There has been increasing interest in recent years in helping people with severe mental illness, and particularly those with a diagnosis of schizophrenia, return to competitive employment in the general economy
(1). Supported employment, in which rehabilitation specialists work simultaneously with consumers and employers to facilitate rapid job placement with ongoing support, has been shown in numerous clinical trials to improve rates of competitive employment
(1–
4) and has been recognized as an evidence-based practice that was strongly advocated in the report of the President’s New Freedom Commission on Mental Health
(5). Despite these advances, a review of eight controlled trials showed that employment rates for people with schizophrenia, even with optimal support, range from only 30% to 80%, with a median of 60% across studies
(6). Further research is thus needed to examine the patient and community characteristics associated with either improved or reduced chances of employment. One recent study showed that although symptoms of schizophrenia constitute a statistically significant impediment to employment, a 40% reduction in all symptoms would increase employment by only 8%
(7). However, that study did not include measures of neurocognitive function, which has been shown to be positively associated with social functioning in people with mental illnesses
(8), or receipt of disability payments, which also may constitute an important impediment to employment
(9,
10). To our knowledge, no study has considered the effect of all of these factors on employment together with environmental factors, such as the availability of vocational rehabilitation services in the community and local unemployment rates. It has become clear that employment among disabled Americans declined precipitously during the 1990s, especially among people with mental illness
(11). A comprehensive examination of a broad range of potential barriers to employment for people with schizophrenia, perhaps the most disabling mental illness, is needed to identify directions for further clinical and policy initiatives.
From 2001 to 2003, baseline data from more than 1,400 patients with schizophrenia at more than 50 U.S. sites were collected as part of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, a major multisite trial funded by the National Institute of Mental Health to investigate antipsychotic pharmacotherapy
(12). In the study reported here, baseline data from the CATIE study were used to examine the association of diverse sociodemographic, clinical, and environmental factors with participation in competitive employment, with participation in other employment activities (volunteer work, workshop, or prevocational programs), and, among those who were employed, with reported monthly earnings.
Method
The CATIE study was designed to compare the cost-effectiveness of currently available atypical and conventional antipsychotic medications through a randomized clinical trial involving a large sample of patients treated for schizophrenia at multiple sites, including both academic sites and more representative community providers. Participants gave written informed consent to participate in protocols approved by local Institutional Review Boards. Details of the study design and entry criteria have been presented elsewhere
(12). The current study relied exclusively on baseline data collected before randomization and the initiation of experimental treatments. Data from one site (33 patients) were excluded because of concerns about their quality.
Measures
The dependent variable of principal interest in this study is a three-level nominal variable with which patients were classified as participants in 1) competitive employment (if they reported any earned income in the previous month), 2) other (noncompetitive) employment activities (if they responded affirmatively to a series of questions concerning participation in supported or sheltered employment, volunteer or irregular work, or prevocational activities such as job search, classes, or vocational assessment), or 3) no employment activity. Those who reported both earned income in the previous month and participation in other employment activities were included in the competitively employed group. The employed patients earned a monthly average of $808 (SD=945).
Questions concerning sociodemographic status were used to document age, race, gender, marital and educational status, and sources of income, including earned income, Social Security payments (Social Security Disability Insurance [SSDI] or Supplemental Security Income [SSI]), and Department of Veterans Affairs (VA) compensation and pension payments.
The diagnosis of schizophrenia was confirmed with the Structured Clinical Interview for DSM-IV
(13). Symptoms of schizophrenia were assessed with the rater-administered Positive and Negative Syndrome Scale (PANSS), which yields a total average symptom score, based on 30 items rated from 1 to 7 (with higher scores indicating more severe symptoms), as well as subscale scores that reflect positive, negative, and general symptoms
(14).
