The most frequently reported psychiatric consequences of sexual abuse in women are posttraumatic stress disorder (PTSD), mood disorders, substance abuse, and eating and sexual disorders
(1–
3). A number of confounding factors, however, render difficult the interpretation of results.
Some studies combined various forms of sexual violence, including harassment, subtle or indirect abuse according to the subjective perception of the victim versus the perpetrator, and others
(4). The occurrence of sexual abuse is generally evaluated on the basis of subjective recall on the part of the victims, where it is well known that both denial and minimization on one hand and exaggeration and even mythomanic reconstruction on the other may occur
(5). Early sexual traumata during childhood/adolescence and abuse during adulthood are sometimes combined when analyzing the results
(6).
Finally, it is still unclear whether there is specificity in the psychic reaction to violent sexual traumata or whether it parallels the response to other forms of nonsexual events.
The present study assesses the psychopathological consequences of a single rape in adult women who did not experience any form of sexual abuse during childhood or adolescence and where the occurrence of rape was established with certainty by police investigation. A control group was composed of women who underwent a severe, almost life-threatening event devoid of any sexual content, such as a car accident, a violent robbery, or a physical assault.
Method
Forty young women who were the victims of rape as decided by a court of law were studied. These women were recruited from those who were consecutively referred to a women’s association devoted to the assistance of abused women and who were raped within a period of 4 to 9 months before the interview. None of them reported any form of sexual abuse during childhood or adolescence. The definition of rape for inclusion in the study was “forced sexual penetration upon the subjects without their consent.” Thirty-four women (85%) were raped by a single man, while in six cases (15%), the aggressors were two or more men. The aggressors were known to the victims only in four cases (10%). At the time of the rape, the mean age was 34.5 years (SD=7.4). By marital status, 22 (55%) were married, eight (20%) were separated or divorced, and 10 (25%) were unmarried.
After a complete description of the study to the subjects, we received no refusal to participate, and written informed consent was obtained. All of the subjects were evaluated by a qualified female psychiatrist (A.G.) by means of the Florence Psychiatric Interview
(7). This is a semistructured clinical interview that is made up of a combination of known rating scales and includes almost all of the symptoms considered by DSM-IV. The Florence Psychiatric Interview is an instrument able to produce DSM-IV diagnoses perfectly superimposable upon those of the Structured Clinical Interview for DSM-IV. Interrater agreement, test-retest reliability, recall bias, construct validity, and agreement with several other instruments have all been extensively evaluated in the validation studies. In particular, the Florence Psychiatric Interview explores 121 symptoms. Because the symptoms were scored 0 to 4 (absent, dubious, mild, moderate, or severe), a symptom was considered to be present when the score was at least 2
(7).
The raped women were compared with 32 women in the general population who had experienced a life-threatening trauma (except any form of sexual abuse). These subjects were recruited by reviewing the records of a community study conducted in Sesto Fiorentino and were selected to match the raped women for age, educational level, and marital status. The mean age was 33.7 years (SD=7.7); 17 (53%) were married, seven (22%) were separated or divorced, and eight (25%) were unmarried. Four of them (13%) had experienced a car accident with risk for the life, 18 (56%) had experienced a physical assault, and 10 (31%) were violently robbed during the previous 9 months. None of these women underwent any form of sexual abuse during childhood or adolescence. These control women were also administered the Florence Psychiatric Interview.
Results
Compared with the nonraped group, the following psychiatric diagnoses were found with significantly greater prevalence among the raped women: PTSD (N=38, 95%, versus N=15, 47%) (χ2=21.2, df=1, p=0.000005), sexual disorder (N=36, 90%, versus N=6, 19%) (χ2=33.2, df=1, p=0.000001), major depression (N=30, 75%, versus N=14, 44%) (χ2=5.8, df=1, p<0.02), eating disorder (N=21, 53%, versus N=2, 6%) (χ2=16.2, df=1, p<0.00006). Anxiety disorders (excluding PTSD) were also more prevalent in the raped group, although they were at the limit of significance (N=15, 38%, versus N=5, 16%) (χ2=3.7, df=1, p=0.054).
