In the most recent meta-analyses of manualized brief dynamic psychotherapy
(1,
2), the authors concluded that this treatment modality is effective for a range of common mental disorders, but the evidence for long-term effects is limited, and additional research is needed to identify the active treatment components.
Transference interpretation is generally assumed to be one of the active treatment components for long-term changes in psychoanalytically oriented psychotherapy. Influential theorists maintain that the ongoing interaction between patient and psychotherapist is heavily influenced by the patient’s past relationships and affective experiences. A focus on the conflicts and themes that arise in the therapeutic relationship will therefore have immediate affective resonance and illuminate the true nature of problems in the patient’s relationships outside of therapy. Transference interpretation may thereby bring about long-term stable changes
(3 –
6) . A different perspective is that too much use of transference interpretation, or its application too early, may make patients inordinately anxious. Only patients with greater psychological resources and more mature relationships are able to benefit from transference interpretations in brief psychotherapy
(7,
8) . The alternative approach is to focus on the patient’s relationships outside of therapy and to interpret patterns, conflicts, and fantasies in those contexts
(9,
10) .
To our knowledge, this study is the first experimental investigation designed to measure long-term effects of transference interpretations in brief dynamic psychotherapy. We randomly assigned 100 patients to brief dynamic psychotherapy with or without transference interpretations. Our main hypothesis was that the transference group would have a more favorable course over the entire study period (4 years) than would the comparison group, as reflected in scores on the Psychodynamic Functioning Scales
(12) and the Inventory of Interpersonal Problems—Circumplex Version
(13) . Our second hypothesis was that suitable patients
(7,
8) —patients with a history of mature object relations and/or lacking personality disorders—might benefit more from therapy with transference interpretations than from therapy without. We have previously reported, however, that patients with a history of less mature object relations unexpectedly benefited more from therapy with transference interpretations than from therapy without during the 1-year treatment period
(14) .
Method
Participants
Patients were referred to the study by primary care physicians, private specialist practices, and public outpatient departments. These patients sought psychotherapy for depressive disorders, anxiety disorders, personality disorders, and interpersonal problems not caused by a mental disorder. The study therapists assessed referred patients for eligibility. Patients with psychosis, bipolar illness, organic mental disorder, substance abuse, and long-term inability to work were excluded. Written informed consent was obtained from each participant.
Treatment Conditions and Therapists
The Regional Ethics Committee for health region 1 in Norway approved the study protocol. Patients were consecutively randomized to two groups after completion of pretreatment ratings. Only the patients’ therapist learned the result of the random assignment procedure. The random assignment code was kept on a separate computer, which belonged to our research assistant. The other clinicians remained blind to the patients’ treatment group. Fifty-two patients were assigned to dynamic psychotherapy with low to moderate use of transference interpretations (transference group). Forty-eight patients were assigned to dynamic psychotherapy of the same kind but without transference interpretations (comparison group). The patients were not informed about which technique was studied or the study hypotheses.
Patients were assigned to one of seven therapists based on availability. The clinical research team consisted of six psychiatrists and one clinical psychologist, all of whom had 10–25 years of experience in practicing psychodynamic psychotherapy. In the pilot phase of the study, the therapists were trained for up to 4 years to enable them to provide treatment with a moderate frequency of transference interpretations (one to three per session) and treatment without such interpretations with equal ease and mastery. Each therapist treated 10–17 patients in the main study. All the therapists treated patients in both groups. Since the therapists were not blind to their patients’ group assignment and also served as clinical evaluators of other patients, no therapist ratings of their own patients were included in any of the statistical analyses.
The patients were offered 45-minute sessions weekly for a year. All sessions were audiotaped. A treatment manual (in Norwegian) was used
(15) . For the transference group, the following specific techniques were prescribed: 1) the therapist was to address transactions in the patient-therapist relationship; 2) the therapist was to encourage exploration of thoughts and feelings about the therapy and therapist, including repercussions to the transference by high therapist activity; 3) the therapist was to encourage patients to discuss how they believed the therapist might feel or think about them; 4) the therapist was to include himself explicitly in interpretive linking of dynamic elements (conflicts), direct manifestations of transference, and allusions to the transference; and 5) the therapist was to interpret repetitive interpersonal patterns (including genetic interpretations) and link these patterns to transactions between the patient and the therapist. In the comparison group, these techniques were proscribed. Instead, the therapist consistently used material about interpersonal relationships outside of therapy as the basis for similar interventions (extratransference interpretations), without any linking to the interaction between the patient and the therapist. Both treatments were mainly exploratory in nature. Patients in both treatment groups were encouraged to explore sensitive topics, but the therapist abstained from giving advice or reassurance.
