To address these issues, we assessed episode frequency from prospective daily mood ratings and compared retrospective and prospective illness variables in patients with a rapid-cycling and a non-rapid-cycling course. In addition to classifying rapid cycling by using the traditional definition of four or more mood episodes per year, we examined these clinical characteristics in relationship to the dimension of episode frequency in an attempt to discern an empirically based boundary for rapid cycling, if present.
Results
Comparison of Patients With and Without Rapid Cycling
The 539 patients with 1 year of prospective ratings included 237 men (44.0%) and 302 women (56.0%). Their mean age was 42.1 years (SD=11.5). A total of 206 (38.2%) had rapid cycling, and 333 (61.8%) did not have rapid cycling. A lifetime history of rapid cycling was reported at study entry by 264 (50.7%) of 521 patients. The demographic and clinical characteristics of the current study group did not differ from those of a larger group of 631 patients that included patients with a shorter follow-up period or incomplete ratings
(12).
The patients’ clinical characteristics at study entry are summarized in
Table 1. There was a nonsignificant overrepresentation of women in the rapid-cycling group. Educational level, marital status, and work status did not differ significantly between the groups (data not shown). Rapid cycling occurred in 41.3% of patients with bipolar I disorder and 27.9% of patients with bipolar II disorder. Patients with rapid cycling had an earlier age at onset, a longer duration of illness, and a longer time from first symptoms to first medication treatment, compared to the patients without rapid cycling. There was a strong relationship between the occurrence of rapid cycling in any prior year, in the year before study entry, and during prospective follow-up. Rapid cycling was associated with a prior history of dysphoric mania/hypomania, lifetime treatment with antidepressants, and a history of substance-induced episodes.
Rapid cycling was associated with lifetime DSM-IV anxiety disorder, childhood physical or sexual abuse, and parental history of drug abuse, as detailed in
Table 2.
