Depression is a common and disabling mental disorder in older persons
(1,
2), who constitute a population that is of growing importance to general as well as geriatric psychiatrists
(2) . It has long been recognized that late-life depression may be associated with impairments in various domains of cognitive functioning
(3 –
5) . In recent years, growing attention has been given to the clinical importance of the relationship between depression and executive functioning—cognitive domains such as planning, organizing, sequencing, and initiation/perseveration
(5 –
9), although not all studies have confirmed the specificity of these associations
(10,
11) .
An understanding of the nature of the relationships between depression and cognition may yield important insights regarding the pathogenesis of depression and opportunities for more specifically targeted interventions. Several possibilities might underlie any such association. Cognitive dysfunction, presumably due to cerebral dysfunction, may contribute to the occurrence of depression, either reflecting a common underlying pathogenesis, such as small-vessel cerebrovascular disease
(12), or as mediated by the psychosocial consequences of diminished cognitive performance. Alternatively, depressive symptoms may precede worsening cognitive deficits, which might reflect depression’s role as an early marker of brain disease or as a mental and physiological state that taxes cognitive performance over time.
Thus far, evidence supports the first hypothesis—that cognitive, especially executive, dysfunction plays an important role in the occurrence of geriatric depression
(5,
13) . Likely mechanisms that have been suggested include disruption of striatal-pallidal-thalamo-cortical pathways
(14) and prefrontal lobe hypometabolism
(15) . Conversely, many studies, but not all, based mainly on community samples have provided support for the hypothesis that depressive symptoms increase the likelihood of cognitive deficit, especially memory deficits, which in the long run may lead to dementia
(16 –
18) .
To our knowledge no prior study has examined the relative strengths of the potentially reciprocal relationships between depression and executive dysfunction over time in older persons. We did so using data collected from repeated measures from a large multiwave observational study. We focused on older primary care patients, because most seniors suffering clinically significant depressive symptoms do not present to mental health specialists but do see primary care providers
(19) . Moreover, primary care patients have a broad range of depressive symptoms and syndromes, including minor as well as major depression
(20) . Specifically, we tested the hypotheses that 1) depressive disorders and symptoms predict subsequent decline in selected components of executive functioning, and 2) executive dysfunction predicts subsequent depressive outcomes. Given prior evidence that otherwise clinically occult cerebrovascular disease might underlie both depressive and cognitive symptoms in later life
(12,
21), we also tested the hypothesis that cerebrovascular risk factors were associated with both depressive and executive function outcomes in this cohort and explored whether any association of cerebrovascular risk factors with either outcome domain was mediated by its association with the other.
Method
Recruitment
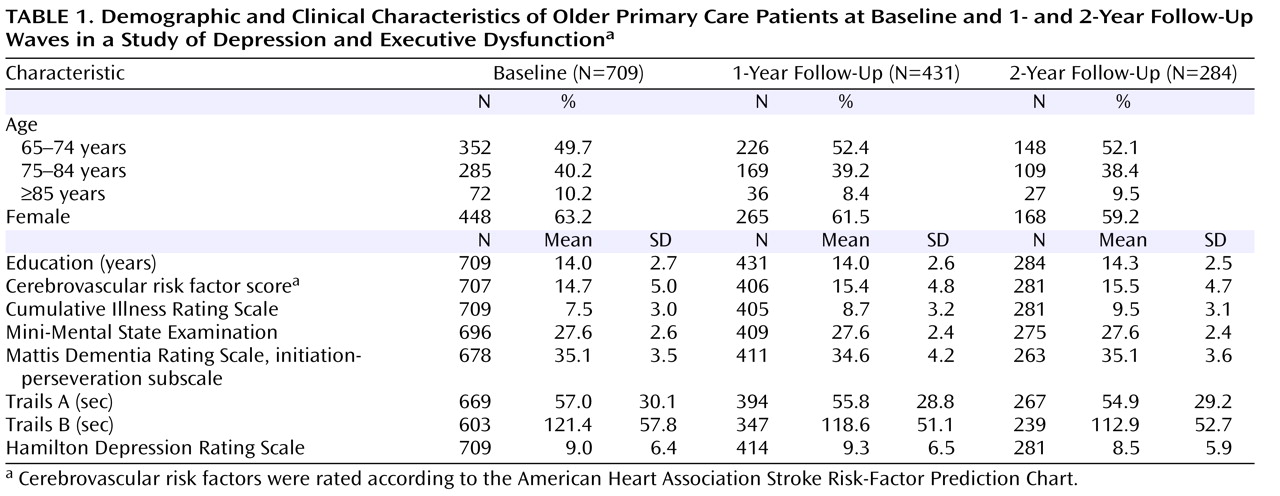
Participants were recruited from private practices and university-affiliated clinics in general internal medicine, geriatrics, and family medicine in Monroe County, New York. The study attempted to recruit all patients age 65 years and older who presented for care on selected days and were capable of giving informed consent. After a complete description of the study was presented, written informed consent was obtained using procedures approved by the University of Rochester Research Subjects Review Board.