The Heinrichs-Carpenter Quality of Life Scale
(15) is a rater-administered scale used to assess overall quality of life and functioning. The scale’s 21 items are rated from 0 to 6 (with higher scores reflecting better quality of life) and yield measures on four subscales that address 1) social activity, 2) instrumental functioning, 3) use of objects and participation in activities, and 4) intrapsychic functioning. The intrapsychic functioning subscale addresses psychological characteristics such as motivation, curiosity, anhedonia, and empathy that are distinct from schizophrenia symptoms. One item in this subscale concerns time utilization and was judged, at face value, to be directly related to employment. This item was excluded to create a five-item modified intrapsychic functioning subscale.
Medication side effects were assessed with the Barnes Rating Scale for Drug-Induced Akathisia (possible range=0–11)
(16), the Abnormal Involuntary Movement Scale for tardive dyskinesia (possible range=0–28)
(17), and the Simpson-Angus Rating Scale for extrapyramidal symptoms (possible range=0–40)
(18). Depression was measured with the Calgary Depression Rating Scale (possible range=1–4)
(19), and substance use was measured with the Alcohol Use Scale and Drug Use Scale (possible range for each scale =1–5)
(20).
Neurocognitive functioning was measured with several tests, which were described in a previous publication
(21). The test scores were converted to z scores and combined to construct five separate scale scores that were themselves averaged to form a composite neurocognitive functioning score. The five scale scores measured 1) processing speed (the average of three components: Grooved Pegboard score, WAIS-R digit symbol test score, and the average of the scores on the Controlled Oral Word Association Test and Category Instances), 2) verbal memory (average score on three trials of the Hopkins Verbal Learning Test), 3) vigilance (average of Continuous Performance Test d′ scores for 2-digit, 3-digit, and 4-digit trials), 4) reasoning (average of scores on the Wisconsin Card Sorting Test and WISC-R mazes test), and 5) working memory (the average of scores on computerized tests of visuospatial working memory [sign reversed] and letter-number sequencing). Data on the neurocognitive measures were missing for 7.5% of the study patients. Because data on the other measures were available for those patients, mean substitution was used to impute their missing composite neurocognitive functioning scores.
The association of employment and obesity, measured by the waist-to-hip ratio, was also explored because weight gain has been identified as a frequent problem with the newer antipsychotic medications. Two site-level measures of the employment environment were also included: 1) the availability of rehabilitation services, as reflected by the proportion of CATIE subjects at each site who reported participation in vocational rehabilitation services, and 2) the unemployment rate in the county in which each site was located, as reported by the Bureau of Labor Statistics for the year in which assessment took place (http://www.bls.gov/lau/home.htm).
Analysis
First, bivariate analysis of variance (ANOVA) and chi-square tests were used to compare the three groups of patients on the potential predictor variables. Paired group comparisons were made by using t tests and chi-square tests. Because of the large number of subjects, an alpha level of 0.01 was set as the required level for statistical significance in these analyses. Tukey’s tests with an alpha criterion of p<0.01 were used for paired comparisons of means.
Next, measures for which significant differences were found in the bivariate analysis were included in a series of four multinomial logistic regression analyses in which competitively and noncompetitively employed patients were compared with patients who were not employed. Because scores on subscales of the PANSS and the Quality of Life Scale were highly correlated, the effects of these scores were examined in separate analyses. The first analysis included the PANSS positive symptom subscale scores. The PANSS negative symptom subscale scores were added in the second analysis, and scores on the five-item Quality of Life Scale intrapsychic functioning scale were added in the third analysis. Because the social activity, instrumental functioning, and object and activities subscales of the Quality of Life Scale, along with the time-utilization item from the intrapsychic functioning subscale, had face-value relationships to employment, only the modified five-item intrapsychic functioning subscale score was included in the model. In addition, because the scores on the neurocognitive subscales were highly correlated, only the composite neurocognitive functioning measure was used in multivariate analyses.
A fourth and final model included the environmental measures reflecting local availability of psychosocial rehabilitation services and the county unemployment rate. The former was measured as the percentage of clients in the CATIE study who reported participation in vocational rehabilitation activities at that site. This item was based on a series of questions concerning service use that asked about participation in psychosocial rehabilitation. Because a strong association would be expected between participation in noncompetitive employment and site-level measures of rehabilitation service availability, the individual-level measure was included in models with the site-level measure to control for individual-level effects. The issue of particular interest here was whether patients were more or less likely to be competitively employed at sites with greater availability of vocational rehabilitation services.
