Childhood conduct disorder is a top mental health priority
(1). Evidence from prospective longitudinal data shows that childhood conduct disorder precedes a variety of major axis I psychiatric disorders
(2), suggesting that treating conduct disorder might significantly reduce the burden of adult mental disorder. Preschool intervention is desirable to prevent chronic conduct disorder
(3). To intervene early, valid methods must be available to diagnose conduct disorder in young children, and in this
Journal, Keenan and Wakschlag
(4) called for studies of the validity of conduct disorder diagnoses in children under age 6. This article responds, reporting the validity of applying the DSM-IV conduct disorder diagnosis to a representative, nonreferred sample of over 2,000 4½–5-year-old boys and girls.
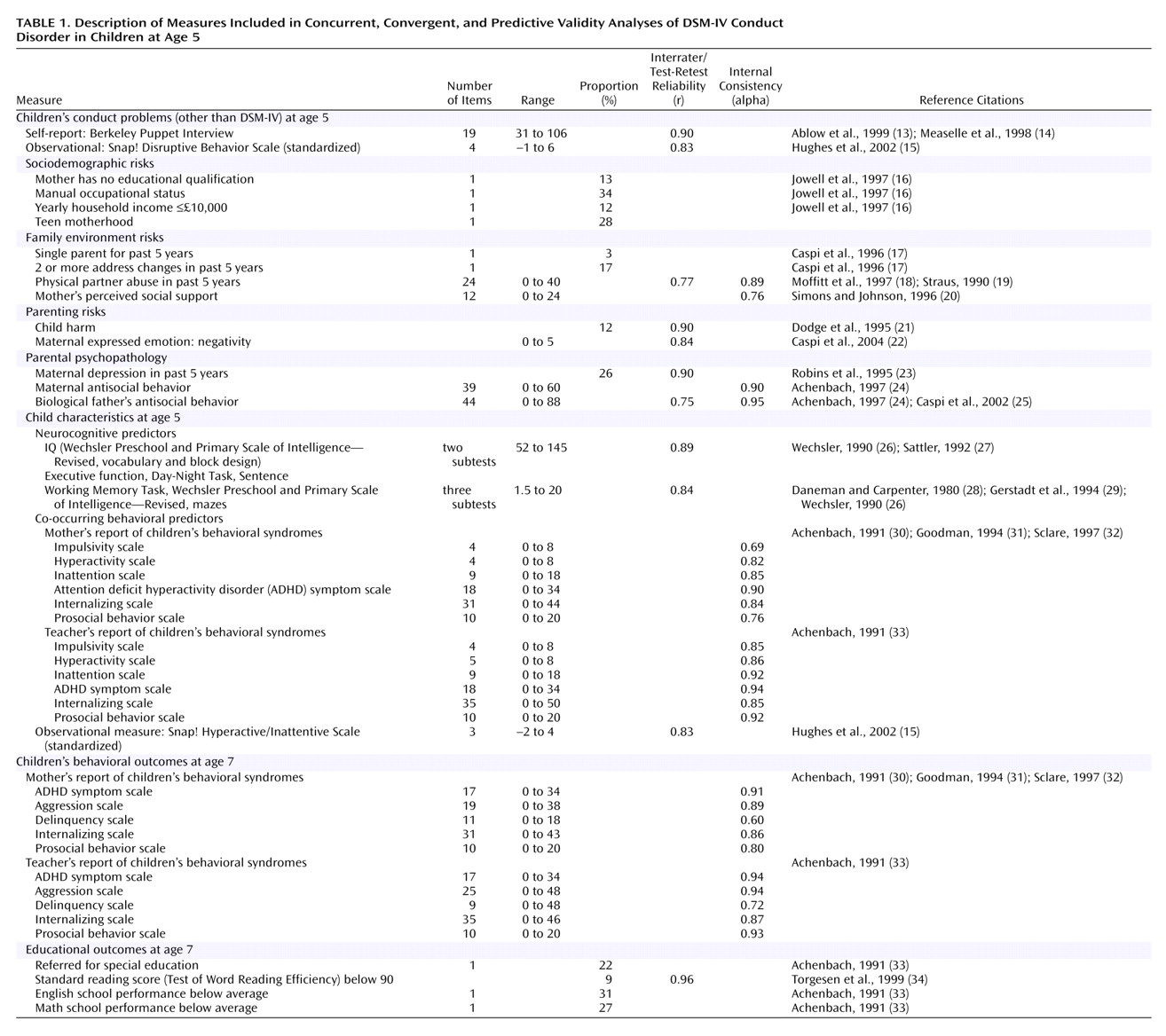
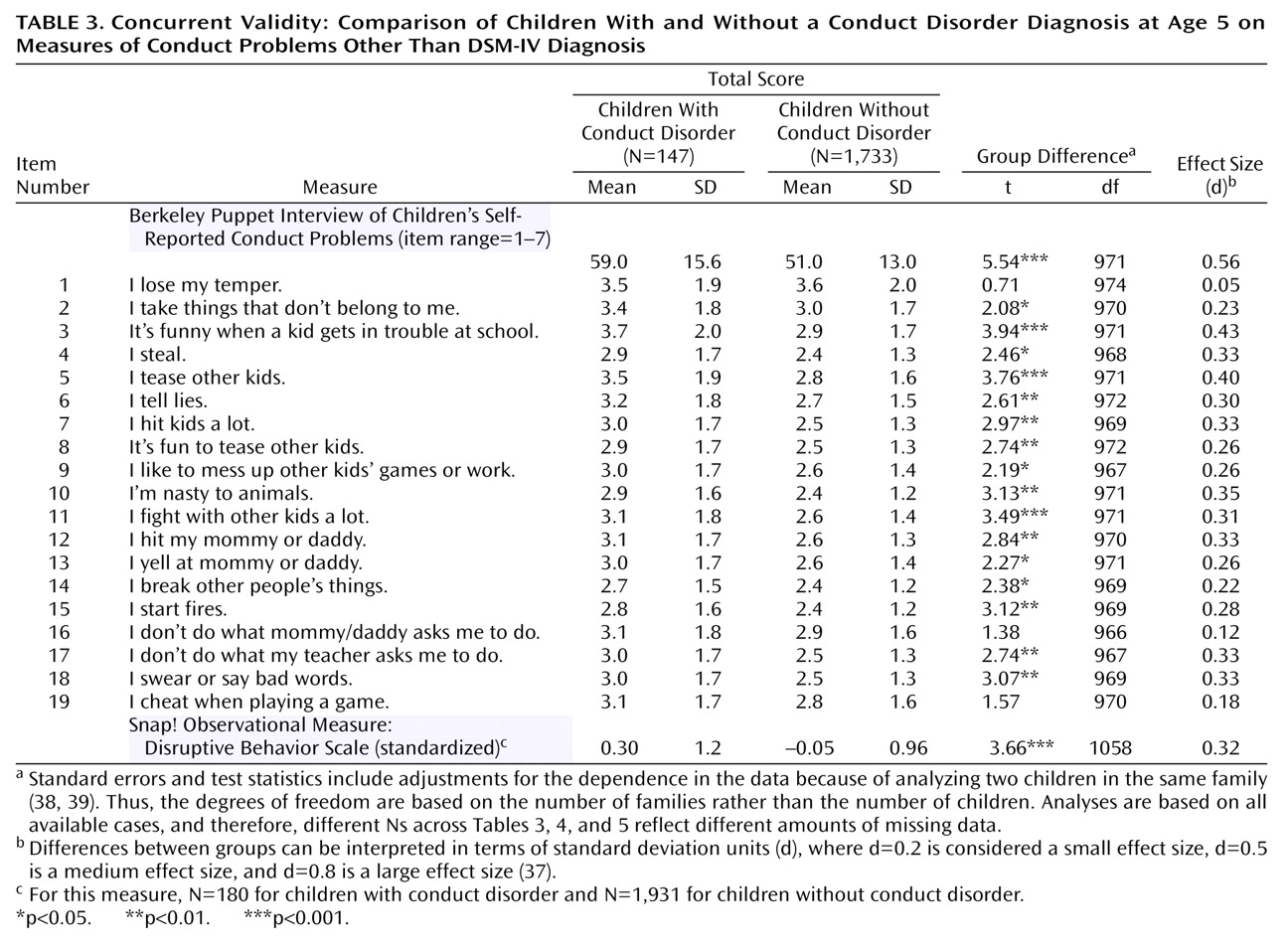
The validity of the DSM-based conduct disorder diagnosis in very young children can be ascertained by testing its concurrent, convergent, and predictive validity
