High levels of nicotine and alcohol use are common in our society and are associated with a range of medical and social morbidities
(1,
2) . Because one of the most consistent predictors of nicotine and alcohol use is church attendance
(3 –
7), it is important for us to understand both the causes of church attendance and its association with psychoactive substance use.
Several studies have suggested an intriguing developmental pattern for the sources of individual differences in church attendance
(8 –
10) . In children, differences in church attendance appear to result largely from the shared environment, as might be expected if church attendance in children resulted largely from parental and community expectations
(11 –
14) . However, as individuals age, shared environmental influences on church attendance diminish in importance while genetic influences increase
(15 –
17) .
In this study we applied a developmental framework to examine the relationship between church attendance and alcohol and nicotine use in a sample of male twin pairs from the Virginia Adult Twin Study of Psychiatric and Substance Use Disorders (VATSPSUD)
(18) . We are interested in determining whether the sources of the correlation between church attendance and substance use change during development. Twin studies are ideal for this purpose. While they have been most commonly used to disentangle the role of genetic and environmental influences for individual traits or disorders, they can also determine the degree to which the correlation between two traits results from genetic versus environmental factors. If longitudinal data are obtained on twins, it then becomes possible to resolve developmental trends in the interrelationship of key variables, that is, to see if the underlying causes of their correlation change over time. Given the centrality in this article of this process—the decomposition, by a twin study, of the correlation between church attendance and substance use—we begin by explicating the conceptual foundation of this method.
Assume we want to understand why frequent church attendance in a teenage male twin is associated with low levels of alcohol consumption. One possibility would be that parents who require their twin boys to go to church with them regularly also teach them about the dangers of alcohol use, carefully monitor their behavior and friends to reduce the likelihood of their exposure to alcohol-abusing peers, and bring them into frequent contact with other families and social settings that discourage alcohol use. Here, church attendance is a marker for a set of familial-environmental behaviors, expectations, and attitudes that reduce the risk for heavy alcohol use.
If we shift our focus to the individual behavior of our subject, we can ask, “What kind of teenage male would prefer to comply with parental requests to go to church each Sunday as opposed to resisting parental pressure and going to spend time with friends?” Plausibly, the genetically influenced temperament of a teenager who wanted to conform with parental and community expectations and/or directly found the religious experience itself rewarding would also be disinclined—because of high levels of conscientiousness and low levels of novelty seeking—to seek out and consume substantial amounts of alcohol. In this scenario, a high level of church attendance is a marker for a set of genetically influenced traits that would reduce the chances of heavy alcohol use.
Finally, imagine that our teenage male has a serious girlfriend. She herself is quite religious and wants her boyfriend to accompany her to church. While she enjoys movies on a Saturday night, she actively discourages her boyfriend from going to places where alcohol is easily available. That is, her expectations increase the rate of church attendance in our teenager at the same time that they reduce his risk of heavy alcohol consumption. In this scenario, church attendance is a marker for a set of environmental experiences that our twin does not share with his co-twin and that would also influence his chances of consuming alcohol.
In this study, then, we had two goals: to determine whether the impact of genetic and environmental factors on church attendance changes from childhood to adulthood and to investigate whether the shared-environmental, genetic, and unique-environmental pathways from church attendance to alcohol and nicotine use change in importance over this same developmental period. That is, referring to the three scenarios above, could their relative importance in explaining the association between church attendance and substance use alter as individuals grow from early adolescence to adulthood?