Because patient data were available from 57 sites and the final two variables were site-level measures rather than patient-level variables, generalized estimation equations were used to adjust the standard errors of the regression coefficients for the correlation of observations within sites
(22). However, only continuous or dichotomous dependent variables can be analyzed with generalized estimation equations in SAS (SAS Institute, Cary, N.C). To address this limitation, we first conducted multinomial logistic regression analyses using PROC CATMOD of SAS Version 8.0. These analyses were then replicated in two generalized estimation equations analyses by using SAS PROC GENMOD. In the first generalized estimation equation, competitively employed patients were compared with those who were not employed. In the second, noncompetitively employed patients were compared with those who were not employed. Because the results of the CATMOD and GENMOD analyses were virtually the same (effect sizes were slightly smaller in the generalized estimation equations analysis, but there were no differences in statistically significant items), we present the CATMOD results.
Because none of the symptom measures differentiated competitively employed patients and those who participated in other types of employment activity, a simple logistic regression analysis was used to compare factors that differentiated these groups in the bivariate analyses.
Finally, linear multiple regression models with generalized estimation equations were used to identify correlates of monthly earnings among subjects who were competitively employed. An alpha of 0.05 was used in the multiple regression analyses. Because we designed the current study to generate rather than test hypotheses, p values were used for descriptive rather than hypothesis-testing purposes.
Results
Subjects
The study subjects (N=1,438) had an average age of 40.4 years (SD=11.6), 76% (N=1,086) were male, 35% (N=498) were black, 12% (N=169) were Hispanic, 74% (N=1,070) had completed at least a high school education, 12% (N=166) were married, and 60% (N=856) had never married. Altogether, 14.5% (N=208) reported some competitive employment, 12.6% (N=181) reported other employment activity, and 72.9% (N=1,049) reported no employment activity.
Bivariate Group Comparisons
The results of the bivariate comparisons are shown in Data Supplement 2, which is available with the online version of this article at http://ajp.psychiatryonline.org.
Bivariate comparisons revealed significant differences between the groups conforming to three patterns of interest. First, the instrumental activity and objects and activities subscales of the Quality of Life Scale showed a monotonic pattern in which workers in competitive employment scored higher than those in other kinds of employment, who, in turn, scored higher than those who were not working. This serial pattern is not surprising, given that these two measures include items that, at face value, could be part of an employment situation.
A second pattern in scores on the total Quality of Life Scale and the social relationships and modified intrapsychic functioning subscales of the Quality of Life Scale showed that those in competitive employment scored no higher than those in alternative employment, but both groups scored significantly higher than those who were not employed. Similarly, compared with nonworkers, participants in either type of employment activity had lower schizophrenia symptom scores (PANSS total scores and negative symptom subscale scores), had higher neurocognitive functioning scores on the general scale and on three of the five subscales, and were better educated. In each case, there were no differences between the two working groups, but both groups were better off than the nonworkers.
A third group of measures differentiated those who were competitively employed from one or both of the other two groups. Competitively employed patients 1) were younger than nonworkers, 2) were less likely to be black, and 3) received lower public support payments on average (especially SSD and SSI payments). There were no significant differences between the groups on measures of depression, substance abuse, tardive dyskinesia, akathisia, and extrapyramidal symptoms and no significant difference on the waist-to-hip ratio.