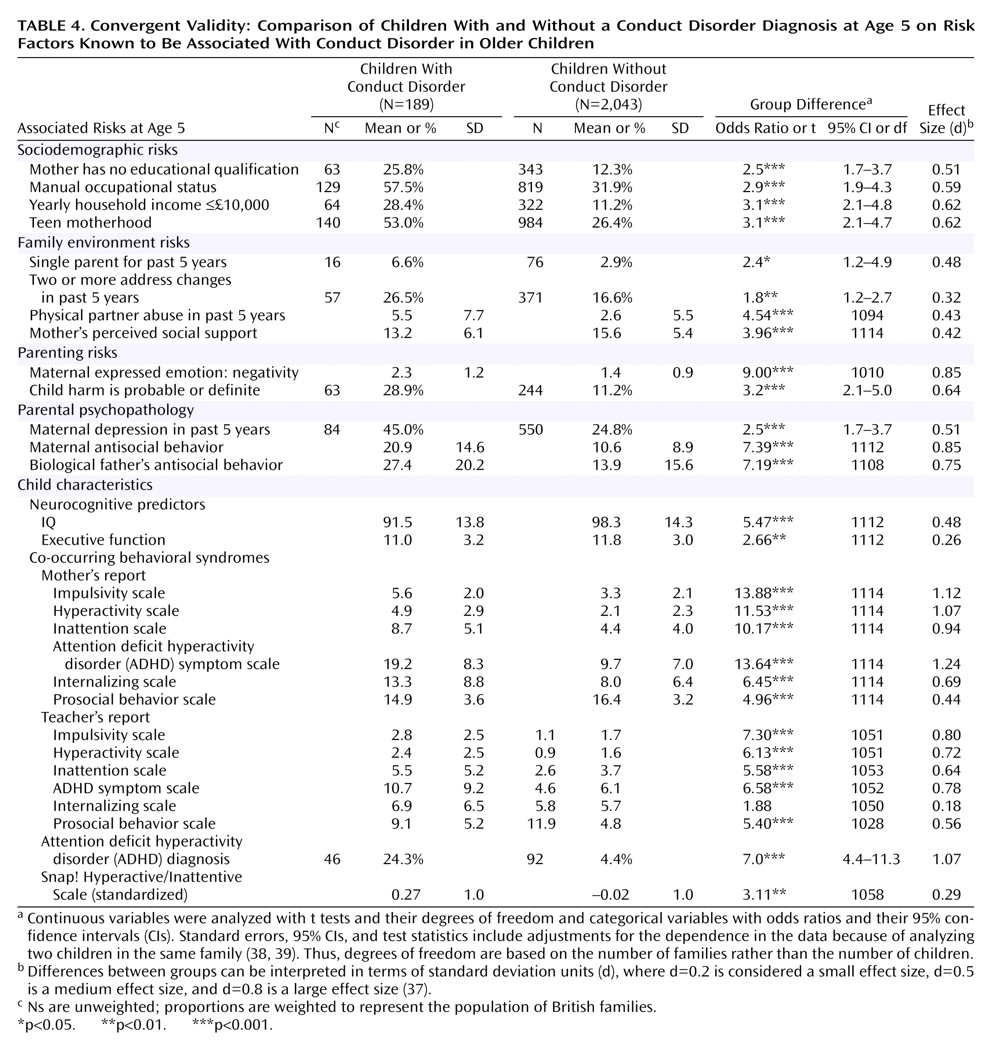
(5). In the present study, the diagnosis of conduct disorder would have concurrent validity if children with and without a conduct disorder diagnosis differed on other, independent measures of conduct problems. The diagnosis would have convergent validity if children with and without a conduct disorder diagnosis differed on measures of risk factors that are known to correlate with conduct disorder in older children. Risk factors associated with conduct disorder in older children include male sex, sociodemographic