Method
Sample
We used data collected in the first and third waves of interviews of members of Caucasian adult male-male twin pairs born between 1940 and 1974 from VATSPSUD
(18) . All VATSPSUD participants were ascertained from the Virginia Twin Registry, a population-based register formed from a systematic review of birth certificates in the Commonwealth of Virginia. Response rates for the first (1993–1996) and second (1994–1998) waves of interviews were 72.4% and 82.6%, respectively. The third interview wave, restricted to male-male twins, was completed between 1998 and 2004 by 1,796 male twins (75%) who had participated in the second interview, including both members of 469 monozygotic and 287 dizygotic pairs. Participants, most of whom were interviewed by telephone, then were a mean age of 40.3 years (SD=9.0). After receiving a description of the research protocol, participants signed informed-consent forms for face-to-face interviews and provided verbal consent for telephone interviews. The project was approved by the Office of Research Subjects Protection at Virginia Commonwealth University. Members of a twin pair were always interviewed by different interviewers. Zygosity was assigned by a combination of self-report measures, photographs, and DNA polymorphisms
(18) .
Assessment
At the first interview, when our sample’s mean age was 34.6 years (SD=8.9), we assessed frequency of church attendance by inquiring, “How often do you attend church or other religious services?” Possible responses varied from “at least once a day” to “once a month or less.” We also inquired how often, during the past year, they consumed alcohol and on average how many drinks they usually had when they drank; a drink was defined as “one bottle of beer, one glass of wine, or one shot of liquor.” We combined these two measures to calculate an average number of drinks per month, which we divided into seven groups: 0, 1–5, 6–15, 16–30, 31–60, 61–200, and over 200.
As detailed in a previous report
(19), in the third interview a life history calendar was used to improve recall accuracy
(20) . The calendar contained columns for each year of the respondent’s life
(21) . The initial rows, completed at the start of the interview, recorded key changes in living situation and major educational, employment, and interpersonal milestones. Toward the end of the interview, we returned to the calendar and obtained a year-by-year history of average cigarette and alcohol use. If necessary, the interviewers used memory prompts from the information previously recorded on the calendar to cue the respondent into the relevant “memory files.” For cigarette use, we inquired about the average number of cigarettes smoked per day. For alcohol, we inquired separately about the average number of days per month on which the respondent consumed alcoholic beverages and the average number of drinks consumed per day when drinking and, as in the first wave of interviews, combined them to calculate an average monthly intake. From this calendar data, we averaged the number of drinks per month of alcohol for the age periods 12–14 and 15–17 and, for analysis, divided them into the same seven groups described above. For cigarette use, we calculated the average daily use for ages 12–14 and 15–17 and for the year in adulthood when they completed their first interview, and we also divided them into seven groups: 0, 1–5, 6–10, 11–20, 21–30, 31–40, and over 40. We did not examine substance use before the age of 12 because prior analyses indicated that it was too rare to generate stable twin models
(22) .
The third interview wave also contained sections inquiring about a range of traits over five age periods. For three of these (ages 8–11, 12–14, and 15–17), we asked, “When you were between the ages of x and y, how often would you attend religious services?” Possible responses ranged from “more than once a week” to “never.”
We assessed the test-retest reliability of our results from the third interview wave from 142 randomly chosen participants interviewed an average of 29 days apart. As we showed previously
(19), test-retest reliability for our measures of average alcohol and nicotine use for each year, as assessed by a polychoric correlation, ranged from 0.80 to 0.95. The test-retest polychoric correlation for church attendance was 0.88 for ages 8–11, 0.84 for ages 12–14, and 0.90 for ages 15–18. We did not assess test-retest reliability for our first interview with this cohort.
Statistical Analyses
The goal of our first analysis was to decompose the variance in church attendance into its genetic and environmental components. We assume that twin resemblance arises from two latent factors. The first of these is additive genes, symbolized by the letter A, which contribute twice as much to the monozygotic as to the dizygotic twin correlation because monozygotic twins share all of their genes while dizygotic twins share, on average, half of their genes identical by descent. The second source of twin resemblance included in our models is shared or common environment (symbolized by the letter C), which contributes equally to the correlation in monozygotic and dizygotic twins and reflects environmental experiences in the home, community, or school that make twins more similar with respect to their church attendance. In addition to this shared environment, the model also contains individual-specific environmental effects (symbolized by the letter E) that reflect those true environmental experiences that make members of a twin pair differ in their church attendance as well as errors of measurement.