Multivariate Group Comparisons
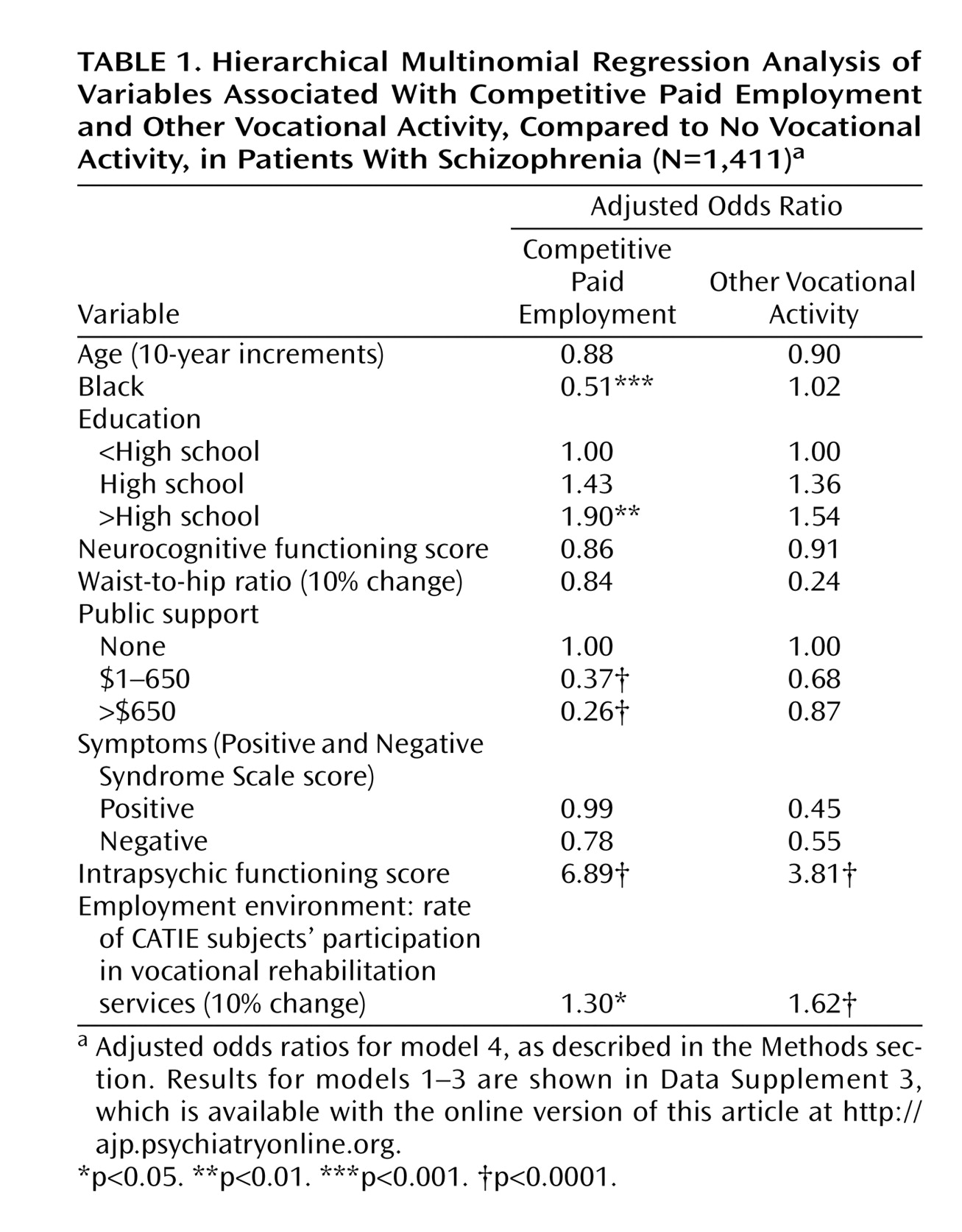
The results for models 1–3 in the multinomial logistic regression analysis are shown in Data Supplement 3, which is available with the online version of this article at http://ajp.psychiatryonline.org. The results for the fourth and final model are shown in
Table 1.
The multivariate analysis largely confirmed the bivariate findings, showing that positive symptoms, negative symptoms, and intrapsychic functioning differentiated participants in both competitive employment and other types of employment from nonworkers. The effect for negative symptoms was significant over and above the effect for positive symptoms, and the effect of intrapsychic functioning was significant over and above the effect of negative symptoms for both types of employment. Neurocognitive functioning, however, had no significant effect over and above symptom measures.