characteristics (e.g., low income, teen motherhood), quality of family environment (e.g., domestic violence, low social support), parenting (e.g., child harm), parental psychopathology, and co-occurring behavioral and neurocognitive child characteristics (e.g., hyperactivity, low IQ)
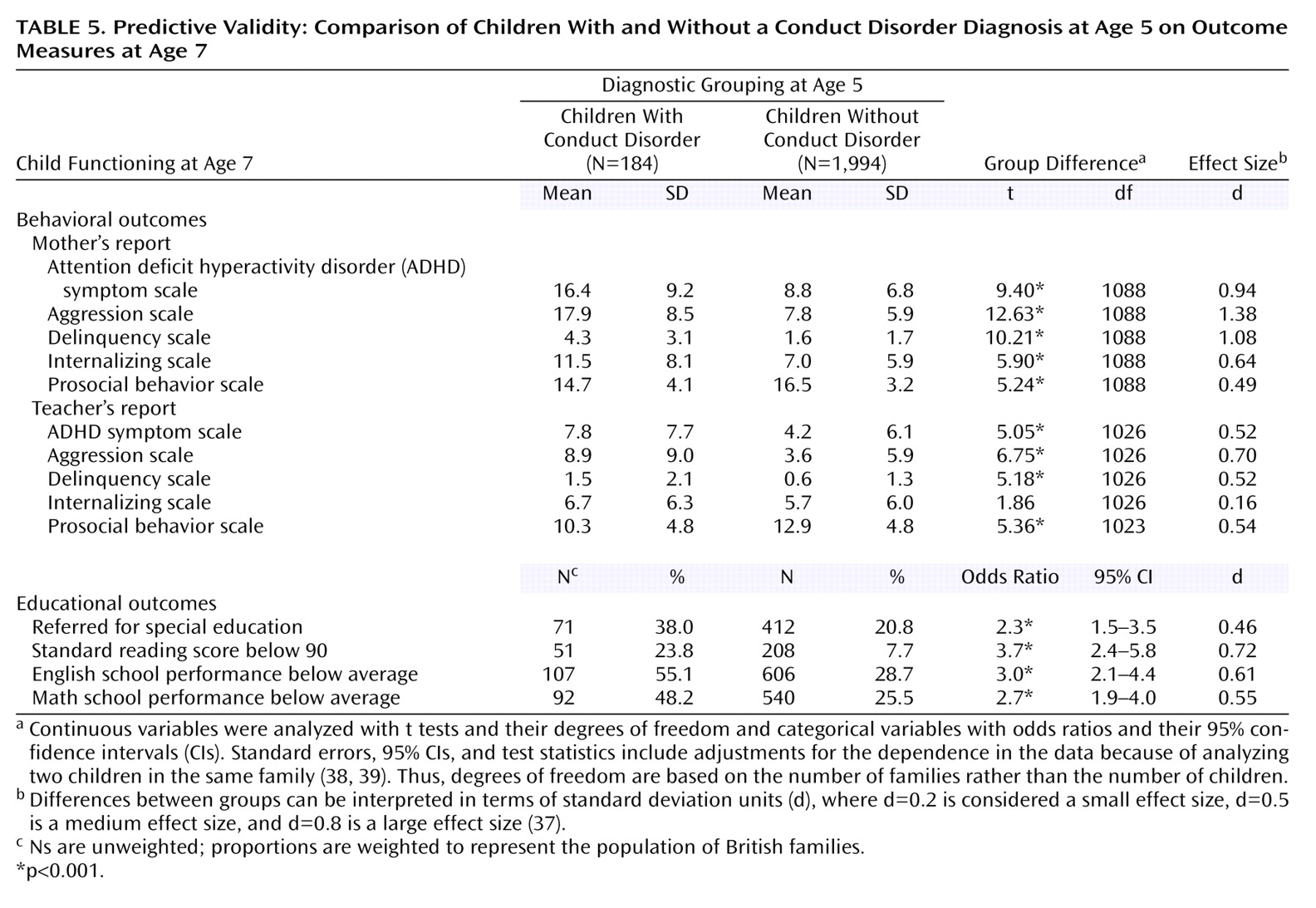
(6). The diagnosis would have predictive validity if children with and without a conduct disorder diagnosis at age 5 years differed on measures of behavioral and educational functioning later in childhood.