For model fitting, we used the software package Mx (23; http://www.vcu.edu/mx). All twin models were fitted directly to the raw data organized by twin pairs. Each record contained the substance use, church attendance, and zygosity data for one pair of twins. The models were fitted using the normal-theory maximum-likelihood approach for ordinal data. This method involves numerical integration to calculate the probability that twins’ observed scores stem from a particular region (bounded by thresholds) of the multivariate normal distribution. Bivariate or quadrivariate integration of the normal distribution was used for univariate or bivariate twin modeling, respectively. For the univariate analyses of church attendance, we presented results of the full or ACE model only, assuming equality of thresholds across twins within a pair and within zygosity groups.
The second goal was to conduct bivariate analyses that sought to decompose the sources of correlation between church attendance and substance use. The ability of twin studies to resolve the sources of resemblance of two traits like church attendance and substance use comes from the comparison of three correlations: within individuals, across monozygotic twin pairs, and across dizygotic twin pairs. For example, if genetic factors are an important cause of their association, the two traits will be correlated much more highly across monozygotic than across dizygotic twin pairs. By contrast, if shared environmental factors are critical, then the trait correlations will be very similar in the two twin types. Finally, if the traits are largely correlated because of environmental experiences unique to the individual, then they should be more strongly correlated within individuals than across monozygotic twins.
For these analyses, we began by fitting the full ACE model and then tested the two key AE and CE submodels. We used Akaike’s information criterion (AIC)
(24,
25) for model selection. The lower its value, the better is the balance between explanatory power and parsimony. To provide a firm statistical baseline for our modeling, we compared these full ACE models with entirely saturated models (which contain a separate parameter for each variable in our model including all of the thresholds—e.g., in monozygotic and dizygotic twins and in twin 1 and twin 2 for each twin pair). In each case, the AIC value of the full ACE model was superior to that of this fully saturated model.
Results
Developmental Effects on Church Attendance
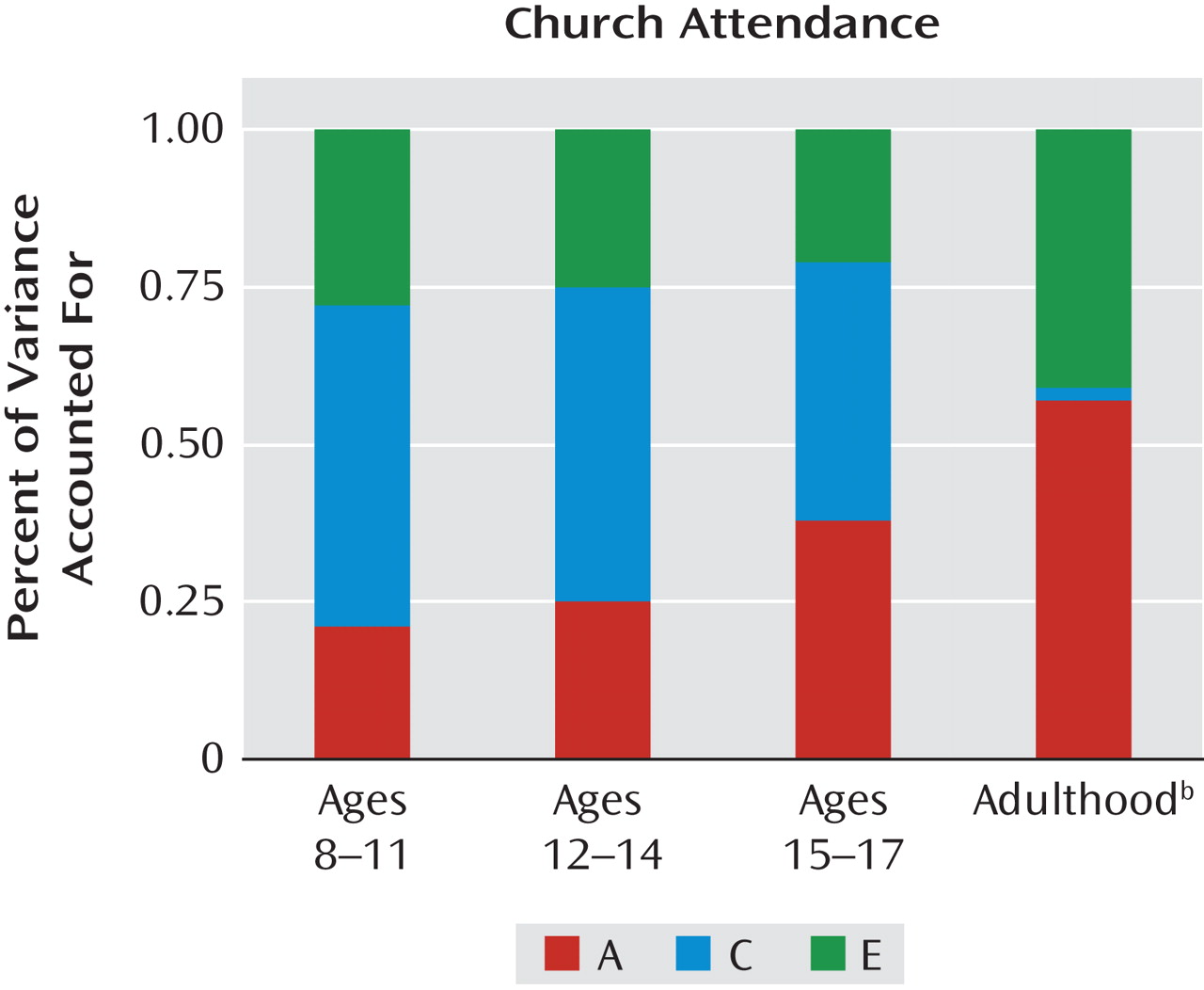
We began by fitting full (or ACE) models to our twin data on church attendance at ages 8–11, 12–14, and 15–17 and in adulthood. The results are summarized in