In contrast, the likelihood of competitive employment was lower for blacks and for those receiving disability payments, but no significant relationship was observed between these measures and noncompetitive employment. Blacks were about half as likely to work as whites. Monthly disability payments greater than $650 reduced the likelihood of competitive employment by 73%–74%, and payments of less than $650 reduced the likelihood of such employment by 59%–63%. The effects of race and disability payment measures remained significant and of largely undiminished magnitude even after negative symptoms and intrapsychic functioning were added to positive symptoms in the models. A higher level of education was more robustly associated with competitive than with noncompetitive employment.
Site-level availability of rehabilitation services was associated with individual participation in competitive employment, and especially in noncompetitive employment, after adjustment for all significant individual-level factors.
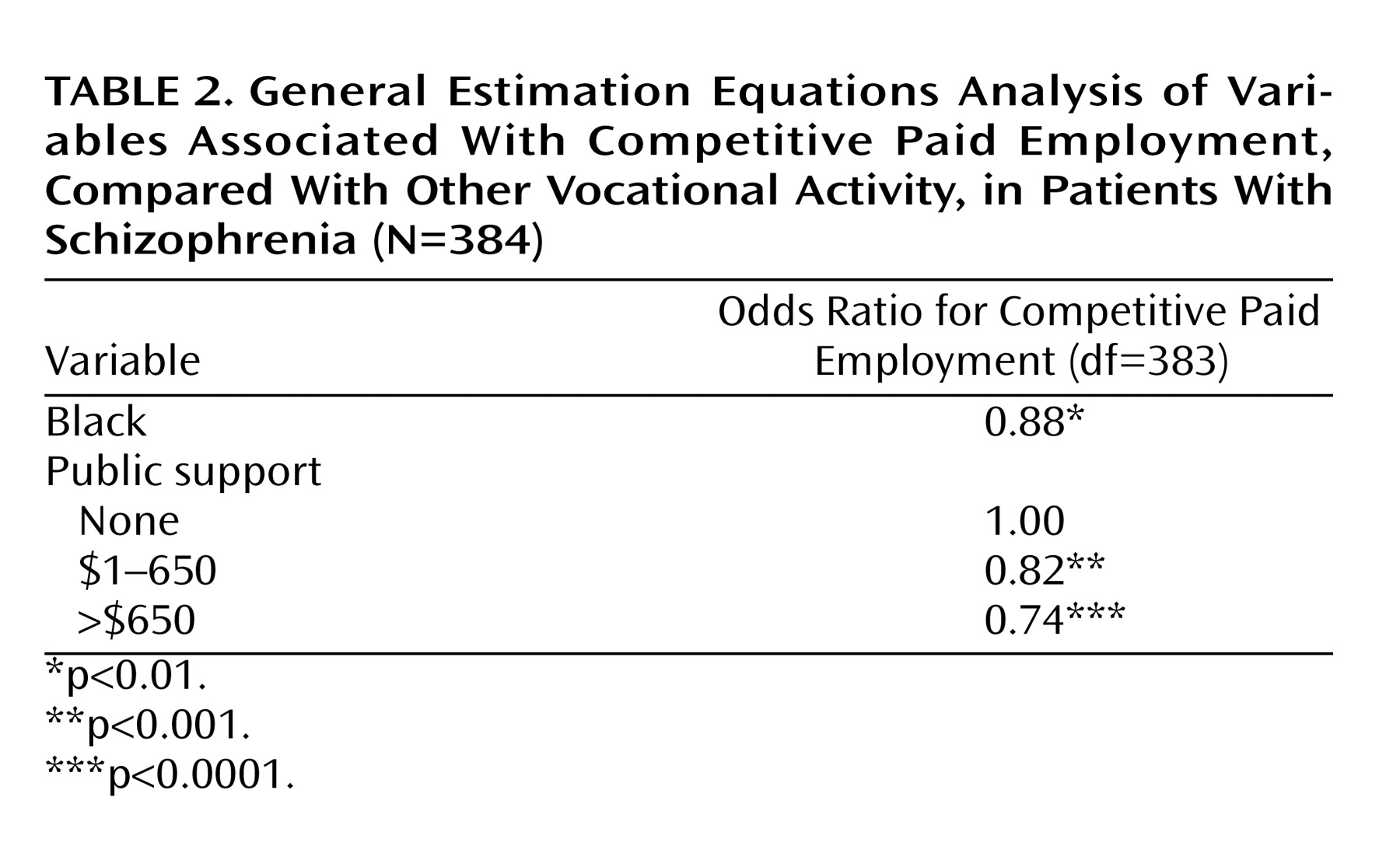
Direct comparison of data for patients in competitive and noncompetitive employment confirmed that blacks and recipients of disability payments were less likely to participate in competitive employment than in noncompetitive employment (
Table 2).