Participants underwent semistructured interviews administered by trained raters in the subjects’ homes or in research offices at the University of Rochester Medical Center. Raters also reviewed each patient’s primary care medical chart, extracting all recorded information about mood and cognitive symptoms, disorders, or treatments as well as active and past medical problems and current medications. The raters’ patient interviews included assessments of cognition, functional status, and psychopathology, the latter including the Structured Clinical Interview for DSM-IV (SCID)
(22) . Interviews and chart reviews were conducted at study intake and again at 1 year and 2 years, and these assessments were supplemented by interim structured telephone interviews focusing on the nine SCID depressive symptoms every 6 months.
Measures
Depression diagnoses at each time point were assigned at consensus conferences of investigators and raters, using SCID criteria and information obtained from the patient interview and the medical chart review. Depression diagnoses were coded ordinally as follows: 1) current or partially remitted major depression; 2) current or partially remitted minor depression (based on proposed criteria in Appendix B of DSM-IV); or 3) no depression (all others). Depressive symptom severity was assessed with the 24-item Hamilton Depression Rating Scale (HAM-D)
(23) . In our research group, interrater reliability on the HAM-D has been high, with an intraclass correlation coefficient of 0.93 (based on six raters and five subjects) and kappa coefficients for the diagnoses of mood disorders ranging from 0.66 to 0.86 (p=0.0003, based on six raters and three subjects).
Medical measures were completed by a physician-investigator (J.M.L.) based on data obtained from the raters’ patient interviews and from the medical chart reviews. The cumulative severity of cerebrovascular risk factors was rated according to the American Heart Association Stroke Risk-Factor Prediction Chart
(24), which creates a weighted sum from the following risk factors (based on their predictive power for stroke): systolic blood pressure, antihypertensive therapy, cardiovascular disease, diabetes mellitus, cigarette smoking, atrial fibrillation, and left ventricular hypertrophy. To determine the specificity of any associations with cerebrovascular risk factors, overall medical illness burden was additionally covaried, as measured by the Cumulative Illness Rating Scale
(25), a reliable and validated scale that assesses the clinical severity of pathology in each organ system. Medical measures were completed by raters blind to the SCID interview data, although not blind to any mention of depression in the medical records.