Figure 1 . In childhood, shared environment is by far the most important source of individual differences in church attendance (50%). This did not change in early adolescence (50%), and it dropped only modestly to 41% by late adolescence. However, in adulthood, the impact of shared environment on church attendance declined dramatically to a statistically nonsignificant 3%. By contrast, the heritability of church attendance was low in childhood (21%), grew modestly to 25% in early adolescence, jumped considerably to 38% by late adolescence, and climbed further to 58% in adulthood. Individual-specific environmental effects were relatively stable throughout childhood and adolescence (ranging between 21% and 28% of the variance) but then rose substantially to 41% in adulthood.
Developmental Changes in the Sources of the Correlation Between Church Attendance and Substance Use
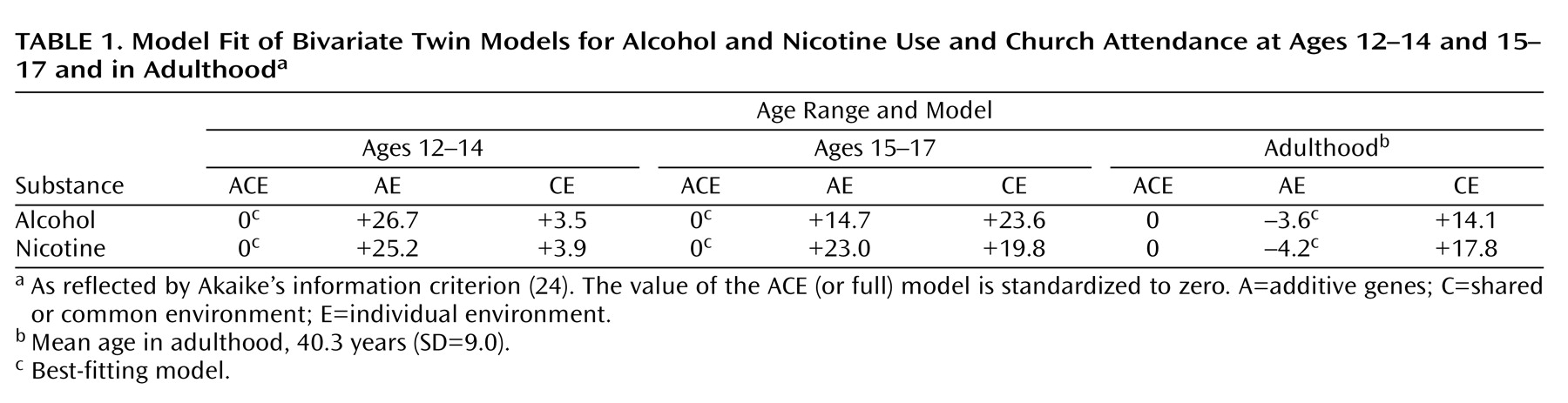
We began by fitting bivariate twin models of church attendance and substance use across the three ages (
Table 1 ). In each case, we compared the fit of the full (or ACE) model with a model that restricted the sources of twin resemblance for both traits to additive genetic effects (AE) or to shared environmental factors (CE). The results were similar with both alcohol and nicotine. By a considerable margin, the ACE model fit best for ages 12–14 and 15–17, while the AE model fit best for adulthood.
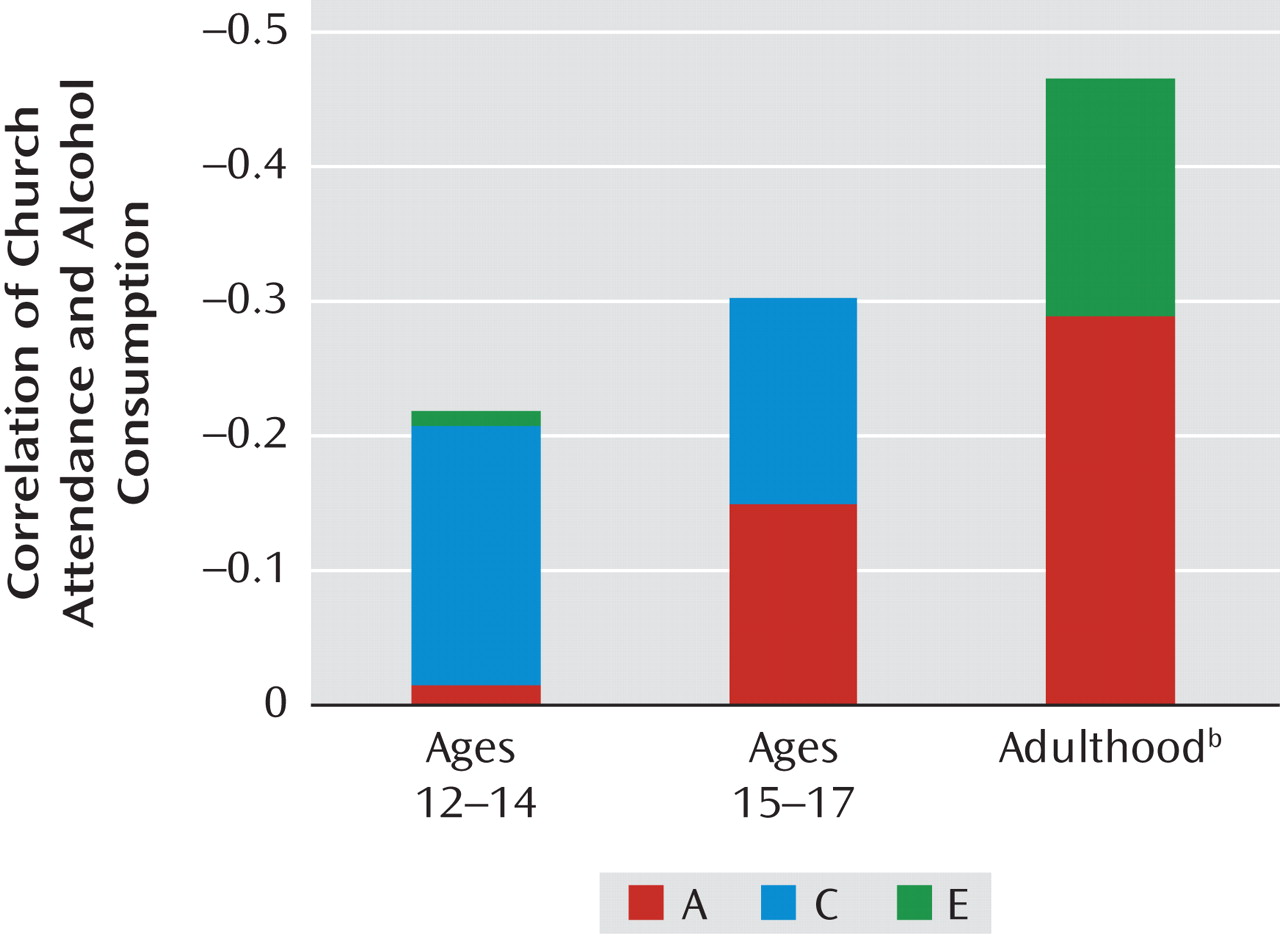