Multivariate logistic regression (N=397) identified five independent variables that were significantly associated with rapid cycling: a lifetime history of rapid cycling (Wald’s χ2=17.64, df=1, p<0.0001, odds ratio=3.39), higher number of lifetime mood episodes at study entry (11–20 episodes: Wald’s χ2=5.24, df=1, p=0.02, odds ratio=4.66; >20 episodes: Wald’s χ2=8.51, df=1, p=0.004, odds ratio=6.49), bipolar I disorder subtype (Wald’s χ2=8.22, df=1, p=0.004, odds ratio=2.76), lifetime history of drug abuse (Wald’s χ2=4.57, df=1, p=0.03, odds ratio=1.99), and history of childhood physical and/or sexual abuse (Wald’s χ2=4.67, df=1, p=0.03, odds ratio=1.86).
Prospective Course of Illness
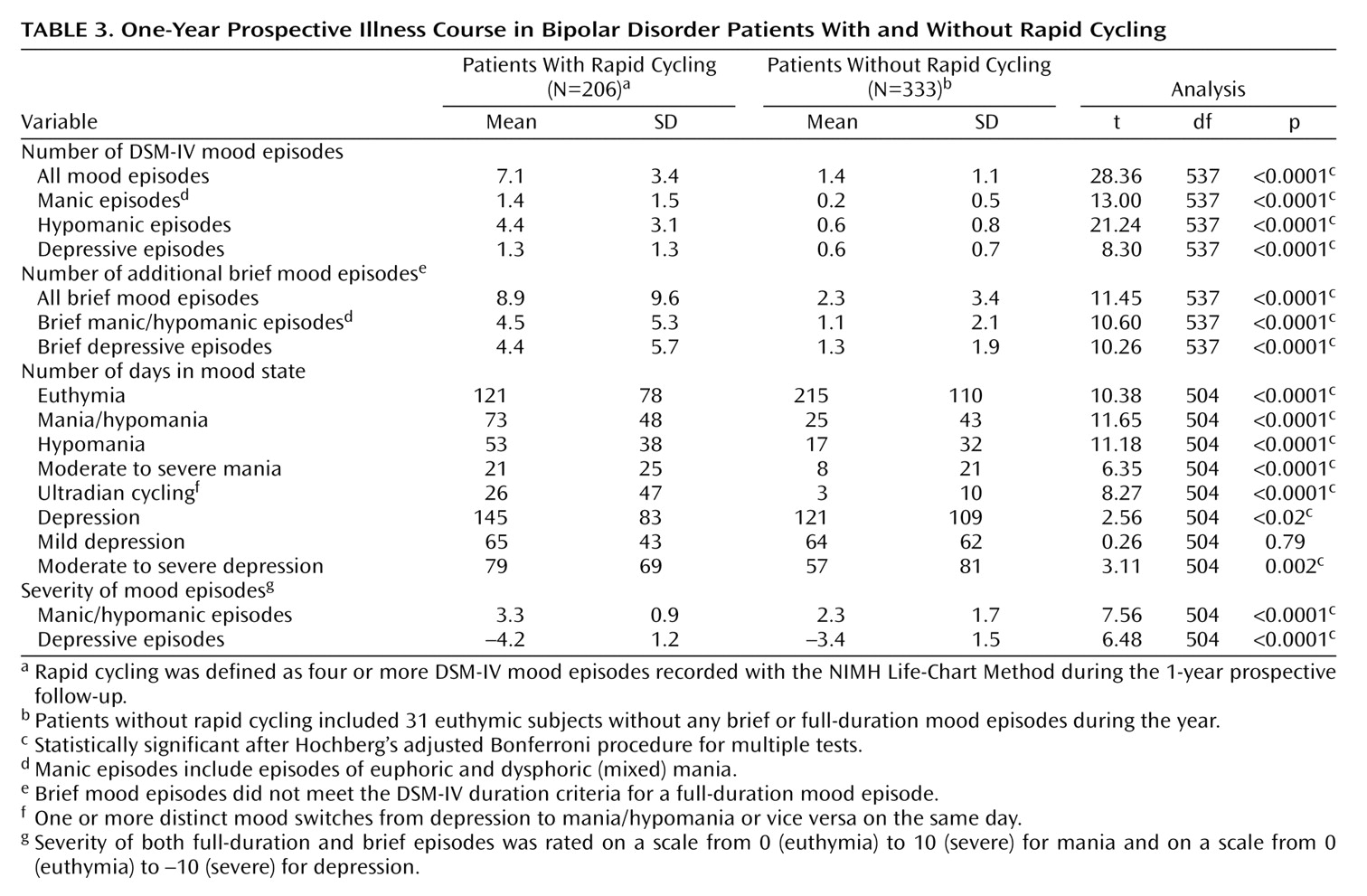
As summarized in
Table 3, patients with rapid cycling had a sevenfold greater mean number of full-duration manic and hypomanic episodes and a twofold greater mean number of depressive episodes, compared to patients without rapid cycling. Over the course of the year, patients with rapid cycling spent many more days in a manic or hypomanic state than did patients without rapid cycling (73 days versus 25 days). Patients with rapid cycling also spent more days depressed, although the difference between groups was smaller (145 days versus 121 days). During follow-up, patients with rapid cycling were twice as likely to experience dysphoric mania/hypomania as were patients without rapid cycling (82.5% versus 38.1%) (χ
2=99.56, df=1, p<0.0001).
Lithium, valproate, carbamazepine, or lamotrigine was used alone or in combination by 193 (93.7%) of the patients with rapid cycling and 305 (91.6%) of the patients without rapid cycling. Patients with rapid cycling were more likely than those without rapid cycling to be given antidepressants (67% versus 57%) (χ2=4.60, df=1, p=0.03), antipsychotics (52% versus 32%) (χ2=19.08, df=1, p<0.00001), and thyroid hormone (32% versus 22%) (χ2=6.71, df=1, p=0.01).
Variables Related to Episode Frequency
The subjects were grouped by the number of full-duration DSM-IV episodes in the first year of prospective follow-up, as follows: no episodes (N=74) and one (N=110), two (N=78), three (N=71), four (N=46), five (N=39), six (N=24), seven (N=24), eight (N=22), nine (N=13), and 10 or more episodes (N=38).