The study raters were trained to administer the cognitive measures by procedures developed under the supervision of a clinical neuropsychologist. Selected components of executive functioning were measured using the initiation-perseveration subscale of the Mattis Dementia Rating Scale
(26) and Trail Making Tests A and B
(27) . The initiation-perseveration subscale consists of verbal, physical, and graphomotor tasks, such as category fluency (naming items in a supermarket), alternating hand movements, and copying an alternating pattern, with higher scores indicating better performance. The initiation-perseveration subscale was chosen partly to allow comparability to prior studies
(7) . Trail Making Tests A and B are widely used and validated neuropsychological tests involving timed paper-and-pencil tasks of numeric (Trails A) and alphanumeric (Trails B) sequencing. Trails A assesses sustained attention, sequencing, and information processing/motor speed. Trails B additionally measures mental set shifting and response inhibition, important components of executive functioning. Trails A and B were analyzed on the basis of completion time in seconds, with greater time indicating poorer functioning; per usual neuropsychological practice, analyses included only those participants who completed Trails A or B within 300 sec (
28, p. 381). Analyses also examined Trails B minus Trails A time (D Trails), which has been recommended as a “purer” measure of executive functioning that, in effect, removes processing/motor speed and other Trails A components from the Trails B time (
28, p. 382). To assess whether associations were specific to the executive functioning domains tapped by the Mattis initiation-perseveration subscale and D Trails or reflected more global cognitive impairment, overall cognitive status was assessed with the Mini-Mental State Examination (MMSE)
(29) .