Assessments
Before the randomization, each patient had a 2-hour psychodynamic interview, modified from Sifneos
(8) and Malan
(16), with an independent evaluator. The interview was audiotaped, and several other clinicians listened to the interview. At least three clinicians rated the interview using the Quality of Object Relations Scale
(17) and the Psychodynamic Functioning Scales
(12) . In addition, the patients completed a number of self-reports, including the Inventory of Interpersonal Problems—Circumplex Version
(13) . No structured interview was used in this study to determine axis I diagnoses. These diagnoses were based on the clinical history and assessment of background variables by the patient’s therapist. Diagnoses according to DSM-III-R criteria were discussed before randomization until consensus was reached. Axis II diagnoses were determined before the start of therapy by the patient’s therapist, using the Structured Clinical Interview for DSM-III-R (SCID-II;
18 ); all therapists had prior training in using SCID-II.
Outcome Measures
The Psychodynamic Functioning Scales, which were developed in the pilot phase of this study, comprise six scales in the same format as the Global Assessment of Functioning scale that measure psychological functioning over the previous 3 months. The six scales are as follows: quality of family relationships; quality of friendships; quality of romantic/sexual relationships; tolerance for affects; insight; and problem solving capacity. Aspects of content validity, internal domain construct validity, interrater reliability, discriminant validity from symptom measures, and sensitivity for change in brief dynamic therapy have been established
(11,
12,
19,
20) . We used three clinical raters, blind to treatment group, who made evaluations at baseline and again 1 year, 2 years, and 4 years after the start of therapy. The interrater reliability estimates (intraclass correlation coefficient) for average scores used in this study were about 0.90 for the Psychodynamic Functioning Scales. All follow-up assessments were completed by December 2005.
The total mean score on the Inventory of Interpersonal Problems—Circumplex Version
(13) was used to assess patients’ self-reported interpersonal problems at baseline, midtreatment, end of treatment, 1-year follow-up, and 3-year follow-up. In all evaluations, patients rated 24 life events on a scale from –3 (extremely negative) to +3 (extremely positive)
(21) . Additional treatment, such as contact with mental health professionals, psychotherapy, psychopharmacological treatment, and sick leave, was recorded.
Moderators
Two patient characteristics were chosen a priori as possible moderators of treatment effects
(22) : rating on the Quality of Object Relations Scale (QOR; P. Høglend, unpublished 1994 manual) and presence of a personality disorder. The QOR measures lifelong tendency to establish certain kinds of relationships with others, from mature to primitive, using three 8-point scales
(14) . The predetermined cutoff score for differentiating high versus low QOR scores was 5.00. QOR scores above the cutoff indicate that recent relationships may be difficult but that there is evidence for at least one mature relationship in the patient’s history. QOR scores below the cutoff indicate a history of less gratifying relationships characterized by need for dependency or overcontrol. The intraclass correlation coefficient for the average QOR scores of three raters was 0.84.
Statistical Analysis
Standard power calculation (endpoint analysis) indicated that a moderate effect size of 0.55 could be detected for an alpha threshold of 0.05 with a power of 0.80. An alpha threshold of 0.10 was selected for the moderator analyses and the subsample analyses in order to balance the risk of type II errors. One outlier in the transference group was deleted from analyses of the longitudinal data, as it became clear during treatment that this patient abused sedatives and painkillers. Longitudinal analyses were performed on a sample of 99 patients. We used linear mixed models in SPSS, version 12.0
(23), to analyze longitudinal data. A randomly distributed intercept and slope were fitted for each patient. Improvement over time was curvilinear. The highest rate of improvement was during therapy, with diminishing returns over time. Time was coded 1, 2, 3, 5, and 9, with one step for each half-year, and transformed to a natural logarithm. Log transformation of time fit the data discernibly better than did a linear time slope (change in –2 log likelihood). Intercept and time were treated as both random and fixed effects, and treatment group (coded 1 or 0) was treated as a fixed effect. The fixed effects in the main group analyses were intercept, time, and time by treatment. The two-way interaction term tests treatment effects. The fixed effects in the moderator analyses were intercept, time, moderator, time by treatment, and time by treatment by moderator. We assumed that treatment group means were equal at baseline, by design
(24) . The QOR was centered at the average level in the subsample with high QOR scores and at the average level in the subsample with low QOR scores. In this way the two-way interaction term in the moderator analyses can be interpreted as treatment effects for the typical patient within each of the two subsamples. The three-way interaction term tests changes in the treatment effect with changes in the moderator.
