All patients with bipolar affective disorder experience recurrent episodes of major depression, mania, hypomania, or mixed states, but the frequency with which episodes recur can range from one in several years to many per day
(1). As many as 20% of people with bipolar affective disorder experience rapid cycling, defined by DSM-IV as four or more affective episodes in a year
(1,
2). Rapid cycling is more common in women and in people with bipolar II disorder
(1,
3–5). Hypothyroidism, steroid hormones, and the use of antidepressants have been associated with rapid cycling, but these findings are controversial
(6–
10). Rapid cycling is just one extreme of the spectrum of episode frequency. Few studies have examined the full range of episode frequency in bipolar affective disorder.
Similarly, although bipolar affective disorder is a familial illness, the nature of episode frequency as a familial trait has not been investigated extensively
(1,
11). Several studies have addressed morbid risk for bipolar disorder among the relatives of rapid-cycling probands
(4,
5,
12,
13), and some studies have addressed the tendency of rapid cycling to run in families
(14,
15), but we are aware of no previous studies that directly measure the familiality of episode frequency. This issue is important, because the absence of familiality could suggest that episode frequency is under the primary control of nongenetic factors. We report here an analysis of episode frequency in families ascertained for a genetic linkage study of bipolar affective disorder. We also examined the relationship between episode frequency and age at onset, suicidal behavior, psychosis, panic disorder, alcoholism, substance abuse, and thyroid disease in these families. We found that episode frequency is a highly familial trait, associated with several indicators of severity, that may help define clinical subtypes of bipolar affective disorder with the greatest genetic liability.
Discussion
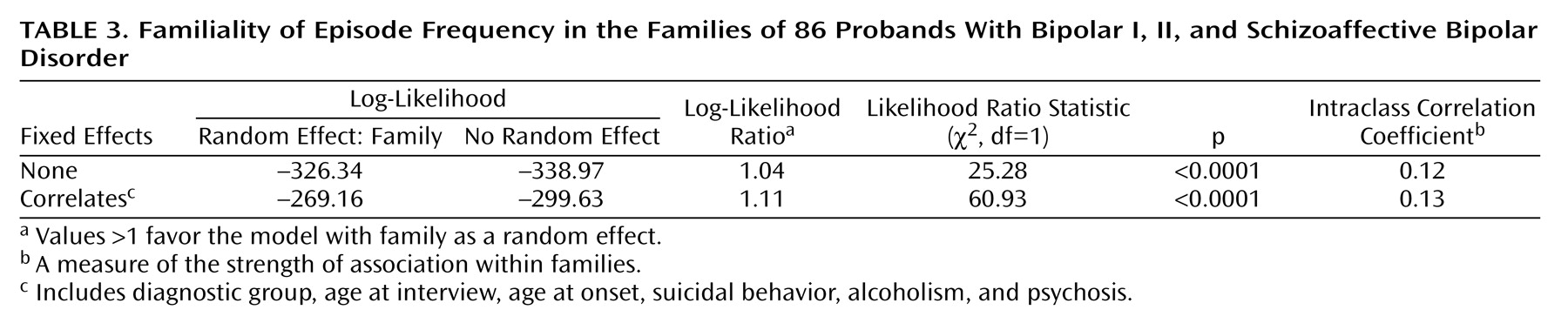
To our knowledge, this study demonstrated for the first time that episode frequency, defined as the number of affective episodes per year, is a familial trait in bipolar affective disorder. We further showed that the familiality of episode frequency is not accounted for by other, correlated variables, such as affective diagnosis subtype, psychosis, alcoholism, or suicidal behavior. As a familial trait associated with several indicators of disease severity, episode frequency may help to define clinical subtypes of bipolar affective disorder with greater genetic liability. These data did not support DSM-IV rapid cycling as the best predictor of familiality or severity.