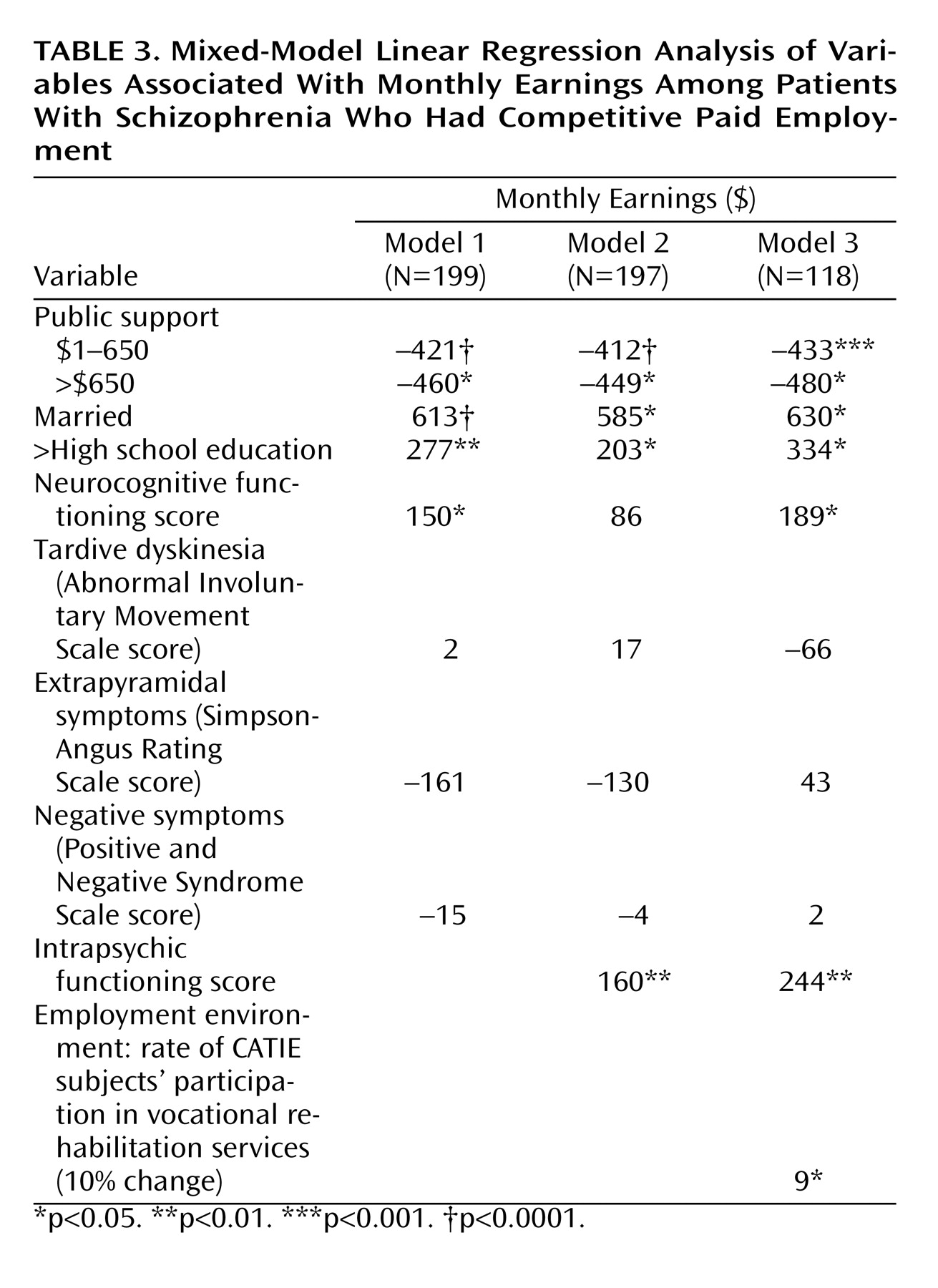
Employment Earnings
Table 3 shows the results of a linear regression analysis of the independent variables that were significantly related to earnings among workers in the bivariate analysis. Because positive symptoms were not significantly related to earnings in the bivariate analysis, this variable was not included in the multivariate analyses. Among those with competitive employment, earnings were lower among patients who received disability payments and were positively associated with being married, with having more than a high school education and better intrapsychic functioning, and with the unemployment rate. Earnings were not significantly related to negative symptoms.