Results
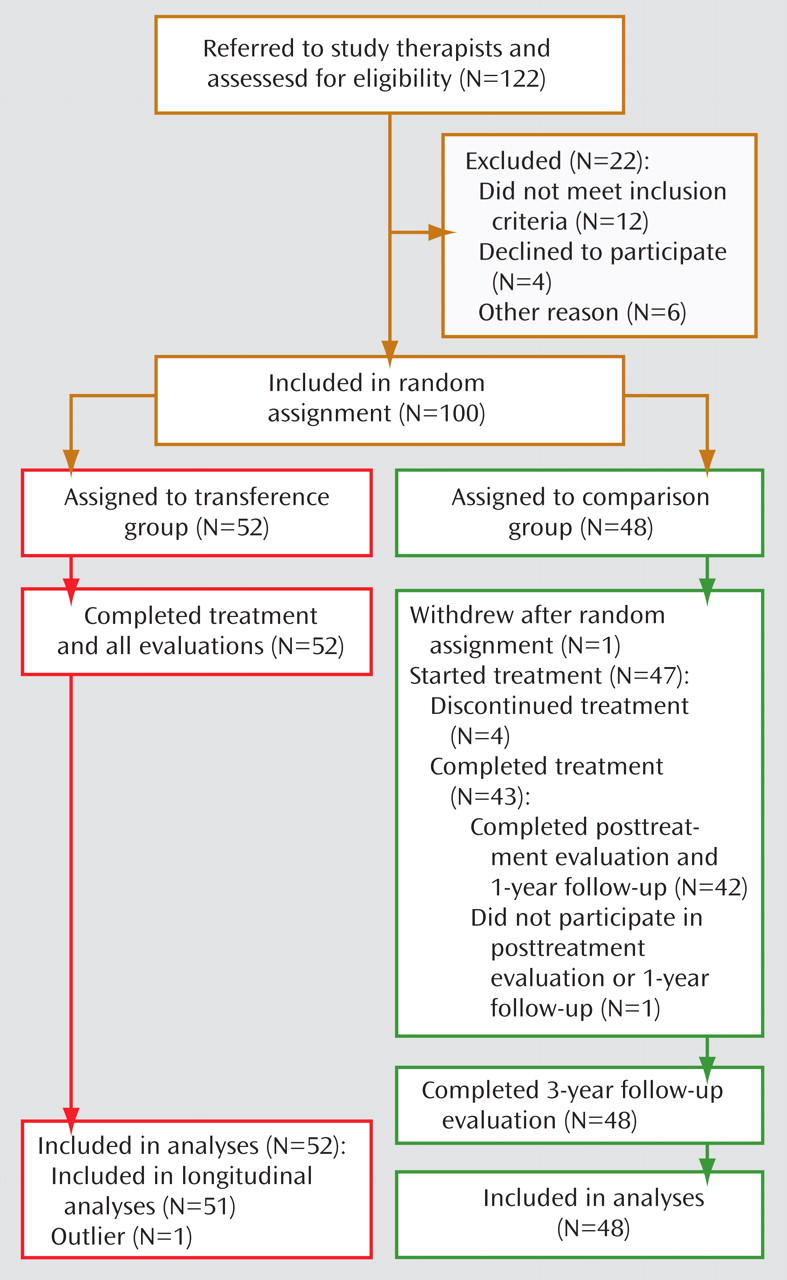
The flow of patients through the study is shown in
Figure 1 . One patient assigned to the comparison group withdrew from the study after randomization. Four other patients, also in the comparison group, dropped out of therapy before session 15.