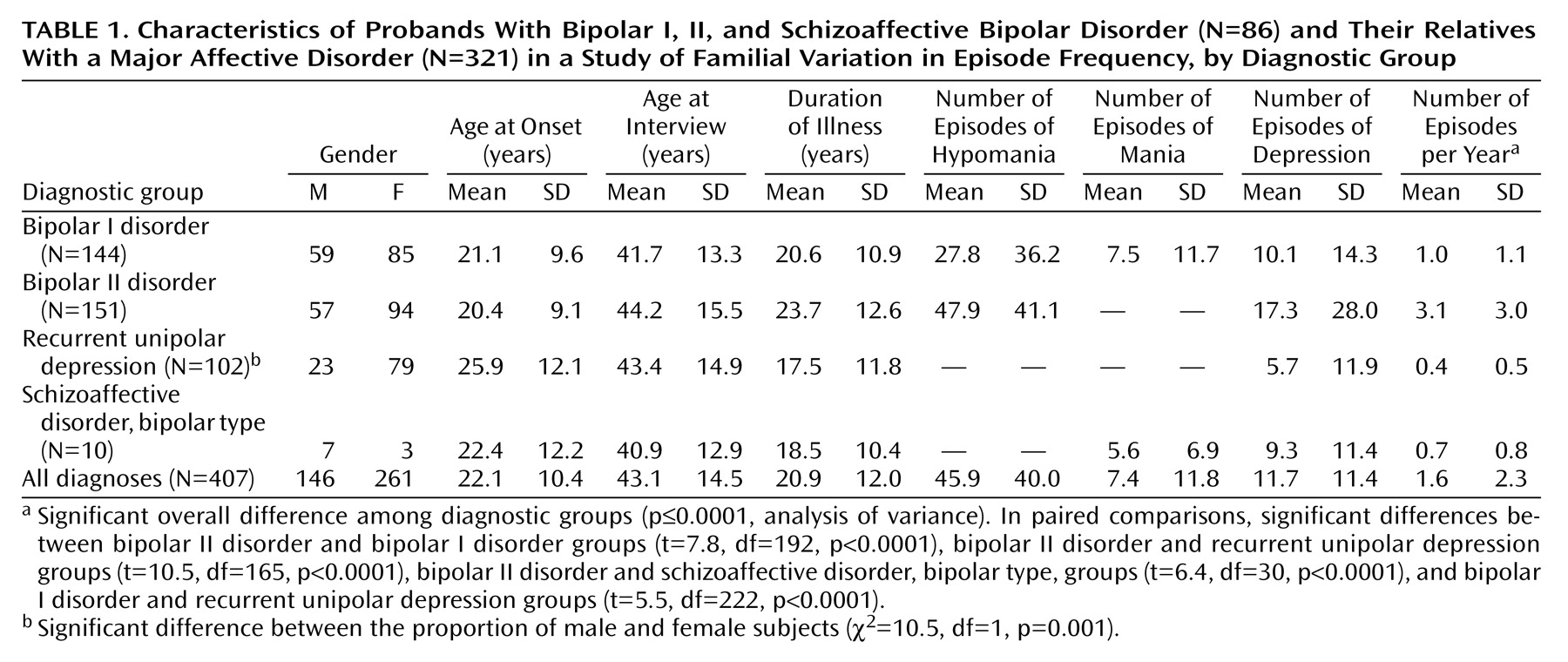
The data were collected from 407 subjects in 86 families, to our knowledge the largest data set ever studied for episode frequency. Diagnoses were highly reliable and were made by including all available data in a best-estimate procedure. The primary data used in estimating episode frequency were retrospective and thus subject to recall bias. There was no reason to expect, however, that relatives would be correlated in their recall bias; thus, recall bias alone cannot account for our findings. The data collection methods had other limitations. Subjects with two or more episodes of mania were not questioned in detail about all hypomanic episodes. Thus, true episode frequency was probably underestimated for subjects with bipolar I disorder. This underestimation was also unlikely to account for our main findings, because the exclusion of hypomanic episodes did not change the distribution of episode frequency in this study group. No data were collected on treatment, so it was not possible to control for potential treatment effects on episode frequency in these data.