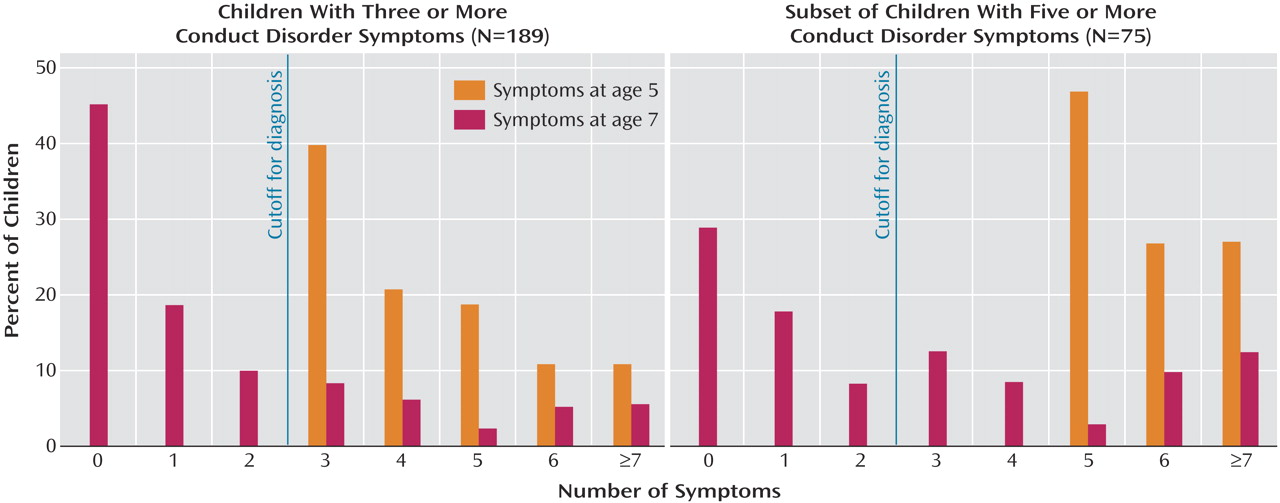
Additionally, we explored whether any children who were diagnosed with conduct disorder at age 5 did not have any conduct disorder symptoms 2 years later and whether these “remitted” children had outcomes at age 7 that would warrant concern.