Our intent was to combine relatively intensive clinical research assessments with an essentially epidemiological approach to studying a broad, heterogeneous group; in this context, it was important not to constrain the cognitive variability of interest by excluding patients with dementia. At the same time, we recognized that the results might differ or be easier to interpret if patients with dementia were excluded. Therefore, all study analyses involving cognition were conducted twice: once including all participants and once excluding the 31 subjects with a diagnosis of dementia. The diagnosis of dementia was based on conservative clinical application of DSM-IV criteria by an experienced geriatric psychiatrist (J.M.L.) using all available information, including participants’ performance on the cognitive measures (including details of subitem performance), qualitative observations provided by the research raters, and history and examinations recorded in patients’ medical records. The results did not differ after participants with dementia were excluded, so in the Results section we report findings from the entire study group.
Statistical Analysis
Analyses were conducted using SAS (version 9.1, Cary, NC). Two-tailed p values were computed, with the alpha level conservatively set at 0.01 because of the number of analyses performed. The chi-square test for categorical variables and the nonparametric Wilcoxon test for continuous variables were used for analyses of baseline variables. Longitudinal data typically have substantial correlation between measurements of the same participant over time; to obtain correct standard errors for regression models, statistical modeling techniques must account for such autocorrelations. In this study we used generalized estimating equations (GEE), a popular modeling approach for longitudinal data that accounts for within-subject correlations in the dependent variables and provides robust inferences