Discussion
This study examined correlates of employment in a large group of more than 1,400 patients who met formal diagnostic criteria for schizophrenia. The relationships between patient characteristics and both competitive employment and other employment activities can be classified into two categories of particular interest. First, several clinical measures, especially measures of psychopathology and both neurocognitive and intrapsychic functioning, differentiated participants in either competitive or noncompetitive employment activities from those who did not work at all but did not differentiate participants in the two types of employment from each other. Educational level was also not significantly different between the two working groups but was higher among workers than among those who did not work, reflecting the adverse consequences of compromises in premorbid achievement, although poor educational attainment might have been related to prodromal deficits that preceded the full onset of schizophrenia. Illness-related factors, if severe enough, seem to block any kind of vocational activity.
In the second category were measures that differentiated patients who were competitively employed from those who either participated in other employment activities or who did not work at all. These measures were more social than clinical in nature. For example, black patients were less likely to be competitively employed than patients in other racial groups, perhaps because of job discrimination in the competitive economy
(23) or internalized attitudes resulting from past experiences of such discrimination. People who received disability payments were also less likely to be competitively employed than were those who did not receive these payments, perhaps because those who received these payments feared the loss of such benefits (and perhaps the loss of health insurance) if they worked at competitive jobs but not if they pursued employment outside the mainstream economy
(1). No differences were found between competitively employed workers and other workers on the more clinically oriented measures of symptoms, neurocognitive functioning, and intrapsychic functioning.
In addition, a proxy measure of the availability of psychosocial rehabilitation services was associated with greater participation in both noncompetitive employment and employment in the competitive economy. This finding is consistent with numerous experimental studies showing that rehabilitation services can promote employment
(1–
4). It would thus appear that although clinical factors are associated with employment in general, being black and receipt of disability payments are more specifically and negatively correlated with participation in competitive employment and that the availability of rehabilitative services is associated with increased involvement in both kinds of employment.
Earnings among employed patients were also strongly negatively associated with receipt of disability payments but positively associated with education, marital status, and better intrapsychic functioning. Thus, a negative association was observed between disability payments, especially payments greater than $650 per month, and both participation in competitive employment and earnings among those who were employed. Although previous studies have demonstrated lower employment rates among public support recipients
(9,
10), no previous study, to our knowledge, has had access to such rich clinical data from a diagnostically homogeneous group. In this study, receipt of disability payments was associated with poorer functioning as assessed with the Quality of Life Scale (r=–0.06, p<0.03) and neurocognitive measures (r=–0.14, p<0.0001) but also with lower PANSS total scores (r=–0.62, p<0.03). In the absence of comprehensive measures of symptoms, neurocognitive functioning, and intrapsychic functioning, it is unclear whether disability payments were themselves a barrier to employment or whether they were merely an indicator of more severe but unmeasured clinical impairment. In the present study, negative relationships between disability payments and competitive employment persisted with minimal reduction in magnitude even after adjustment for multiple measures of symptoms and neurocognitive and intrapsychic functioning. It has been reported in the clinical literature that individuals who receive disability benefits often do not work competitively because they fear a loss of benefits, and perhaps a loss of health insurance, if they work at competitive jobs
(1). Consistent with our findings, it has also been observed that those who do work take care not to earn enough money to jeopardize their benefits
(1).