Discussion
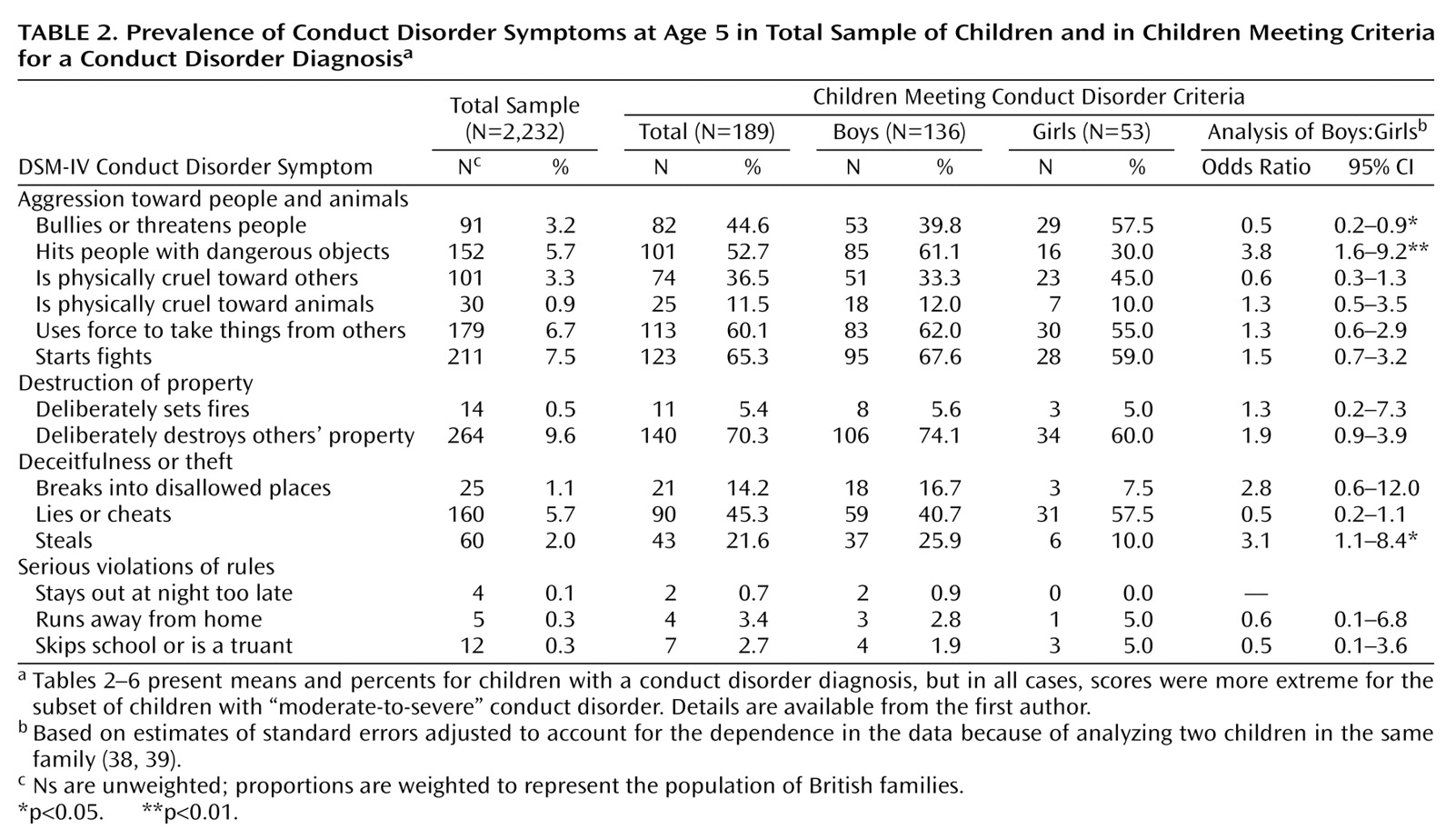
The utility of a diagnostic framework lies primarily in its ability to identify individuals who may need treatment. Applying DSM-IV diagnostic criteria for conduct disorder to 4½–5-year-old children appears to have succeeded in doing that. In a nonreferred, population-based sample, the conduct disorder diagnosis classified a small subset of children who were aggressive and antisocial. They also had lower executive functioning, lower IQ, and co-occurring ADHD symptoms—neurodevelopmental hallmarks of life-course persistent antisocial behavior
(41). Moreover, diagnosed children were disproportionately likely to come from backgrounds marked by low social class, single parenthood, family disruption, and parental psychopathology. Conduct-disordered children in our sample were disproportionately likely to have experienced harsh parenting and physical harm. Thus, the life contexts of young children identified as having conduct disorder in our study resemble the “criminogenic” environments that have been shown to interact with neurodevelopmental vulnerabilities to exacerbate behavior problems and promote antisocial personality development
(41). Concerns about the welfare of children diagnosed with conduct disorder increase, given that these children, regardless of whether they had any conduct disorder symptoms at follow-up, were disproportionately likely to have continuing behavioral and educational difficulties. Effect sizes for the association between risk factors and conduct disorder in our sample of young children are comparable to those reported for older children
(42,
43).
