Numerous studies have shown that attention deficit hyperactivity disorder (ADHD) symptoms and diagnoses are associated with educational attainment (
1,
2). However, despite an early synthesis (
3) pointing strongly to inattention as potentially the best predictor of later school failure, most studies have not differentiated inattention and hyperactivity. Therefore, it remains unclear whether these dimensions operate additively or interactively or whether one dimension is more important than the other (
1,
2,
4). Clarifying these issues has theoretical and practical implications. At the theoretical level, it will help in identifying the possible mechanisms linking ADHD symptoms to educational attainment (
5). At the practical level, it will help in focusing intervention efforts more strategically (
6). The screening process for at-risk children would also benefit from this clarification by specifying whether children who demonstrate high levels of both dimensions are more at risk than children demonstrating high levels of only one dimension. The aim of the present study was to examine the unique, additive, or interactive contributions of inattention and hyperactivity symptoms during the elementary school years to educational attainment (defined by high school graduation).
We also addressed some limitations of previous studies. First, few studies have estimated the respective contributions of inattention and hyperactivity (
1) while controlling for the child's sex, socioeconomic status, and intelligence. The inclusion of these confounding variables is necessary because they are strongly related to both ADHD symptoms and educational outcomes (
7,
8). Second, few studies have controlled for comorbid conditions, an important limitation given that externalizing and internalizing problems overlap with ADHD (
9–
11) and are associated with educational attainment. Indeed, hyperactivity symptoms are strongly associated with externalizing disorders such as physical aggression (
12) or opposition (
13,
14), whereas inattention symptoms seem more likely to be associated with internalizing problems such as anxiety/depressive symptoms (
15,
16).
Finally, only two prospective studies with the necessary confounding variables made the distinction between inattention and hyperactivity symptoms (
2). Lee and Hinshaw (
17) followed girls who were first diagnosed with ADHD when they were between the ages of 6 and 13 years and showed that only inattention symptoms predicted educational achievement 5 years later. Massetti et al. (
4) followed young children diagnosed using modified criteria for ADHD and found that only the inattentive group had consistently lower achievement scores. Unexpectedly, results for the inattentive/hyperactive group were only marginally significant, and the hyperactive group did not differ from the comparison group. Both these studies relied on highly selected or clinically referred participants. Moreover, one study examined educational achievement in girls throughout adolescence, whereas the other examined children in their early teen years. If ADHD symptoms are trait-like and continuously distributed in the population, the differential predictive power of inattention and hyperactivity problems for long-term educational outcomes should hold true in a population sample, which remains to be tested (
18–
20).
The present study is based on a population sample of children in the school system in one of the Canadian provinces. We utilized behavioral assessments made by different teachers between the end of kindergarten (6 years of age) and the end of elementary school (12 years of age) and obtained the official record of high school graduation (by the age of 22–23 years). We included the aforementioned confounding variables as well as additional confounding variables previously shown to be associated with ADHD symptoms and/or educational attainment (i.e., birth weight and sociodemographic variables). To take into account the richness of repeated teacher assessments of inattention and hyperactivity throughout the elementary school years, developmental trajectory analyses were utilized (
21,
22). We hypothesized that ADHD symptoms would predict high school graduation even after the inclusion of meaningful confounding variables and that inattention symptoms would be a better predictor than hyperactivity symptoms.
Method
Participants
In 1986–1987, a representative sample (N=6,397) of kindergarten children in the French-speaking schools of the province of Québec was selected. Both teachers and mothers completed the Social Behavior Questionnaire for 3,715 of these children (
23). Of these 3, 715 children, 2,000 (1,001 boys) were randomly selected for participation in the present study and followed longitudinally. Information on high school graduation was obtained from the Québec Ministry of Education official records and was available for the whole sample. Among the 2,000 study participants, 32.1% did not graduate from high school relative to 34.1% among the initial representative sample. Although statistically significant (χ
2=5.36, df=1, p=0.02), this difference is clearly low in magnitude. Additional information regarding attrition and missing data for the 2,000 participants followed longitudinally is presented in this report. After complete description of the study, written consent was obtained at each wave of data collection from the mothers (including consent regarding teachers' reports).