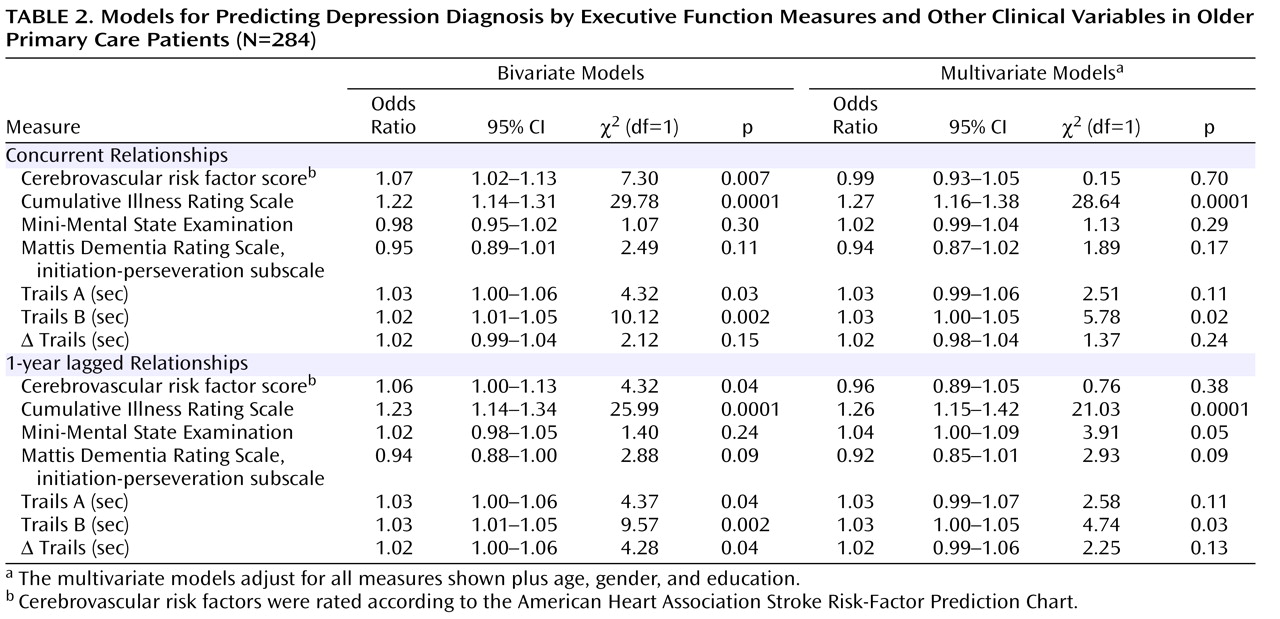
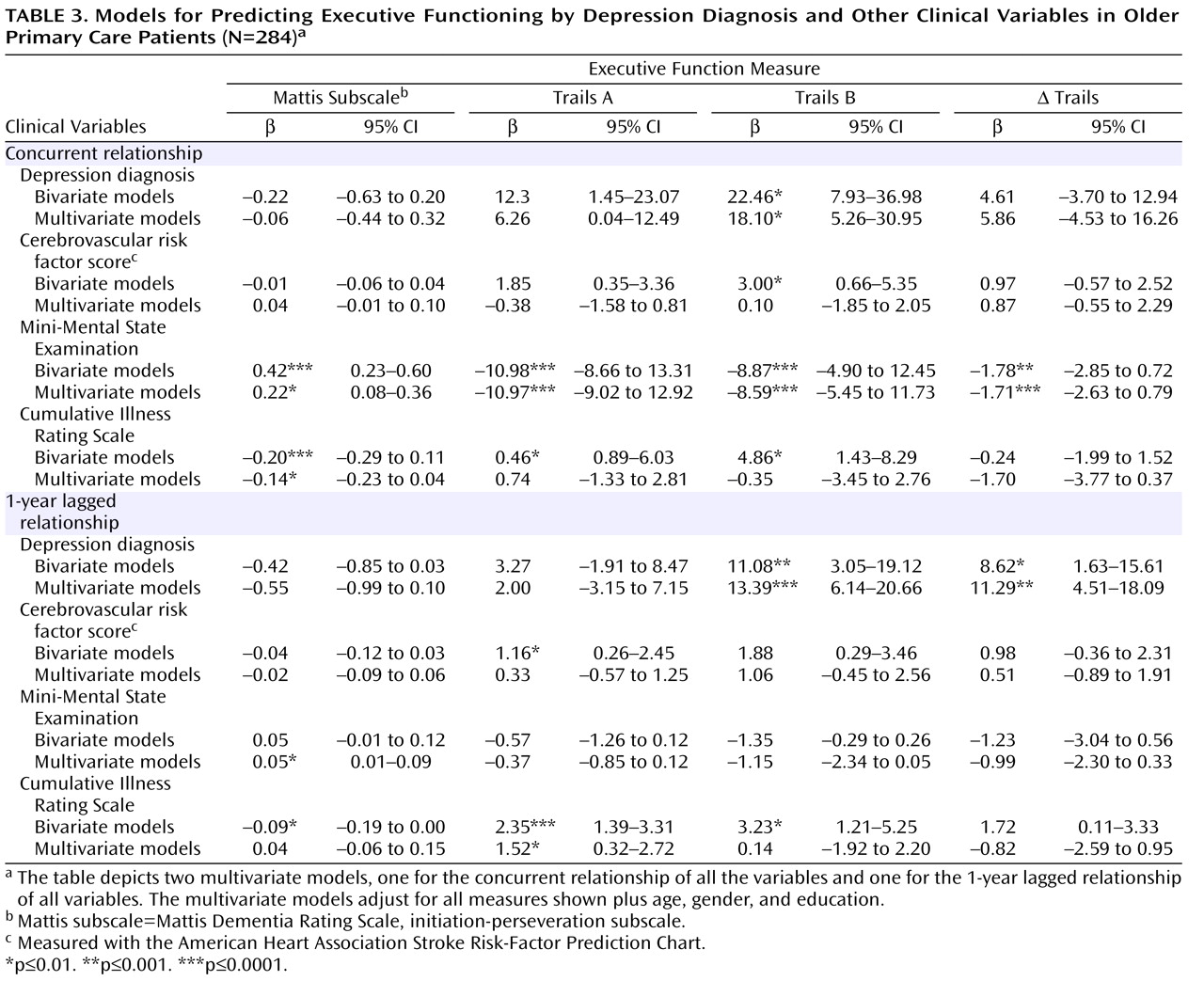
(30) . Specifically, we used depression diagnosis as an outcome variable predicted by the four cognitive measures—the Mattis initiation-perseveration subscale, Trails A, Trails B, and D Trails—either individually (simple regression model) or simultaneously (multiple regression model), adjusting for covariates (age, gender, education, MMSE score, Cumulative Illness Rating Scale score, and cerebrovascular risk factor score). Antidepressant treatment was not covaried, as it is not independently associated with depression outcome in naturalistically followed primary care cohorts, probably because of confounding by indication
(31) . Multinomial logit link was used for analyses with three-level depression diagnosis (major depression, minor depression, no depression) as the outcome variable
(32) . Both concurrent and 1-year lagged depression outcomes were modeled. Concurrent analyses reflect cross-sectional associations using data pooled from repeated measures at all time points. Lagged analyses were used to predict depression 1 year after measurement of executive functioning and also to predict executive functioning 1 year after the diagnosis of depression; the latter used a linear link for the modeling. Lagged analyses included participants who were assessed at intake and at least one other time point during the follow-up period.
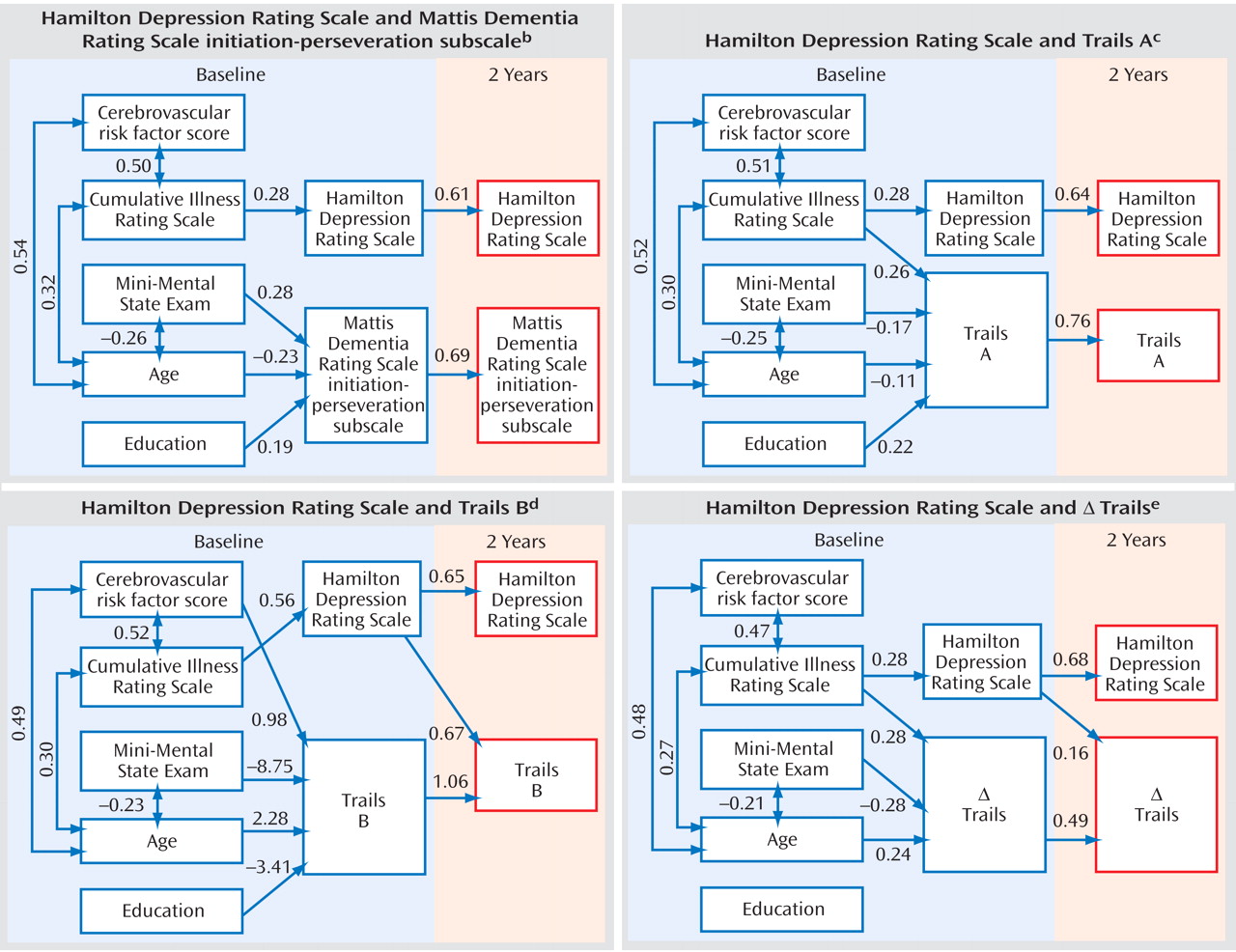
We used path analysis to test competing dynamic models involving depressive symptom severity (as measured by the HAM-D) and cognition as both predictors and outcomes. These analyses used SAS’s CALIS procedure, employing the maximum likelihood method to estimate statistical parameters on the variance-covariance matrix for structural equations models (SEM). The chi-square statistic was used to test the null hypotheses and goodness of fit. Unstandardized path