Pervasive developmental disorders—the most common of which include autistic disorder, Asperger’s disorder, and pervasive developmental disorder not otherwise specified—are highly heritable and may lie along a severity continuum determined by a common set of genetic susceptibility factors
(1). Autistic traits with severity that falls below the clinical threshold for a pervasive developmental disorder diagnosis have been found to aggregate in the family members of autistic individuals
(1,
2).
A limitation of previously published family studies has been the lack of a validated method for quantitative assessment of heritable subsyndromal autistic traits. Recent advances, however, have made such quantitative characterization possible
(3–
5). In this study, we measured familial aggregation of such traits among the siblings of children with and without pervasive developmental disorders. We limited the siblings to brothers in order to avoid underestimation of familial aggregation, since lower phenotypic expression of genetic susceptibility in female subjects has been observed in studies of autistic traits in the general population
(3).
Method
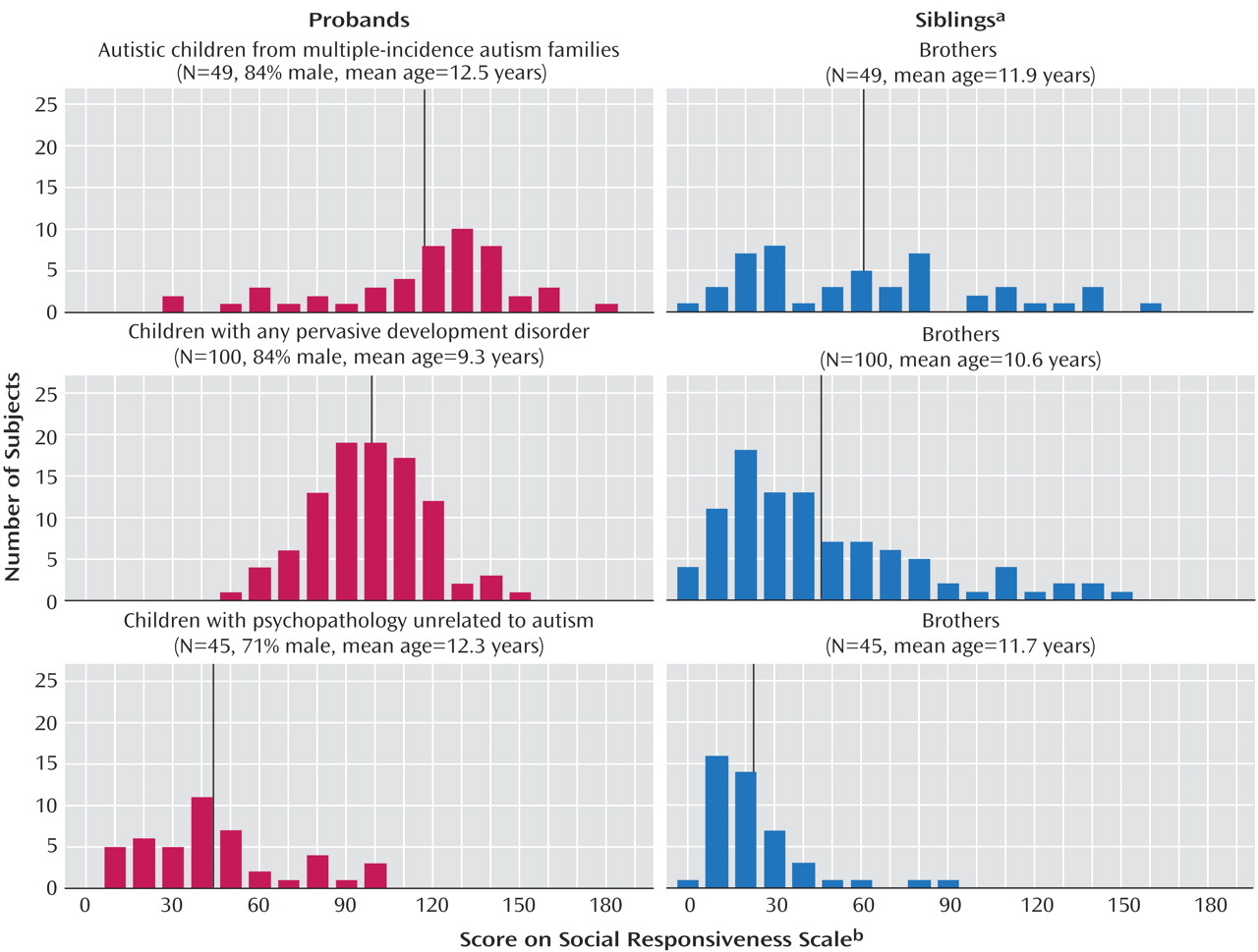
Subjects were recruited from two sources: the Autism Genetic Resource Exchange and the Washington University Child and Adolescent Psychiatry Service. The Autism Genetic Resource Exchange preferentially selects for multiple-incidence autism families, and for this study 49 families were recruited by mail from a pool of 75 families eligible on the basis of 1) at least one known nonautistic boy in the family and 2) prior completion of the entire Autism Genetic Resource Exchange research protocol. Washington University serves a clinical population representing the entire range of pervasive developmental disorder diagnoses (as well as all other child psychiatric conditions), and for this study, 145 families were consecutively enrolled on the basis of recruitment mailings and follow-up phone contacts. All Washington University probands were diagnosed independently by two expert clinicians. All autistic disorder diagnoses were confirmed with the Autism Diagnostic Interview—Revised. Because Washington University did not preferentially select for multiple-incidence families, autistic probands from the two sources were maintained in separate groups for data analysis.