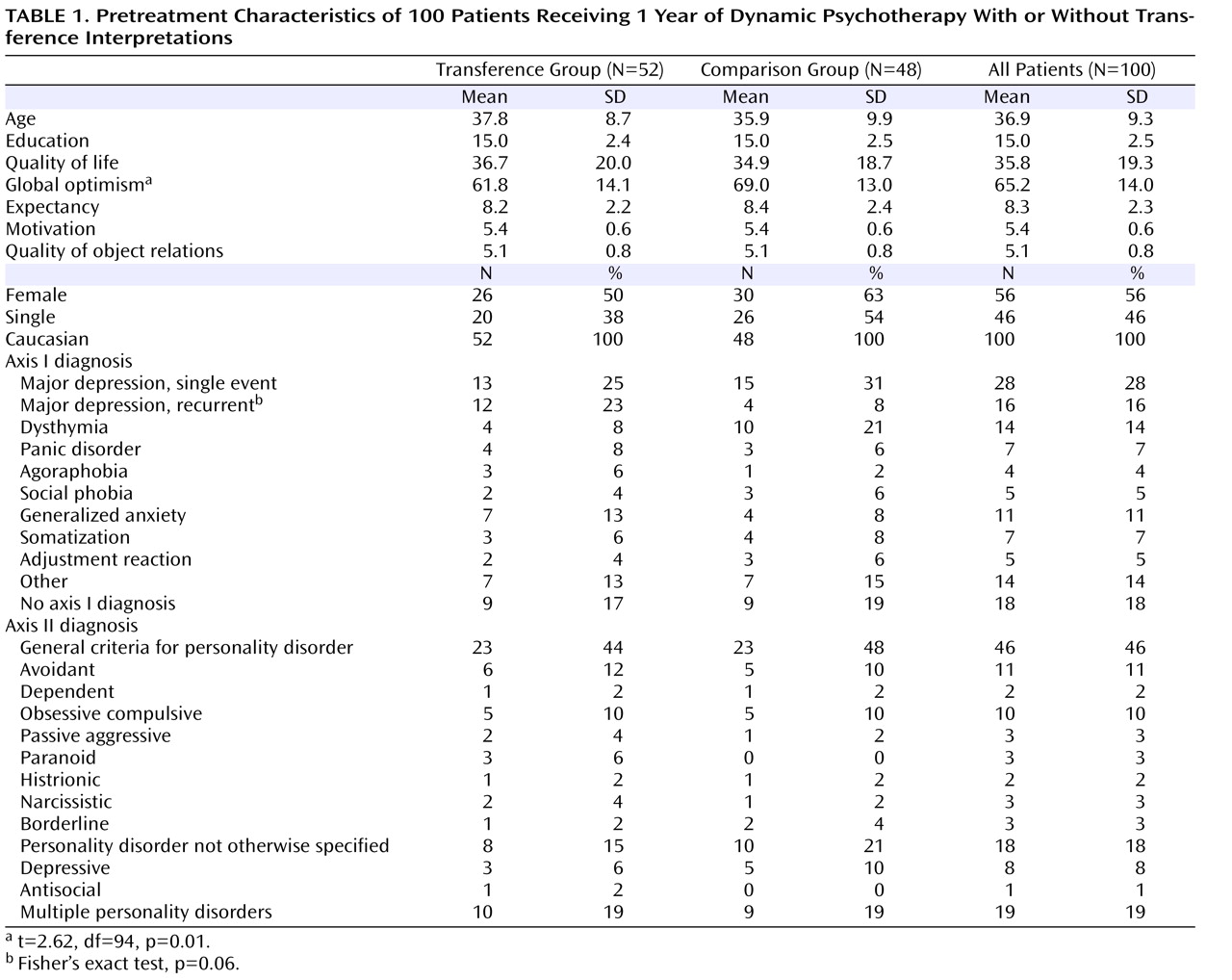
Patient Characteristics at Baseline
Table 1 summarizes the patients’ baseline clinical and demographic characteristics. No significant differences were observed between the transference group and the comparison group on the baseline variables, except that patients in the comparison group rated themselves as more optimistic.
Therapist Effects
To detect possible therapist effects, we performed several linear mixed-model analyses with time, time by treatment, therapist, and time by treatment by therapist as fixed effects. We detected no differences in effectiveness between therapists. However, it should be noted that this study did not have the power to detect small to moderate therapist effects.
Treatment Fidelity
The mean treatment length, with dropouts excluded, was 34 sessions (SD=6.1) for the transference group and 33 sessions (SD=6.6) for the comparison group. A manual for process ratings of audiotaped sessions included the therapist performance scales: the General Interpersonal Skill scale, the Interpretive scale, and the Supportive Technique Scale
(25) as well as the Specific Transference Technique Scales (P. Høglend, unpublished 1995 manual). All items in these instruments use a 5-point Likert scale ranging from 0 (not at all) to 4 (very much). On average, four or five full sessions of each therapy (452 sessions) were rated by three clinicians who were blind to the group to which the patient belonged. With two raters per session, interrater reliability coefficients were generally high (range=0.70 to 0.97) for all the process scales
(26) . The use of specific transference techniques (five items) differed significantly between the treatment groups. The average score was 1. 7 (SD=0.7) in the transference group, indicating moderate use, and 0.1 (SD=0.2) in the comparison group, indicating nearly no use at all (t=14.8, df=58.2, p<0.0005). Some transactions in the patient-therapist relationship also needed to be addressed in the comparison group during the initial sessions and during the termination phase. Analysis of interpersonal relationships outside of therapy (extratransference) (five items) was given somewhat more space and emphasis in the comparison group. We found no group differences in the scores on the General Interpersonal Skill scale (eight items) or the Supportive Technique Scale (seven items).