coefficients that reached statistical significance (p<0.05) are presented in path diagrams. The path diagrams present only baseline and 2-year data, since parallel analyses using baseline and 1-year data yielded similar findings. Because no disparity was noted for separate analyses of men and women, we report the results for both genders combined.
Sensitivity analyses tested the robustness of estimated parameters by repeating the primary analyses and excluding participants who were depressed at baseline and whose depression onset was before age 65, in light of suggestions that small-vessel cerebrovascular disease or executive dysfunction may be most salient in depression with a later onset age. In addition, we reran the GEE modeling analyses by substituting depression diagnoses with HAM-D score and with the HAM-D rescored to exclude neurovegetative symptoms (decreased work and activities, diminished libido, gastrointestinal symptoms, weight loss, insomnia, psychomotor retardation, agitation, diurnal variation, and other somatic symptoms). These results did not substantively differ from those based on the entire sample and so are not reported in detail here.
Discussion
Our hypothesis of a dynamic bidirectional relationship between geriatric depression and executive dysfunction was not substantiated, as executive dysfunction did not independently predict subsequent depression diagnosis or HAM-D score. However, antecedent depression was a robust independent predictor of the executive functioning domains captured in Trails B and D Trails (i.e., set shifting), although not for processing speed (Trails A) and category fluency/perseveration (Mattis initiation-perseveration subscale score). Consistent with many, but not all, previous studies
(6,
13,
35), overall medical burden, rather than cerebrovascular risk factors, was an independent predictor of subsequent depression as well as executive dysfunction.