DSM-IV defines subjects with four or more major affective episodes in a year as having rapid cycling. The published studies of rapid-cycling subjects, so defined, have not consistently detected familial aggregation
(4,
5,
12–15). We found little support for the DSM-IV definition of rapid cycling in this study group. As a categorical trait, rapid cycling was not familial in this analysis, even though we found significant evidence of familiality when we considered subjects across the full range of episode frequency. Rapid cycling was associated with the diagnosis of bipolar II disorder, but it was not correlated with any of the other clinical features we examined. Our retrospective data did not allow us to identify subjects with discrete periods of rapid cycling punctuating a course of illness with few other episodes. We cannot rule out familial effects in these subjects.
The evidence linking hypothyroidism and rapid cycling is controversial. The association of hypothyroidism with major affective disorders and the presence of thyroid antibodies in patients with major affective disorders have been described in numerous publications, but the biological relationship between these two illnesses remains unclear
(6–
8,
10). Our data, which relied solely on subjects’ self-report, were limited by lack of information from thyroid function tests and thyroid antibodies assays. Nevertheless, the rate of reported thyroid disease among unaffected subjects (6%) appeared similar to the population rate of 5.9%
(26), and the rate of reported thyroid disease among the lithium-treated subjects was similar to that reported in another study
(27). Thus, we do not appear to have greatly under- or overestimated the rates of thyroid disease in these study subjects. We found, as have others, that thyroid disease was more common among affected subjects and that this difference remained significant even after subjects with a history of lithium exposure were dropped from the analysis. We found no association between thyroid disease and episode frequency in the study group, consistent with previous studies
(4,
5,
28).
Alcoholism and substance abuse are known to be highly associated with major affective disorders
(1,
24,
25). In a previous study that included some of the subjects also included in the present analysis, alcoholism was found to be associated with a higher rate of suicide attempts and to be clustered in a subset of families
(29). The present study extended this finding by demonstrating that alcoholism and suicide attempts are both strongly associated with episode frequency. Our new results suggest that the association between alcoholism and suicidal behavior is mediated, at least in part, by an increase in episode frequency.
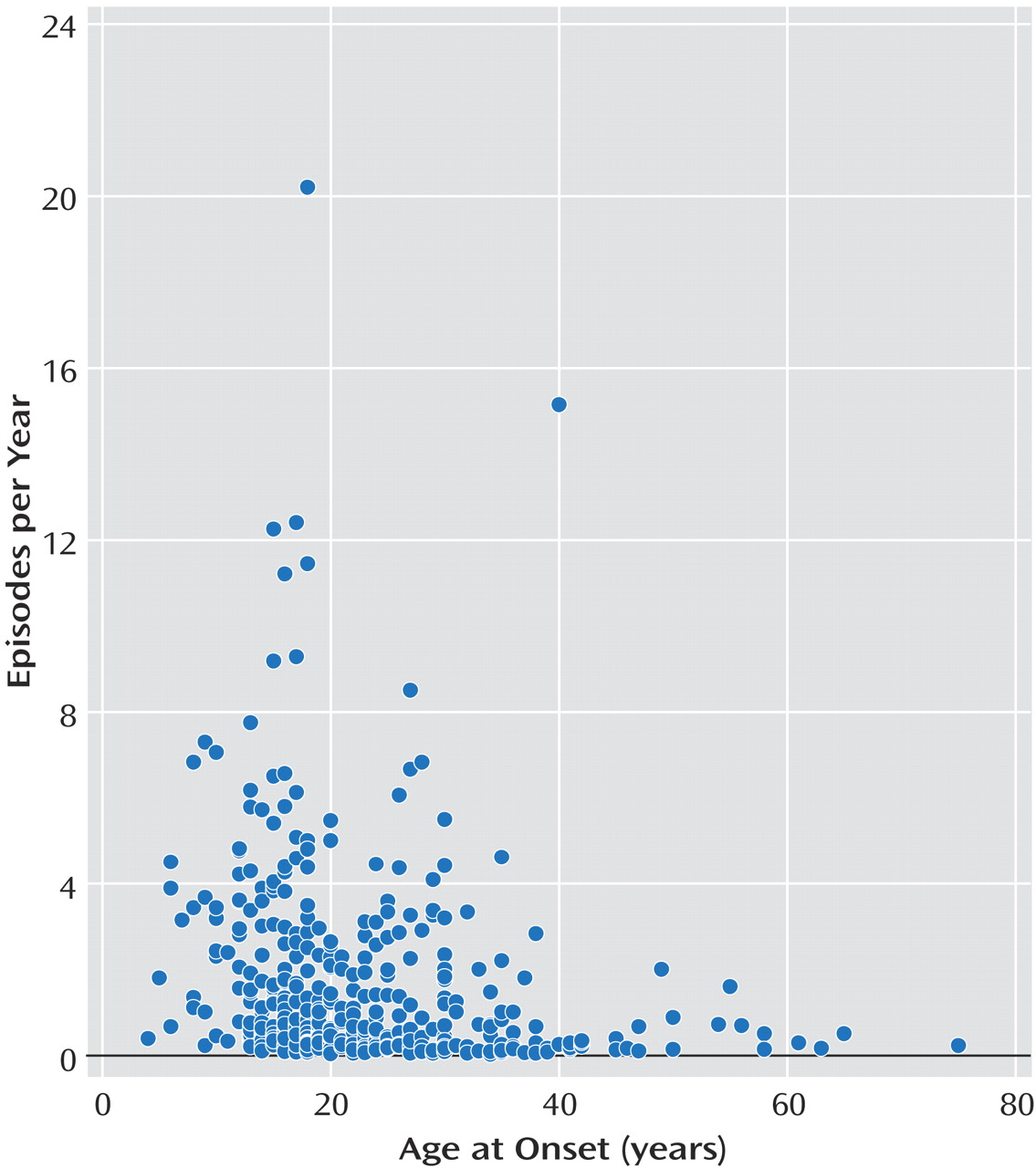
Episode frequency was also associated with other clinical features of bipolar affective disorder. Age at onset (itself a significant predictor of prognosis, comorbidity, and treatment response in bipolar affective disorder