Before all follow-up evaluations were completed, two sessions from each of 50 patients had been rated by three clinicians with regard to treatment fidelity. The raters may have guessed from the content which group the patient belonged to. We believe it is unlikely that the raters could remember the treatment group from listening to anonymous audiotapes months or even years before the follow-up evaluations. However, we cannot rule out the possibility that blinding may have been compromised for some patients.
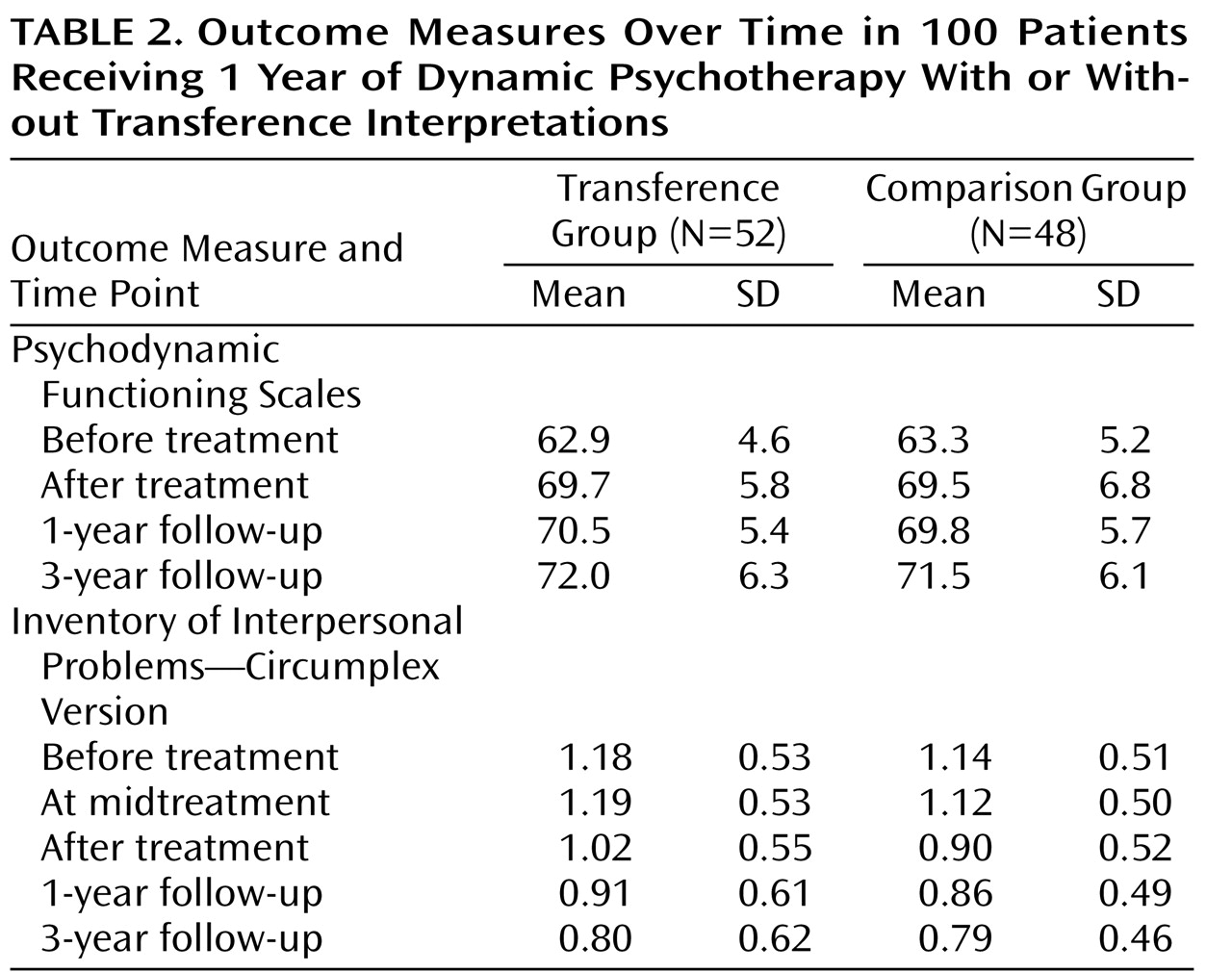
Primary Analyses of Outcome Variables
Descriptive statistics over time for the two outcome variables are presented in
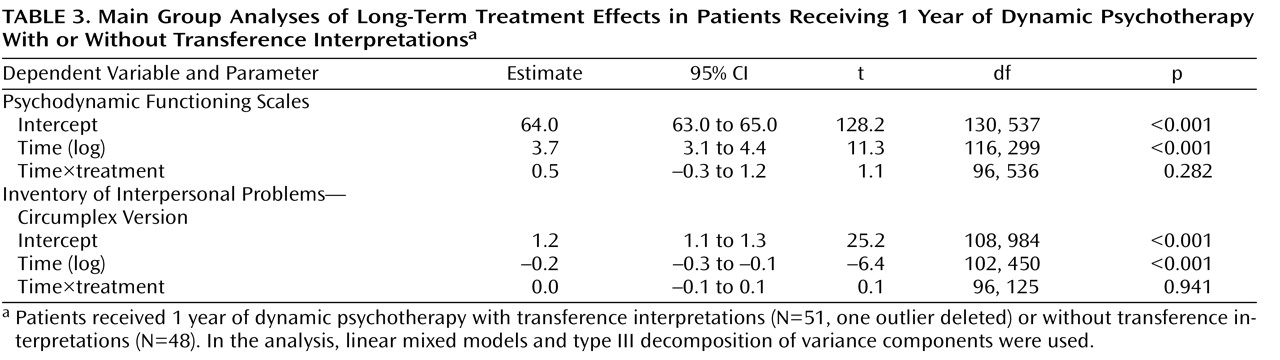
Table 2 . We detected no significant treatment differences for any outcome variable at any time point. Furthermore, we could detect no statistically significant time by treatment effects in the longitudinal analyses (
Table 3 ).
However, patients in both treatment groups also improved significantly on both outcome measures after treatment termination. Average improvements on the Psychodynamic Functioning Scales during the follow-up period were 2.3 (t=3.1, df=51, p=0.002) for the transference group and 2.0 (t=2.9, df=47, p=0.006) for the comparison group. The within-group effect sizes (Cohen’s d)