Limitations of this study need to be considered. We tested our hypotheses using interim data from an ongoing prospective study. The relationships of interest may play out differently over a longer period. Participants in our study were predominantly white, were relatively well educated (although educational levels varied considerably), and had sufficient cognitive abilities and English communication skills to consent to the study and complete the cognitive measures. While the study group largely reflects the population of older persons in Monroe County, New York, who present to primary care practices, our results may not generalize to other or more impaired populations. An additional source of sample bias was introduced by study withdrawals and deaths; those without 2-year follow-up data were more depressed and had a greater medical burden at baseline, although presumably their inclusion would have reduced our ability to detect the relationships of interest. We used a limited neuropsychological test battery to improve the tolerability of the assessments and thus the generalizability of our findings in broad primary care groups. Because limited batteries are more likely to yield chance findings than broader batteries with more redundant assessments of the domains of interest, caution must be exercised in drawing conclusions from them. Lastly, executive functioning is a broad construct with multiple components, of which only initiation-perseveration and mental set shifting were captured by the measures used in this study. Also, the tests we used necessarily depend on other cognitive domains, including language, visuospatial skills, and processing/motor speed; the latter may be particularly important, given the primacy of processing speed’s association with depression in correlational studies of depressed patients in psychiatric settings
(9,
11) . At the same time, it should be recognized that we employed D Trails time to help increase the specificity of the Trails findings for set shifting.
Despite these limitations, this study drew on a primary care cohort that is, to our knowledge, unique in the extent and rigor of the study assessments it has undergone. Our findings have important implications for understanding the potential mechanisms that underlie the associations of depression and executive functioning. It has been suggested that executive dysfunction may be merely an epiphenomenon of depression
(36), that is, that depressed subjects’ poor performance on neuropsychological tests is a reflection of their neurovegetative symptoms of depression, decreased motivation, and lack of attention. However, while findings from the concurrent models are consistent with such prior work, this perspective cannot fully account for our longitudinal finding that depression independently predicts subsequent cognitive impairment in some domains. Moreover, reanalyzing the data by excluding the neurovegetative symptoms did not change the results.
Our data indicate that depression can be a harbinger of subsequent cognitive impairment, presumably on the basis of structural brain disease. This would seem to be consistent with the postulated course of the “depression-executive dysfunction syndrome,” potentially reflecting frontostriatal abnormalities caused by cerebrovascular disease or other aging-associated conditions
(8,
11) . Indeed, depression might interact with white matter disease to produce executive dysfunction, with depression representing a “vulnerability or necessary cofactor”
(37) . However, our data suggest that the depression-executive dysfunction syndrome model may need to be refined, as depression was associated with the set-shifting component of executive function but not the domains assessed by the Mattis initiation-perseveration subscale.
In this study, as in some prior work
(38), cerebrovascular risk factors were not independently associated with either depression or executive functioning outcomes, suggesting that the role of otherwise clinically occult cerebrovascular disease in depression may be more important in specific patient subgroups than in a broad primary care population, the latter likely including depressive conditions reflecting a “final common pathway” for heterogeneous pathogeneses. Such pathogeneses likely include prominent roles for a wide range of psychosocial factors as precipitants or moderators of depression outcomes
(39) .
To further elucidate such mechanisms, future research should delineate the course of broadly sampled patient groups with co-occurring depression and executive dysfunction compared with other patients with either depression or executive dysfunction alone, or neither. Such representative, population-based approaches can usefully complement functional neuroimaging or other approaches that more directly examine frontostriatal activity, typically taken from more highly selective, smaller clinical patient samples. Examination of these issues across a broader age range also may prove instructive, as it remains unclear whether the relevant pathogenic mechanisms are qualitatively or quantitatively distinct in later life. Clinicians should be aware that older depressed patients, already at risk of greater functional disability
(6), are at further risk of disability related to subsequent decline in at least some aspects of executive functioning
(40) and possibly also to broader cognitive deterioration
(16 –
18) . It remains to be seen whether better treatment of depression with somatic therapies, established depression-specific psychotherapies, or innovative psychosocial approaches (which might target selected components of cognitive functioning) can improve outcomes by reducing the risk of subsequent cognitive decline.