The findings of this study are also consistent with recent research revealing an unexpected decline in employment among disabled Americans during the 1990s. It was initially expected that activation of the provisions of the Americans With Disabilities Act in 1992 would increase employment opportunities for disabled Americans. In fact, employment declined steadily in this population, especially among younger adults and people with depression
(24), even during the employment boom of the late 1990s when job opportunities were expanding substantially for the nondisabled population. Although several possible explanations for the decline have been considered, the decline in employment among the disabled most closely parallels the sharp increase in the number of SSDI and SSI recipients in the population
(25,
26). This increase, in turn, is thought to reflect the easing of SSDI and SSI disability requirements for mental illness and musculoskeletal disorders (e.g., back pain) and the increase in SSDI and SSI payment levels relative to rates of compensation in low-wage jobs during the 1980s and 1990s
(25,
26).
These data suggest that policy makers face the challenge of preserving employment incentives without jeopardizing the financial safety net required by many people with severe mental illnesses such as schizophrenia, especially because their need for such support may be both long-term and intermittent. Although recent legislation allows SSDI and SSI recipients to continue their Medicaid coverage after returning to work
(26), some fair mechanism should be developed for preserving access to income supports while allowing access to the rewards of employment. A policy that can accomplish these goals and that will also be politically acceptable will, however, be difficult to craft.
This study had several limitations. First it was based on cross-sectional data, and causal inferences cannot be justified. Disability recipients, for example, are likely to be different from other patients, and thus the relationship between disability payments and employment may reflect the confounding effect of differences in the underlying illness that were not measured in this study. Because such potentially confounding factors threaten the validity of all cross-sectional studies, we used statistical methods to adjust for potentially biasing differences. The CATIE study is uniquely suitable for this approach because it includes an exceptionally rich array of measures that can be used for such statistical adjustment. Nevertheless, these finding must be approached cautiously because several alternative interpretations are possible.
Ultimately, experimental studies of both clinical and policy innovations are necessary to identify factors that affect employment among people with schizophrenia
(1–
4). However, because it is not possible to randomly assign patients to receive disability payments, questions about the effect of such payments on employment can be addressed, however imperfectly, only through observational studies such as this one. Additional longitudinal data on changes in employment status and its relationship to a variety of factors will be available when the CATIE study is completed, and these data may allow further examination of these issues.
Second, although we interpreted our data as showing that negative symptoms and intrapsychic functioning are predictors of employment, the observed associations may also have reflected a reverse causality; that is, patients who were working may have reported fewer negative symptoms and better intrapsychic functioning specifically because they were working. This causal ambiguity is less likely to affect observed relationships with positive symptoms or other measures.
Third, our measure of the availability of rehabilitation services in each community was based on simple participation rates among the CATIE subjects, and we do not know if this measure reflects the availability of rehabilitation services in the wider community or whether those services followed evidence-based models
(1–
4). The observed relationship between participation in rehabilitation services and employment outcomes, although consistent with experimental research findings
(1–
4), should also be interpreted with caution.
Finally, although the CATIE investigators sought to engage a broadly representative set of sites, the generalizability of the findings is unknown. However, it is noteworthy that the average PANSS score among the CATIE subjects (mean=75.7, SD=17.5) was substantially lower than the average baseline total PANSS score in an international collaborative trial of olanzapine and haloperidol
(27) (mean=86.4, SD=15.4) or in a recent U.S. Department of Veterans Affairs trial that compared the same medications
(28) (mean=90.8, SD=19.5). Because neither the CATIE study nor either of these trials applied any entry criteria pertaining to refractory illness, it seems clear that the subjects included in the analyses reported here could not be characterized as having illnesses that were refractory to treatment.