(27) were equal in the two groups at 0.4 (moderate). Within-group improvement after treatment on the Inventory of Interpersonal Problems—Circumplex Version was also statistically significant in both groups, and effect sizes were moderate.
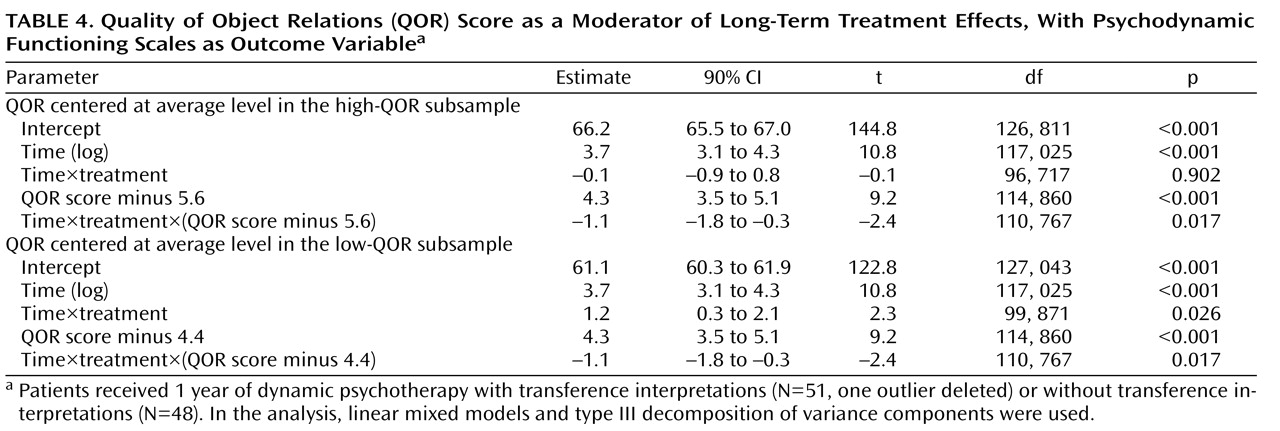
Moderator Analyses
When the QOR was included in the statistical model, a significant moderator effect was observed, using the Psychodynamic Functioning Scales as outcome variable. As shown in
Table 4, the long-term effect of transference interpretations increased with lower scores on the QOR. There was no treatment effect for the average patient with high QOR scores, but there was a statistically significant treatment effect for the average patient with low QOR scores.
Secondary analyses with global optimism as a covariate yielded the same pattern of results as those without the covariate. To assess the potential effect of dropouts in the comparison group, we included treatment completion status by time in the statistical model. This did not change the results. We detected no significant moderator effects using the Inventory of Interpersonal Problems—Circumplex Version as outcome variable. Presence of personality disorder was not a significant moderator of treatment effects.