The results for the best-fitting models for church attendance and alcohol use and for church attendance and nicotine use were similar, as shown in Figures 2 and 3. These figures present the proportion of the observed correlation between church attendance and substance use that resulted from genetic, shared environmental, and individual-specific environmental factors. Starting with alcohol (
Figure 2 ), we see that the total correlation with church attendance increased substantially in absolute value from –0.22 at ages 12–14 to –0.30 at ages 15–17 to –0.47 in adulthood. At ages 12–14, nearly all of the correlation (88%) resulted from shared environmental effects, while the parallel figures at ages 15–17 and in adulthood were 51% and zero. By contrast, the impact of genetic factors on the correlation of church attendance and alcohol intake increases steadily over development both in absolute magnitude (producing correlations of –0.02, –0.15, and –0.29 over the three ages) and proportionally (accounting for 7%, 49%, and 62%, respectively, of the total correlation). The proportion of the correlation between church attendance and alcohol use that resulted from individual-specific environmental effects was very small at ages 12–14 (–0.01) and undetectable at ages 15–17, and it accounted for 38% of the church attendance-alcohol relationship in adulthood.
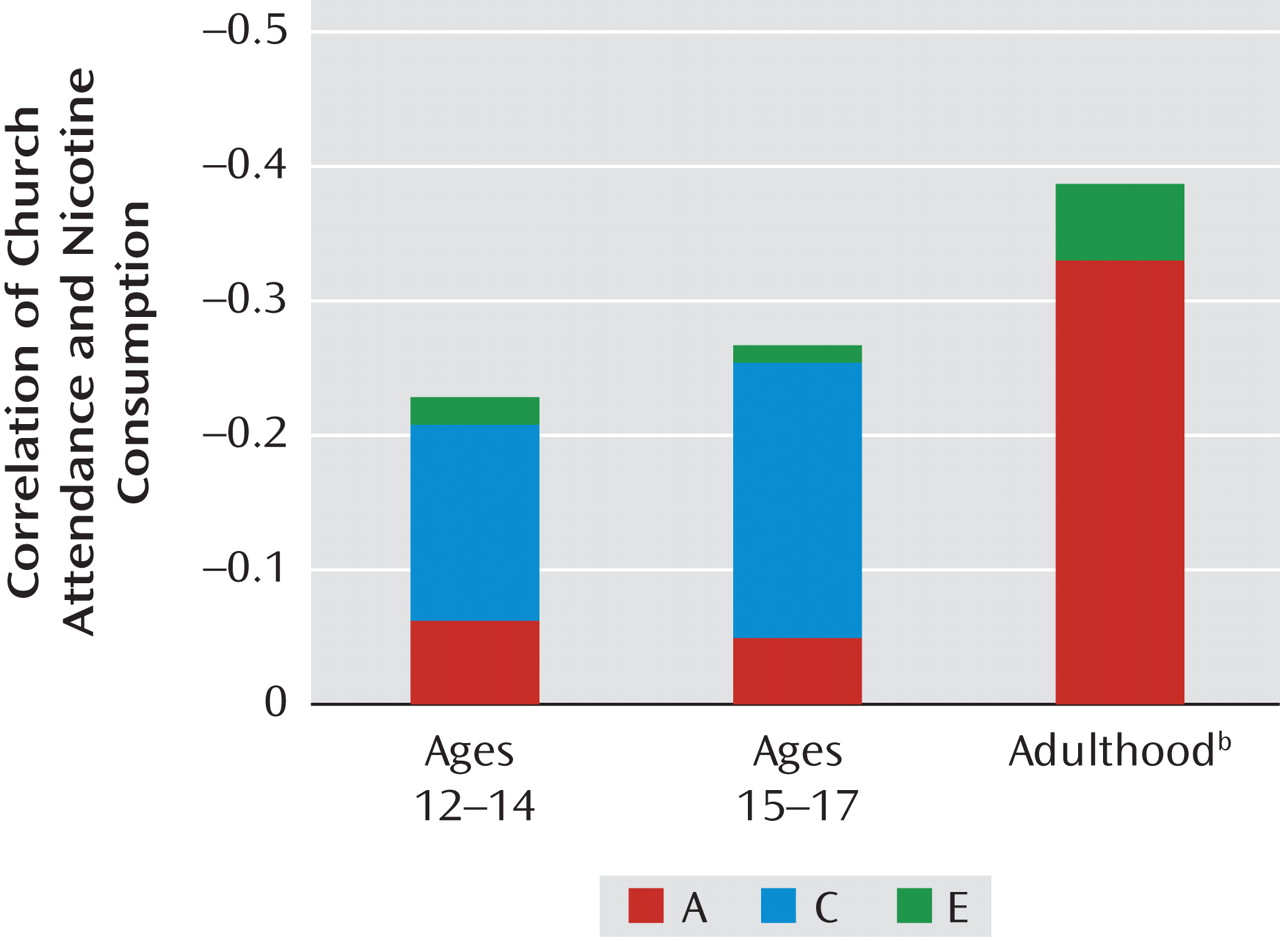
As with alcohol, the overall correlation between church attendance and nicotine use also increased substantially over time (
Figure 3 ). In both early and later adolescence, the correlation was largely a result of shared environmental factors (64% and 76%, respectively), with a modest genetic contribution. In adulthood, the picture was quite different. Most of the correlation (85%) between church attendance and nicotine use arose from shared genetic factors. As with alcohol use, individual-specific environmental factors played a small role in the relationship between church attendance and nicotine use in adolescence but increased moderately in importance in adulthood.
Discussion
This study had two interrelated goals: to examine whether the sources of individual differences for church attendance change from childhood to adulthood and to explore (for the first time, to our knowledge) whether the pathways responsible for the strong association between church attendance and psychoactive drug use undergo developmental change.
Consistent with previous studies (for example, references 9, 10), we found dramatic alterations in the etiologic role of genetic and environmental factors in church attendance with development. In childhood and early adolescence, individual differences in church attendance derive largely from shared environmental effects. Over time, however, shared environmental factors become less and less important while genetic factors become increasingly influential in frequency of church attendance. By adulthood, church attendance is largely influenced by genetic and individual-specific environmental factors, with virtually no role for the shared environment.