Instruments and Measures
Teachers rated children with the Social Behavior Questionnaire each year from kindergarten to sixth grade, providing seven assessment points from the age of 6 to 12 years. (In Québec, within this age range a teacher teaches only at one level, and thus the assessments were made by a different teacher each year.) The Social Behavior Questionnaire is based on the Children's Behavior Questionnaire (
24) and the Preschool Behavior Questionnaire (
25), which both demonstrate good psychometric properties, particularly test-retest reliability. These results for test-retest reliability have been replicated with the Social Behavior Questionnaire (
23). Furthermore, the Social Behavior Questionnaire was used in several studies of large sample cohorts that documented its predictive validity on a range of adolescent and adult outcomes, particularly for hyperactivity and inattention (
12,
21,
22,
26 [also see the data supplement accompanying the online version of this article]). We assessed hyperactivity with the following two items from the scale: 1) restless, runs about, or jumps up and down, does not keep still and 2) squirmy, fidgety child (Cronbach's alpha for the seven assessments: 0.84–0.89). The following four items were used to assess inattention: 1) weak capacity for concentration, cannot maintain his or her attention for a long time on the same task; 2) easily distracted; 3) absentmindedness; and 4) gives up easily (Cronbach's alpha for the seven assessments: 0.85–0.90). Each item for both dimensions was scored from 0 to 2.
The measure of educational attainment differentiated participants who had a high school diploma at 22–23 years of age (coded as 0) and those who did not (coded as 1). The latter category represented 32.1% of the participants (and included individuals who dropped out of school [17.2%] and individuals receiving vocational and adult education [14.9%]).
Initial individual-level confounding variables were sex (coded as 0 for girls and 1 for boys) and birth weight (coded as 1 for low birth weight [under 2,500 g, N=6.7%] and 0 otherwise). Socioeconomic variables were as follows: years of schooling of each parent, assessed when the child was 6 years old (mother: mean=11.97 years [SD=2.56], father: mean=12.17 years [SD=3.42]); occupational socioeconomic index of each parent, assessed when the child was 6 years old and based on criteria by Blishen et al. (
27) (mother: mean rating=44.01 [SD=13.03], father: mean rating=44.00 [SD=14.88]); and annual income of the whole family, assessed when the child was 7 years old and divided into categories (from 1 to 13) of $5,000 (Canadian), with category 1 being <$5,000 and category 13 being >$60,000 (median income score=7/13; interquartile range=5/13). Family structure was assessed when the child was 6 years old; a score of 1 was given if the child was living with both biological parents (N=82.7%) and a score of 0 otherwise.
We included the following two additional control variables reflecting changes in the family between the ages of 6 and 12 years of age, since these changes can influence educational success (
28): 1) a documented divorce or a separation between the two biological parents (N=13.9%) and 2) a residential move (N=40.5%). These two variables were derived from annual questions asking whether the target event had occurred within the previous year. A score of 1 indicated that the informant reported the occurrence of the event during this period.
We also assessed dimensions that co-occur with inattention and hyperactivity. The three behavioral dimensions (anxiety/depressive symptoms, physical aggression, and opposition) were assessed from age 6 through age 12 years, as rated by the child's teachers with the Social Behavior Questionnaire. Each item was scored from 0 to 2, depending on how frequently the child manifested the behavior. The score for each dimension was averaged across the 7 years of assessment. We used the following five items to assess anxiety/depressive symptoms: 1) is worried, worries about many things; 2) tends to do things on his own, rather solitary; 3) appears miserable, unhappy, tearful, or distressed; 4) tends to be fearful or afraid of new things or new situations; and 5) cries easily (mean score=2.00 [SD=1.33]; Cronbach's alpha: 0.72–0.77). Assessment of physical aggression encompassed the following three items: 1) fights with other children; 2) bullies other children; and 3) kicks, bites, or hits other children (mean score=0.47 [SD=0.87]; Cronbach's alpha: 0.81–0.88). Assessment of opposition encompassed the following five items: 1) irritable, quick to “fly off the handle;” 2) is disobedient; 3) does not share toys; 4) blames others; and 5) inconsiderate of others (mean score=1.32 [SD=1.48]; Cronbach's alpha: 0.79–0.83). Scores of verbal intelligence were obtained at age 15 years using the Sentence Completion Test (mean score=9.87 [SD=1.52]; range: 0–13), which demonstrated a high correlation with other verbal and nonverbal measures of intelligence and with educational achievement, irrespective of population characteristics (
29).
Data Analysis
First, we estimated trajectories of inattention and hyperactivity during elementary school using k-means for longitudinal data (
30). In this procedure, each observation is first assigned arbitrarily to one group. Then, the mean of each group is calculated and each observation is reassigned to the group with the closest mean. The operation is repeated until convergence. The estimations are repeated a large number of times (10,000 times in the present study) to obtain the best solution as assessed by a criterion that maximizes a ratio computed by dividing the trace of the between-variance by the trace of the within-variance.
Next, we used a binary logistic regression to examine the predictive links between the trajectories and later high school graduation, controlling for confounders. Many of the confounding variables were strongly intercorrelated, and thus we adopted a stepwise procedure. We entered these variables one at a time and did or did not keep them in the model according to a criterion dependent on the imputation procedure. At the final stage, we entered the trajectories of hyperactivity and inattention together. We tested for a two-way interaction between inattention and hyperactivity as well as two-way interactions between either inattention or hyperactivity and each confounding variable.