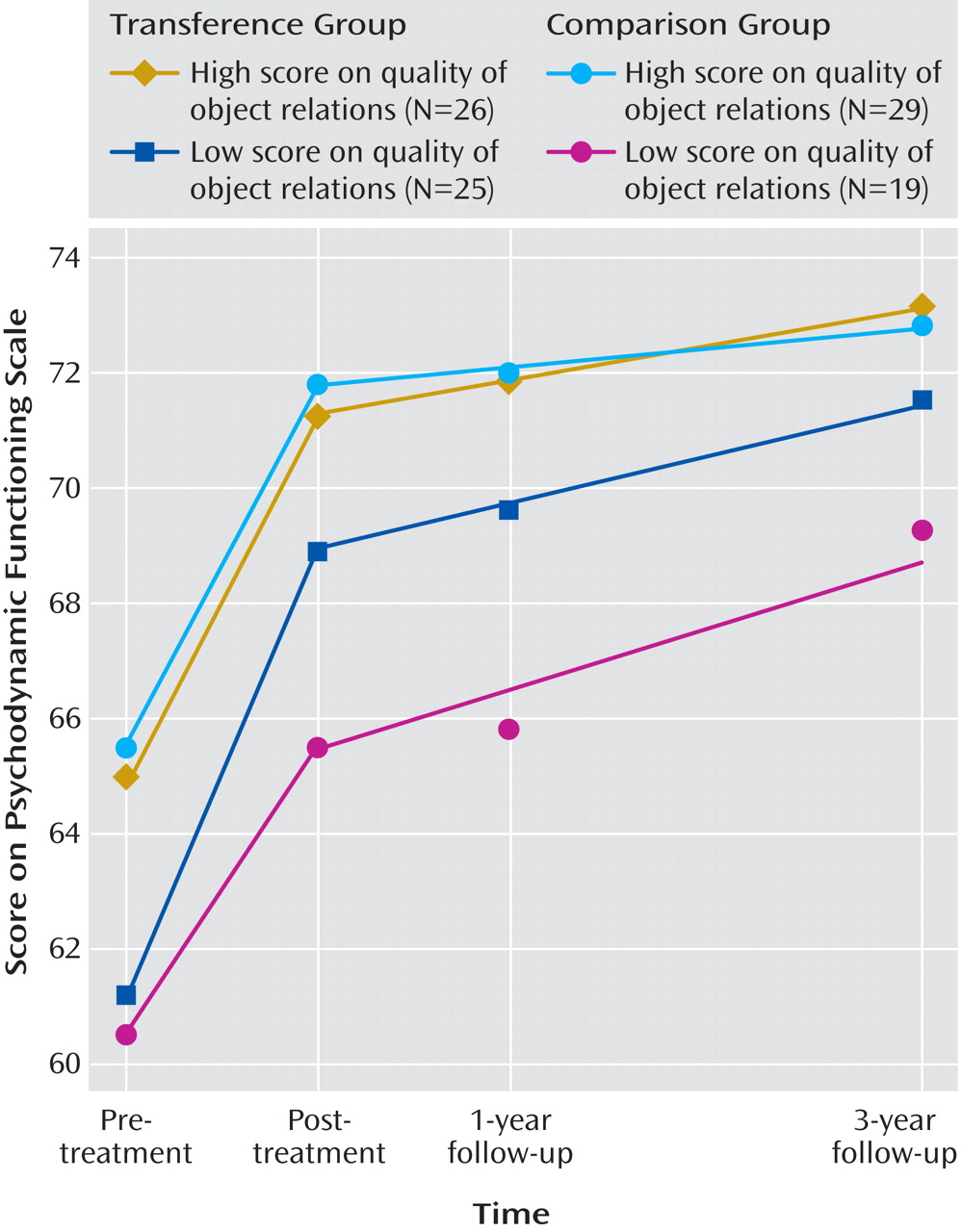
Subsample Analyses
Figure 2 shows the descriptive mean trajectories of the Psychodynamic Functioning Scales for each treatment group using subsamples of patients with high (N=55) and low (N=44) QOR scores. This illustrates the moderator effects of the QOR.
