with a cross-sectional study design, it is not possible to completely disaggregate the potential interrelationships between benzodiazepine use, illness severity, and hospitalization. Thus, these associations should be interpreted with caution. Longitudinal and case-control studies that examine the relationship between benzodiazepines and health outcomes, such as cognitive impairment, falls, and hip fractures, have usually, but not always, reported poorer outcomes among long-term benzodiazepine users
(18,
22–25).
Limitations
This study had several limitations that must be considered in interpreting the results. First, the study sample was composed of all patients receiving treatment for depression during the first 3 months of fiscal year 2001. The patients with benzodiazepine use in this sample (prevalent cases) may have preferentially included patients with chronic depressive illnesses, including those who remained in treatment because they were given benzodiazepines. In a sample composed of patients who were newly receiving depression treatment (incident cases), a smaller percentage of patients might receive benzodiazepines.
Second, although all patients in the study received treatment for depression in mental health settings, we were unable to identify the specialty of providers who prescribed the benzodiazepines. General medical rather than mental health providers may have been responsible for some of these prescriptions. However, depressed benzodiazepine users had an average of 16 outpatient mental health visits, suggesting that even if mental health providers did not prescribe all of the benzodiazepines, they also did not greatly limit the use of these medications.
Third, the diazepam-equivalent doses we present must be considered approximate, given the range of diazepam dose equivalents suggested in the literature. Fourth, as noted earlier, the cross-sectional nature of this study limits the conclusions we can draw about the causality of the associations between benzodiazepine use and hospitalization. And finally, although we note frequent long-term use of benzodiazepines, we do not know that such use was inappropriate. The patients in this sample may have had indications for long-term use and may have experienced continued benefit from these medications. The patients’ mean dose of diazepam equivalents was not extremely high, and the doses were relatively stable.
Nevertheless, given the numerous studies demonstrating adverse medical outcomes among long-term users of benzodiazepines, the high prevalence of benzodiazepine use in this sample remains a concern. Further research is needed on both the risks and benefits of this widespread practice.
Summary
Despite guideline cautions, long-term co-prescription of antidepressants and benzodiazepines remains a common treatment pattern in specialty care. Elderly patients are more likely to receive benzodiazepines than younger patients, although elderly patients receive lower doses than younger patients. Further research is needed to clarify clinicians’ reasons for long-term treatment with benzodiazepines and the effectiveness of this practice.