Figure 1 illustrates prospective illness characteristics in relation to overall episode frequency. Increasing episode frequency was largely attributable to manic and hypomanic episodes. The number of DSM-IV depressive episodes was relatively constant in the groups of patients with five or more full-duration DSM-IV-defined mood episodes per year. Similarly, the average number of days per year during which patients experienced hypomanic, manic, or ultradian cycling gradually increased with the number of full-duration DSM-IV-defined episodes per year, and the average number of days during which patients were depressed was relatively consistent among the groups of patients with one or more episodes per year. The number of additional brief episodes progressively increased along with the frequency of full-duration DSM-IV-defined episodes.
Figure 2 shows the relationship between the overall frequency of full-duration DSM-IV-defined episodes and the prevalence of the variables that distinguished patients with and without rapid cycling. Except for bipolar I disorder subtype and female gender, these variables tended to increase in prevalence as a function of episode number (r=0.15–0.37, all p<0.0001). The prevalence of bipolar I disorder subtype had a somewhat uneven pattern. An increase in the percentage of female patients at eight episodes could indicate nonlinearity; 53% of patients with zero to seven episodes were women, compared to 73% of patients with eight or more episodes (χ
2=8.65, df=1, p=0.003), although the percentage of women among patients with nine and 10 or more episodes was lower than the percentage of women among patients with eight episodes. None of the other curves showed evidence of nonlinearity suggestive of this or any other cutoff point for separating patients with rapid cycling from those without rapid cycling. We reanalyzed the comparisons reported in
Table 1 and
Table 2 with a definition of rapid cycling as eight or more episodes; 73 subjects had rapid cycling according to this definition. Female gender was the only variable with a greater significance in the reanalysis than in the original analysis (data not shown).
Discussion
To our knowledge, this study is the first comparative investigation of rapid-cycling and non-rapid-cycling bipolar disorder that systematically used both a categorical and a dimensional analysis and is one of the few studies
(18,
19) in which the diagnosis of rapid cycling was based on prospectively observed episode frequency.
In this group of 539 outpatients with bipolar disorder, prospective evaluation revealed a 38% prevalence of rapid cycling as defined by DSM-IV criteria. Notable findings in patients with rapid cycling were considerably greater severity and frequency of manic episodes and a greater severity of depressive episodes, compared to patients without rapid cycling. Patients with rapid cycling had as many brief mood episodes as full-duration DSM-IV episodes. However, there was a lack of clear boundaries between the patients with and without rapid cycling on any of the prospective and retrospective variables examined as a function of episode number.
The prospective course of illness indicates that the study subjects were considerably ill despite extensive treatment. The prospective illness characteristics of the 419 bipolar I disorder patients were similar to findings in a group of 146 patients with bipolar I disorder who were followed for 2–20 years in the Collaborative Depression Study
(20). The patients in the Collaborative Depression Study were depressed an average of 31.9% of the time, manic for 2.3%, hypomanic for 7.0%, and cycling/mixed for 5.9%. The patients in our study experienced those mood states 35.6%, 3.9%, 8.7%, and 3.3% of the time, respectively.
These findings confirm that the main burden for a majority of patients with bipolar illness is depression
(21); patients with rapid cycling were depressed 39.5% of the time, and patients without rapid cycling were depressed 33.2% of the time. It is interesting to note that in all patients (both with and without rapid cycling) who had one or more full-duration episodes per year, the average amount of time in a depressed state was fairly stable, regardless of the total number of episodes (
Figure 1). In contrast, the proportion of time in a hypomanic, manic, or ultradian cycling state was significantly higher in patients with rapid cycling (27.1% of the time versus 7.7% of the time in patients without rapid cycling) and increased progressively as a function of episode frequency.
When we compared the prior illness histories of the patients with and without rapid cycling, we found that five independent variables were associated with rapid cycling in the logistic regression analysis: previous rapid cycling, a greater number of previous mood episodes, bipolar I disorder subtype, history of childhood physical and/or sexual abuse, and lifetime drug abuse.
A previous history of rapid cycling and a history of more than 10 mood episodes before study entry were the strongest predictors of rapid cycling during the first year of prospective follow-up. This finding suggests that some patients have a propensity toward rapid cycling that may be expressed periodically or more continuously.