Throughout the 4-year study period, patients with low scores on the QOR in the transference group (N=25) had a more favorable outcome than did those in the comparison group (N=19). The mean difference between treatment groups on the Psychodynamic Functioning Scales was 3.1 at end of treatment (90% confidence interval [CI]=0.1 to 6.0; t=1.7, df=42, p=0.09), 3.0 at the 1-year follow-up (90% CI=0.2 to 5.9; t=1.8, df=42, p=0.08), and 2.2 at the 3-year follow-up (90% CI=–1.1 to 5.4; n.s.). The between-group effect sizes (Cohen’s d) were moderate: 0.54, 0.55, and 0.37 at the three time points, respectively. Improvement for patients with more mature object relations was similar in the transference group (N=26) and the comparison group (N=29) throughout the entire study period.
Discussion
Both treatment groups continued to improve after treatment, which is consistent with some findings from recent meta-analyses of manualized brief dynamic psychotherapy
(1,
2) . In a previous study from our group with a 4-year follow-up after treatment termination, the same posttreatment maturation was observed
(28) .
We detected no significant differences between the two treatment groups in occurrence of positive or negative life events or in the use of additional treatment after therapy. All patients completed the 3-year follow-up evaluation. Statistical analyses indicated that differential dropout cannot explain the results.
Equal average outcomes are typical when different psychotherapies are compared. This has led many researchers to conclude that technical differences between treatments have negligible effects
(29) . However, two treatments may be equally effective on average but work through different active treatment components in different patients
(22) . The QOR was a moderator of the long-term effect of transference interpretations. Contrary to mainstream clinical thinking and our second hypothesis, use of transference interpretation was more effective than avoidance of such interpretation with the ostensibly less suitable patients, that is, patients with low scores on the QOR.
Within the subsample of patients with low scores on the QOR, we detected no significant differences in positive and negative life events or use of antidepressant medication during the follow-up period. However, within this subsample, significantly more patients in the comparison group than in the transference group consulted a mental health professional during the follow-up period (comparison group: N=11, 58%; transference group: N=7, 28%; χ 2 =7.1, p=0.02). They also received additional psychotherapy significantly more often (comparison group: N=8, 42%; transference group: N=5, 20%; χ 2 =5.4, p=0.02), and they took sick leave more often (comparison group: N=7, 37%; transference group: N=3, 12%; Fisher’s exact test, p=0.05). Despite the fact that more than twice as many patients in the comparison group received additional treatment during the follow-up period, they had a less favorable course over the 4-year study period than the transference group. It is possible that the moderated long-term treatment effect of transference interpretations would have been stronger if additional treatment during the follow-up period had been equal for both groups.
No moderated long-term effect of transference interpretations was found when the Inventory of Interpersonal Problems—Circumplex Version was used as an outcome measure. Self-report scales have limitations and may be less sensitive in detecting change
(30) . The clinician-rated Psychodynamic Functioning Scales operationalize clinical inferences drawn by experts. In addition, these scales were rated with high precision, by three raters on each occasion.
Earlier studies indicated that transference interpretations had a negative impact on treatment outcome
(31 –
34) . These studies also reported that quality of object relations was a moderator of associations between the frequency of transference interpretations and outcome. Methodological limitations, especially in naturalistic designs, prohibit definite conclusions. Recent clinical trials have reported more positive findings. Bateman and Fonagy
(35) showed that a psychoanalytically oriented day treatment program for patients with borderline personality disorder was superior to standard psychiatric care. Svartberg et al.
(36) showed that short-term dynamic psychotherapy was at least as effective as cognitive therapy for patients with cluster C personality disorders. Clarkin et al. showed that 1 year of transference-focused psychotherapy for borderline patients was slightly superior to the well-established dialectical behavioral therapy
(37), or in some areas superior to dialectical behavior therapy
(38) . Giesen-Bloo et al.
(39), however, have reported that long-term schema-focused therapy was superior to transference-focused psychotherapy for borderline patients. In the present study, 60% of patients with low scores on the QOR had one or more personality disorders. Our study identifies a core active treatment component, transference interpretation, with positive long-term impact on patient functioning and thus represents an extension of previous work.
In this study, treatment was manualized and monitored. Although individually tailored treatments might yield somewhat different effects, experimental manipulation of treatment techniques is the only method currently available for studying causal effects. The lack of therapist effects in this study may be due to insufficient power. However, use of manualized treatments and experienced, specifically trained therapists tends to reduce therapist effects
(40) . The sample size was not large enough to provide accurate estimates of effect sizes. The population estimates may range from small to large. The patient sample had mixed diagnoses; the effects on depression, for example, cannot be evaluated with precision. However, diagnostic group (mood disorders versus other diagnoses) was not a moderator of treatment effects in this study. Our findings indicate that potential moderators should be included in studies of psychotherapy. Future research may add transference interpretations to other psychotherapy modalities for depressive, anxiety, and personality disorders and investigate the potential for improved outcomes.