One proband from each family was assessed along with the closest-in-age brother (since the Autism Genetic Resource Exchange preferentially selected for multiple-incidence families, the closest-in-age nonautistic brother was selected to allow more conservative estimation of familial aggregation). Thus, three sibling pair groups were studied: 1) autistic probands from multiple-incidence families and their closest-in-age nonautistic brothers (N=49 pairs); 2) probands with any pervasive developmental disorder (autistic disorder [N=27], Asperger’s disorder [N=8], or pervasive developmental disorder not otherwise specified [N=65]) and their closest-in-age brothers (N=100 pairs); 3) probands with psychopathology unrelated to autism (disruptive behavior disorders, primarily ADHD [N=28], affective disorders [N=6], or anxiety disorders [N=11]) and their closest-in-age brothers (N=45 pairs). The subjects were predominantly Caucasian and ranged in age from 4 to 18 years.
After obtaining written informed consent, the Social Responsiveness Scale scores for the probands and their brothers were obtained from both parent report (94% completion rate) and teacher report (83% completion rate). The Social Responsiveness Scale capitalizes on observations of children in natural social contexts and distinguishes children with a pervasive developmental disorder from those with other psychiatric conditions
(3,
4). It generates a singular severity score for autistic social impairment (higher score equates with greater severity), use of which has been validated by extensive factor and cluster analyses among clinical and nonclinical populations
(4). Social Responsiveness Scale scores are highly heritable in males
(3,
5) and generally unrelated to age (from 7 to 18 years) and IQ. Composite nonverbal IQ scores on the Raven Colored Progressive Matrices obtained from the Autism Genetic Resource Exchange autistic subjects were not significantly correlated with Social Responsiveness Scale scores (Pearson’s r=–0.16).
The mean Social Responsiveness Scale score from all available informants was calculated for each subject (parent report/teacher report correlation: r=0.76). These were compared across the sibling groups using single-factor analysis of variance (ANOVA), with and without square-root transformation (which resulted in absolute values for skew of less than 0.5 in both the proband and sibling distributions). Two-factor ANOVA (proband diagnostic group, proband versus sibling status) was also employed for an overarching analysis of all study groups.
Discussion
Siblings of children with pervasive developmental disorders, who have a 10-fold increase in risk for affected pervasive developmental disorder status, are also more likely than their counterparts in unaffected families to exhibit subthreshold levels of autistic social impairment. This increased liability was observed among siblings of autistic probands from multiple-incidence autism families and to a lesser (but still highly significant) extent among siblings of probands with any pervasive developmental disorder. Subthreshold autistic impairments were quantitatively measured in this study by using an instrument (the Social Responsiveness Scale) for which scores have been shown to be highly heritable in male subjects
(3,
5), and sibling intraclass correlation for Social Responsiveness Scale scores in this clinical study group (ICC=0.35) was consistent with that observed in twins in the general population
(3). Therefore, these findings add to the body of evidence suggesting that the specific genetic susceptibility factors responsible for pervasive developmental disorders may also be responsible for more common social impairments, the severity of which falls below the threshold for a categorical pervasive developmental disorder diagnosis.
This study was limited to some degree by size and by variation in ascertainment strategy across the two primary sources of subjects. Although the findings support an additive genetic model for a substantial proportion of autism/pervasive developmental disorder cases, the family data collected were not extensive enough to determine whether genes of major effect are operative in specific subsets of families (as occurs, for example, in rare autistic syndromes associated with tuberous sclerosis). Future studies involving larger numbers of subjects, parents
(5), and extended pedigrees are warranted to confirm and extend these findings. Additional support for shared genetic liability across the disorders in the autism spectrum comes from a recent Danish national register-based study (N=943,664 children) that showed elevated rates of autistic disorder among both the siblings of autistic probands and the siblings of children with other pervasive developmental disorders, including Asperger’s disorder
(6).
We conclude that across categorically defined pervasive developmental disorder diagnoses, genetic susceptibility is manifested by familial aggregation of continuously distributed (subsyndromal) autistic traits, and that genetic studies may be enhanced by quantitative assessment of those traits across the entire range of severity with which they occur in affected families.