These results, in accord with our previous findings with peer group deviance in this sample
(22), suggest that as individuals age, they increasingly shape their own social and religious behavior in large part through their genetically influenced temperament. In childhood, church attendance is probably strongly influenced by parental and community expectations. However, as children develop into early and then late adolescence, they can begin to assert their own preferences about whether they wish to attend church. Once they are adults, they are able to decide entirely for themselves whether or not to attend church. As Windle et al.
(26) noted, “Socially and emotionally early adolescents increasingly desire autonomy and the opportunity to participate in decision-making that affects their daily lives,” and during this stage of development they are typically “provided with increased behavioral autonomy by their families” (pp. S275–S276).
Our results are consistent with prior evidence that level of religiosity is protective against problematic alcohol consumption in adolescence
(27,
28) . Interestingly, in reviewing this subject, Windle
(29) concludes, consistent with one key aspect of our own findings, that the impact of religiosity on alcohol intake in adolescence is “optimally conceptualized as an indirect effect … [via] family relationships and community ties” (p. 46).
For church attendance alone, as well as for the correlation between church attendance and alcohol and nicotine use, individual-specific environmental influences grow in importance over time. This is not unexpected, as contact between twins typically declines with age and twins’ respective social networks become increasingly independent
(22) . We suspect that much of this unique environmental effect results from the twins in adulthood associating with distinct sets of friends and different romantic partners. We know from other research that individuals are substantially correlated for both measures of religiosity and of alcohol and nicotine use with their partners and friends
(30) .
These analyses do not directly address how, via shared or unique environmental processes, church attendance would affect substance use. In Western countries, including the United States, church attendance is an important cultural variable that indexes a range of social attitudes and values that often include negative views about the use of psychoactive substances
(31 –
33) . This is well illustrated by findings from a study of religious attitudes in a different subset of the VATSPSUD sample
(7) . In that investigation, the questionnaire items “I believe drinking alcohol is a sin” and “I believe that smoking cigarettes is a sin” loaded substantially on a “social religiosity” factor that also included items assessing the frequency of church attendance
(7) . While we hope to address this important question in further analyses, our working hypothesis is that from an environmental perspective, frequent church attendance is an indicator of a set of negative attitudes toward the use and consequences of alcohol, nicotine, and other psychoactive substances. We also suspect, but need to confirm empirically, that the genetic pathways between church attendance and substance use are more likely mediated by personality and temperamental variables.
This study well illustrates the potential complexity of human developmental processes. A standard longitudinal study might show increasing inverse correlations between church attendance and psychoactive substance use over time but provide no hint that underneath these correlations the specific causal processes involved were changing dramatically. Genetically informative samples can often provide important insights into developmental processes that would be very difficult to obtain in other ways. Given the strength of the association between church attendance and substance use and the substantial morbidities associated with excess consumption of alcohol and nicotine, the pattern of findings uncovered in these analyses can help inform our efforts to prevent and reduce harmful consumption of psychoactive substances.
Limitations
These results should be interpreted in the context of three potentially important methodological limitations. First, our participants were all white male twins born in Virginia. Prior work in the VATSPSUD has shown that this population is over 85% Protestant, of whom approximately 60% are fundamentalist or Baptist
(17) . Our results may not extrapolate to other populations with different patterns of religious affiliations.
Second, we obtained detailed nicotine consumption data only on cigarettes, so non-cigarette sources of nicotine (such as pipes, cigars, and chewing tobacco) are not captured in these analyses. Third, our information on both church attendance and substance use in childhood and adolescence was obtained retrospectively and may be subject to recall bias. We tested the reliability of our assessments, and they were all excellent. Where there were sufficient data (for alcohol use during ages 15–17 and tobacco use during ages 12–14 and 15–17), we found no evidence that the reliability of recall of substance use differed as a function of the frequency of church attendance in adulthood. An unusual pattern of recall bias would be needed to produce our findings artifactually. Furthermore, we used a life history calendar to collect these data. This method reflects the structure of autobiographical memory and promotes sequential retrieval within memory networks, thereby improving substantially the completeness and accuracy of retrospective reporting
(20,
34 –
36) .