[30]) was strongly associated with episode frequency in this study group. We also found that episode frequency was significantly associated with psychotic features. It is possible that episode frequency accounts for some of the tendency of psychotic features to run in families with bipolar affective disorder
(31,
32). An earlier analysis of a subset of these subjects indicated that episode frequency tended to increase in successive generations of a pedigree, a phenomenon known as anticipation
(33). A complete analysis of anticipation is beyond the scope of the study reported here, but if anticipation were present in the current study group, it would tend to decrease the familiality of episode frequency and thus could not account for our findings.
It may come as a surprise that the highest quartile of episode frequency contained many subjects with bipolar II disorder, which is traditionally considered less severe than bipolar I disorder, as well as many subjects with early onset, psychotic features, alcoholism, and suicidal behavior, clear indicators of a severe illness. This finding is consistent with previous reports indicating more chronicity and a higher rate of comorbidity and suicidal behavior in bipolar II disorder, compared to bipolar I disorder
(34,
35). These results imply that the traditional view of severity, which emphasizes mania, may be too narrow. Bipolar II disorder is in many ways more “severe” than bipolar I disorder.
These findings have implications for genetic research in bipolar affective disorder. As a quantitative trait, episode frequency may offer an alternative phenotype that would be more powerful than the categorical phenotypes typically used in genetic linkage and association studies. Episode frequency may also offer an approach to genetic heterogeneity in bipolar affective disorder, because subjects with similar episode frequencies may be more likely to share genetic determinants. Episode frequency is also associated with several indicators of disease severity. To the extent that disease severity is related to genetic liability, episode frequency may help to define clinical subtypes of bipolar affective disorder with a greater burden of genetic risk factors. However, further data concerning the heritability of episode frequency—for example, in twins—is needed before we can make confident predictions about the potential value of episode frequency as a phenotype in genetic research.
In conclusion, we found that episode frequency is a familial trait in bipolar affective disorder. These data also raise concerns about the DSM-IV definition of rapid cycling in bipolar affective disorder. We suggest that episode frequency is an important clinical feature of bipolar affective disorder, with implications for severity, comorbid conditions, and genetic research.