Our finding that rapid cycling was more prevalent among patients with bipolar I disorder contrasts with various reports of overrepresentation of patients with rapid cycling among bipolar II disorder patients
(6). However, two large studies also failed to report a preponderance of rapid-cycling patients among patients with bipolar II disorder
(22,
23).
Childhood physical or sexual abuse was associated with higher episode frequency. We previously reported that early abuse was associated with an earlier age at onset of bipolar disorder, serious suicide attempts, and comorbid drug abuse and anxiety disorders
(12). These findings suggest that early traumatic experiences may contribute to a later adverse illness course.
Substance abuse is highly comorbid with bipolar disorder
(11), and patients with rapid cycling may be particularly sensitive to the destabilizing properties of alcohol and drugs, as they frequently reported prior induction of depressive and manic/hypomanic episodes by these agents. Alternatively, patients with faster cycling frequencies may use these substances at a higher rate.
Several factors were associated with rapid cycling in the univariate but not in the multivariate analysis, indicating that these factors were intercorrelated with one or more of the factors mentioned earlier. As in other studies
(6), we found a modest overrepresentation of women among the patients with rapid cycling, especially among those with higher episode frequencies. Our finding of a younger age at onset of bipolar disorder in patients with rapid cycling was also found in previous studies
(23–
25), as was our finding of a longer duration of illness in patients with rapid cycling
(4,
5), although most studies reviewed found no differences
(6). Our finding of a longer time between first symptoms and first medication treatment in patients with rapid cycling raises the question of whether earlier recognition and treatment might prevent or attenuate this more problematic course.
Prior histories of both dysphoric mania/hypomania and ultradian cycling were more prevalent in patients with rapid cycling than in patients without rapid cycling. These associations were confirmed during prospective follow-up, which suggests that depressive features pervade both manic and depressive phases of the illness in patients with faster cycle frequencies. Our study was not designed to evaluate the contribution of antidepressants to the development of rapid cycling. Still, 54% of patients in the study who had been treated with antidepressants reported having experienced an antidepressant-induced switch to mania/hypomania in the past, a phenomenon that has been associated with a subsequent rapid-cycling course
(26).
The most rigorous studies of family history of mood disorders reported no significant differences in family history between patients with and without rapid cycling
(4–
6,
19,
27,
28). We found that a parental history of major mood disorder (bipolar disorder and/or depression) was more likely in patients with rapid cycling than in those without rapid cycling. More prominent was our finding of a parental history of drug abuse in patients with rapid cycling. However, rapid cycling was also associated with the occurrence of childhood adversity, which suggests that parental substance abuse and the associated environmental instability may have indirectly contributed to the risk of rapid cycling.
The results of our study must be considered in the context of several limitations. Although our study population is in many respects comparable to other groups of outpatients
(10), 80% of the subjects in our study had bipolar I disorder, almost 60% reported a lifetime history of psychotic symptoms, and 38% had a rapid-cycling course. This greater overall severity of illness may restrict the generalizability of our findings. The exclusion of patients with less than 1 year of follow-up may have affected the representativeness of the study subjects. Moreover, the retrospective data on previous illness characteristics covered a period of many years and thus were susceptible to inaccuracies. An inevitable limitation is the fact that we studied the naturalistic course of treated bipolar disorder.
Despite these limitations, our findings can be used in the further conceptualization of rapid cycling in bipolar disorder, defined as the occurrence of four or more mood episodes per year
(1). Kendell
(29) proposed that boundaries between two clinical syndromes may be indicated by a nonlinear relationship between symptom measures and an independent variable on which the syndromes differ markedly. Like Bauer et al.
(3), we found no bimodal distribution of the number of episodes per year. They reported that the proportion of women increased markedly among patients with four to eight episodes per year and even reached 100% among patients with nine or more episodes per year. We found a larger proportion of women among patients with eight or more episodes per year. However, this potential nonlinearity was not confirmed in analyses of any of the other risk factors we examined (
Figure 1). Likewise, changing the boundary for rapid cycling from four to eight episodes per year did not essentially change the results of our dichotomous comparisons.
In conclusion, our overall findings suggest that rapid cycling is a dimensional course specifier with an arbitrarily defined cutoff at four episodes per year on a continuum of episode frequency seen in the naturalistic course of treated outpatients with bipolar disorder.