Attrition and Missing Data
Information on high school graduation was available for all participants. All also had at least one assessment of inattention and hyperactivity over the seven time points. Participants with at least one assessment were included in the estimation procedure for the trajectories (
30) (98.0% had three or more assessments for both dimensions).
For the confounding variables, 0%–20% of the data were missing except for birth weight (24.4%), family income (43.5%), and verbal IQ (38.4%). Even though the percentage of missing data were low for most variables, deletion of cases with missing data for one variable would have resulted in a strong power decrease and a possible bias as a result of differences in the characteristics of nonrespondents. Consequently, we performed multivariate imputation by chained equations to generate 50 complete data sets, a number considered to be sufficient (
31,
32). We then fitted the logistic model to each of the 50 imputed data sets and pooled the resulting estimates. This procedure also calculated the fraction of missing information for each estimate, which was attributable to the uncertainty caused by the missing data. We could then directly compare different statistical models fitted to the same imputed data sets. In the aforementioned stepwise procedure for the selection of the confounding variables, the decision to retain or eliminate a given variable was based on a Wald test assessing the information added to the model by the variable.
Results
Developmental Trajectories of Inattention and Hyperactivity
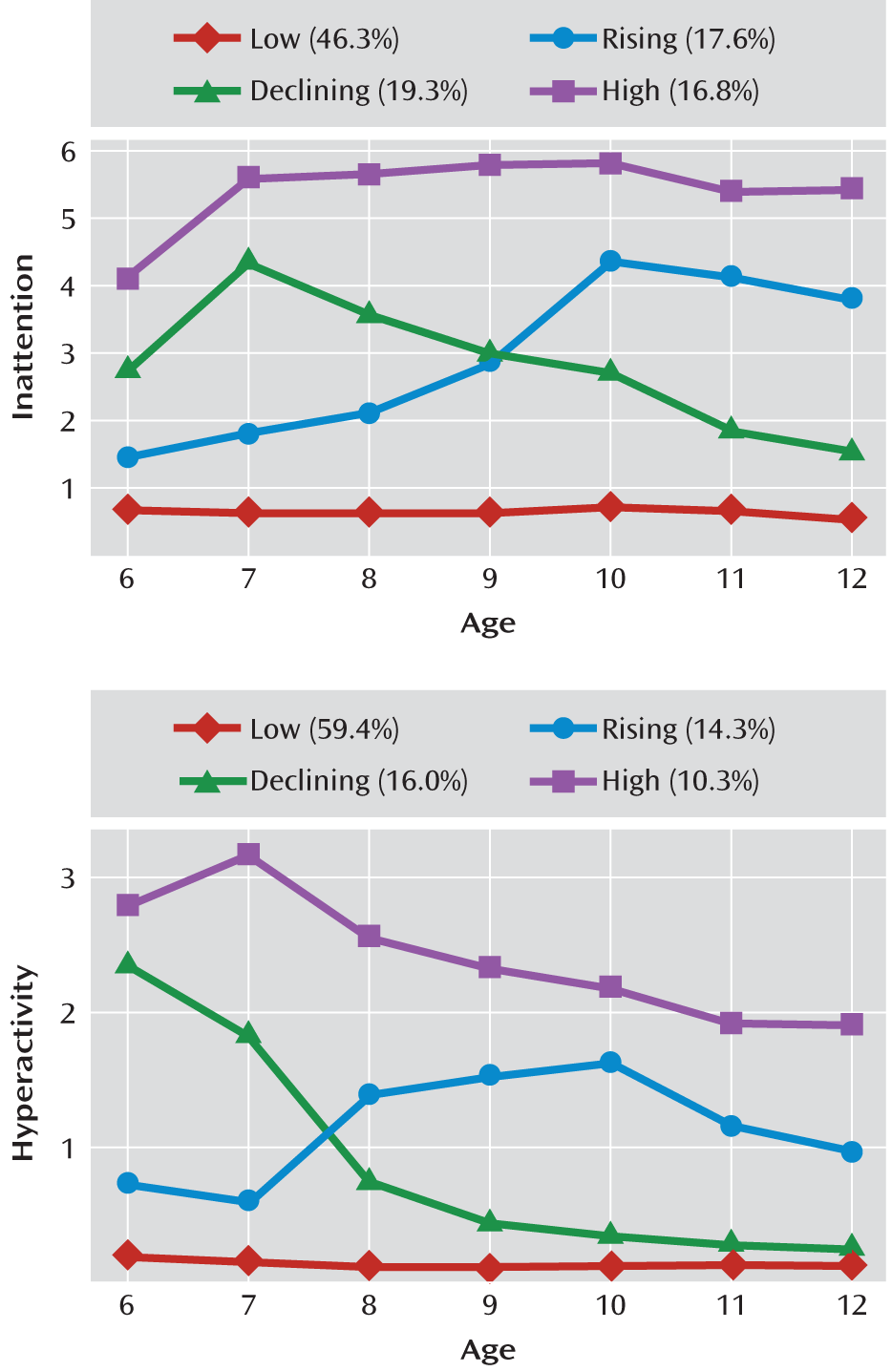
The following four developmental trajectories of inattention were identified from the analysis (
Figure 1): one stable low trajectory (46.3% of the study sample); one stable high trajectory (16.8%); and two crossing trajectories, with one rising (17.6%) and one declining (19.3%). The following four trajectories of hyperactivity were found (
Figure 1): one stable low trajectory (59.4%); one high declining trajectory (10.3%); and two crossing trajectories, with one sharply declining (16.0%) and one slightly increasing (14.3%). Biederman (
9) emphasized that symptoms of hyperactivity tend to wane, whereas symptoms of inattention tend to persist over time. In the present study, two hyperactivity trajectories were declining, and only one was slightly increasing, whereas for inattention only one trajectory was declining, while the others were stable or sharply increasing.