Whether valid diagnoses can be made of disruptive behavior disorders in preschool-age children has been a focus of controversy
(4,
44,
45). Some argue that disruptive behaviors in young children should not be pathologized because aggressive, destructive, and defiant behaviors, which characterize conduct disorder, are thought to be common and developmentally normative in the preschool period
(46), and most children will outgrow them
(47). Others believe that children falsely identified as having conduct disorder may be stigmatized, and unnecessary referral for treatment may waste health care resources. Some argue that the predictive accuracy of conduct problems for future conduct disorder improves only when children are older
(48), and applying diagnostic criteria validated for older children and adolescents to young children (i.e., “down-aging”) may promote overdiagnosis
(44).
Our research demonstrated that the co-occurrence of three or more conduct disorder symptoms, constituting a syndrome of problems, is rare and signals poor outcome. In this study, a large majority of children who had at least three (65%) or at least five (80%) DSM-IV conduct disorder symptoms at age 5 years, regardless of age-7 conduct disorder symptom status, had at least one educational difficulty 2 years later. Furthermore, the fact that the children’s conduct disorder diagnosis continued to predict teacher-rated educational difficulties at follow-up, after we controlled for age-5 IQ and ADHD diagnosis, suggests that the conduct disorder diagnosis uniquely captures a subset of young children who may have enduring school-related problems and on whom treatment resources would not have been wasted.
Clinicians wishing to minimize the risk of treating “false positives” can adopt a conservative approach by applying more stringent diagnostic criteria for moderate-to-severe conduct disorder. Moreover, diagnostic precision might be improved if specific age-appropriate guidelines are developed
(47). However, the present study shows that minimum DSM-IV criteria for a conduct disorder diagnosis were sensitive enough to identify young children who might benefit from intervention. Long-term studies of early-onset antisocial behavior have shown that true recoveries from conduct disorder are extremely rare because although not all conduct disorder children grow up to have antisocial personality disorder, virtually all children with conduct disorder have mental disorders and poor functioning in adulthood
(41). Fortunately, evidence has shown that interventions for preventing chronic conduct disorder can be effective if applied early in life
(49).
Four limitations temper the findings of this study. First, our sample comprised mostly white twins living in England and Wales. Therefore, our findings may not generalize to other ethnic or racial groups in other countries or to singletons. However, our estimate of the prevalence of conduct disorder of 2.5%–6.6% and the sex ratio of 3–5 boys per girl are comparable to other epidemiological studies of singletons in the United States
(50–
52). Second, we could not address the validity of the oppositional defiant disorder diagnosis because it was not assessed. Third, we report findings based on a “research” diagnosis that may differ from typical practice in clinical settings. However, we interviewed mothers face-to-face to assess symptoms and did not rely on self-administered checklists. Fourth, predictive validity analyses were limited to a 2-year follow-up period. Predictive validity for later childhood and adolescence should be tested.
The strengths of this study include features that directly address the limitations of existing research identified by Keenan and Wakschlag
(4): i.e., equal representation of preschool-age girls and boys in a large population-based sample, both teacher and mother reports of DSM-IV conduct disorder symptoms, and a longitudinal design with a high retention rate (98%).
Recently, a standardized interview
(53) and observational
(54) methods for making diagnoses in preschool-age children have been developed. This study adds to those efforts by demonstrating that interviewing mothers and gathering collateral reports from teachers can validly identify young children with DSM-IV conduct disorder.