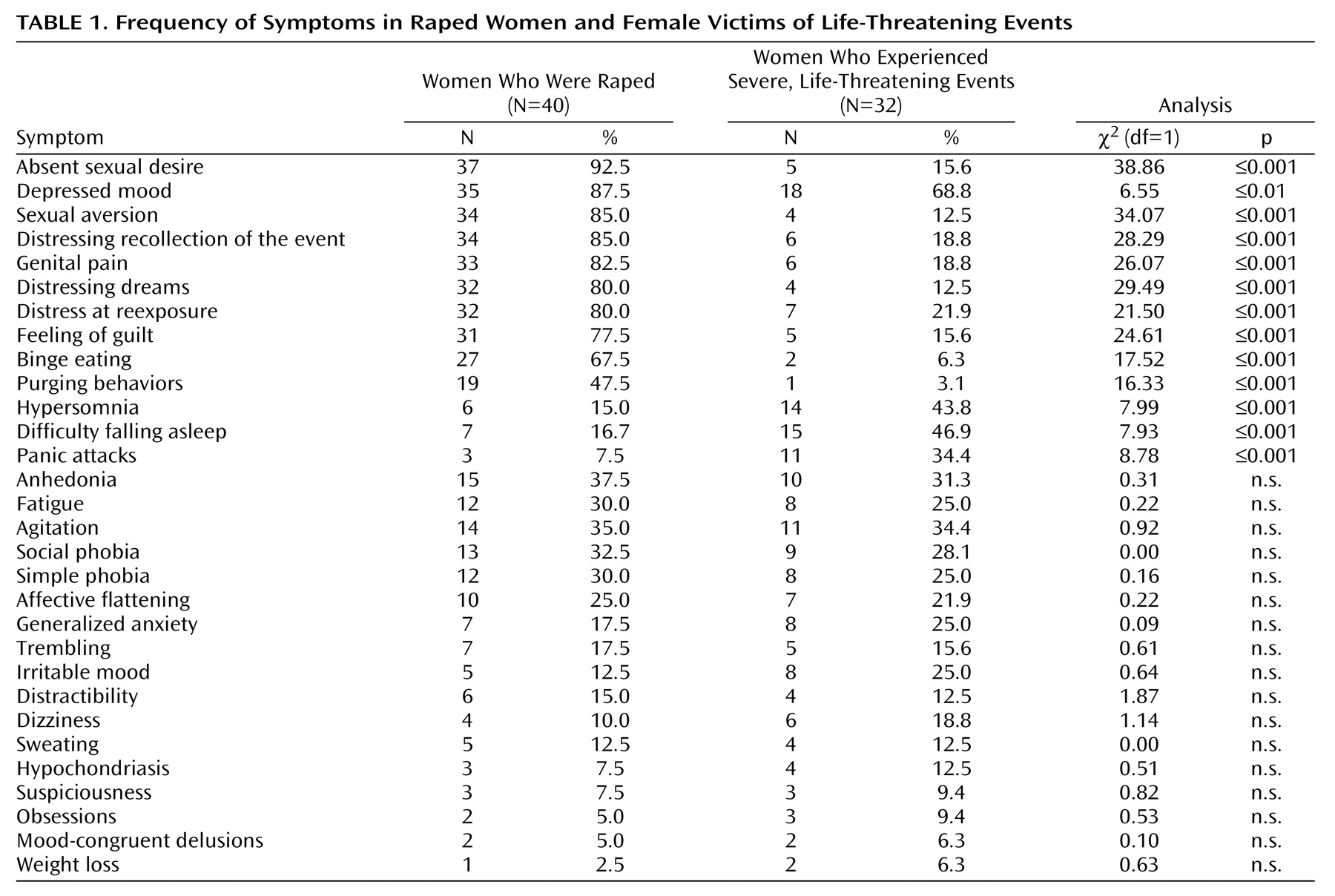
As far as the single symptoms were concerned, significant differences between the two groups are summarized in
Table 1, which shows the frequency of the 30 symptoms reported by at least three subjects.
Discussion
This group cannot be assumed as representative of all adult women who were raped for the first time but only for the subjects who were instituting legal proceedings against the rape perpetrator and chose to contact an association devoted to the assistance of abused women. We could presume that raped subjects referring to an association devoted to the psychological and legal assistance of abused women could be more prepared to describe their symptoms. Furthermore, interviewing raped women is difficult because of their negative attitudes toward a detailed psycho(patho)logical investigation after such an experience. Although we did not receive any refusal to participate from the raped women, it is still possible that some symptoms or psychopathological areas were not fully answered by the interviewees.
The significant differences between raped and nonraped women seem to indicate that the psychopathological consequence of rape could be rather specific. In particular, most of the raped women show a more significant impairment in the areas of painful reexperience of the traumatic event, sexual disorders, and eating disorders. This could warrant particular attention and interest. The control group was made up of women who had undergone different kinds of life-threatening traumata. These events may have different meanings (physical contact with an aggressor, or impersonal trauma in the case of a car accident) and could produce different reactions. The differences between the raped subjects and the control subjects could be due to the interpersonal contact rather than to their sexual nature. However, when we compared the symptoms of those who had experienced a car accident with those who had undergone a physical attack or a robbery, no difference or tendency for a difference emerged. It would seem, therefore, that the main difference actually was in the sexual nature of the event.
No other study, to our knowledge, has dealt with women raped in adulthood who were not sexually abused in childhood or adolescence and whose rape had been ascertained with reasonable security in a forensic trial. An adequate comparison with other studies is therefore impossible.