Prediction of High School Graduation
A total of 67.9% of the participants in the whole sample had a high school diploma at the age of 22–23 years.
Table 1 shows that those in the high inattention trajectory were the least likely to have a high school diploma at the age of 22–23 years (29.2%), while those in the low inattention trajectory were the most likely to have completed high school (88.5%). The difference between the high and low hyperactivity groups was smaller (40.1% versus 77.1%, respectively).
Bivariate associations are presented in Table 1 of the data supplement. All variables significantly predicted high school graduation (p<0.001) except birth weight. Socioeconomic variables, anxiety, and verbal IQ correlated more with inattention than hyperactivity. Hyperactivity was strongly correlated with physical aggression and opposition. Parental separation between the ages of 6 and 12 years increased the risk of being in a higher inattention trajectory, particularly the rising trajectory, suggesting the importance of time-varying covariates of these trajectories.
To build the model predicting high school graduation, we used a stepwise procedure for the confounding variables and then entered the trajectories for hyperactivity and inattention. When contrasted with the low inattention trajectory, the declining inattention trajectory (odds ratio=2.67, 95% confidence interval [CI]=1.90–3.75), rising inattention trajectory (odds ratio=3.87, 95% CI=2.75–5.45), and high inattention trajectory (odds ratio=7.66, 95% CI=5.06–11.58) all indicated an increased risk for not graduating from high school (
Table 2). In contrast, the hyperactivity trajectories were not significantly associated with high school graduation after accounting for inattention trajectories. We compared the fit of a model, including all the confounding variables as well as inattention, to a model with hyperactivity added and found that hyperactivity did not add significant information to the model.
The interaction between inattention and hyperactivity was not significant. We tested the two-way interactions between inattention and each confounding variable and between hyperactivity and each confounding variable. These interactions were tested for the following two reasons: to determine whether the role of inattention was conditioned by personal or sociofamilial moderators and to determine whether the role of hyperactivity was significant for subgroups of children. No term of interaction added to the model fit except between hyperactivity and residential move (Wald test: p=0.05), but this result should be interpreted with caution given the number of tested interactions.
Complementary Analyses
To test for the possibility that results varied depending on the statistical procedure used, we employed complete data sets without imputation alongside joint trajectories of inattention and hyperactivity and averaged scores instead of trajectories. Lastly, only the first wave of data on a larger sample was used. In all cases, inattention was highly significant but not hyperactivity. Further details regarding these analyses are presented in the data supplement.
Discussion
The aim of the present study was to assess the differential predictive power of inattention and hyperactivity problems during elementary school for educational attainment in young adulthood (22–23 years of age). We found that inattention strongly predicted high school graduation by early adulthood, with no additional or interactive contribution of hyperactivity. To the best of our knowledge, this is the first study to estimate the respective longitudinal contribution of both dimensions in a population sample and the first to do so in early adulthood, with complete official records of high school graduation and while controlling for meaningful variables.
Because hyperactivity and inattention assessments were available from teachers at yearly intervals, beginning in kindergarten and throughout elementary school, we were able to trace the developmental trajectories of these mental health symptoms over a 7-year period and use them as predictors of high school graduation in early adulthood. We expected that using 7 years of assessment by independent teachers who interacted daily with the children over more than 6 months would provide a better estimation of the long-term association between hyperactivity, inattention, and school attainment than ratings or diagnoses at one or two points in time. Predictive analyses indicated that inattention trajectories were a strong predictor of school attainment, even after controlling for meaningful variables. Hyperactivity trajectories were not significantly associated with high school graduation when inattention was included in the analysis. Children in the trajectory of high inattention from kindergarten to age 12 years (16.8%) had the highest risk of not having obtained a high school diploma by age 22–23 years, with 70.8% not graduating. Conversely, children in the trajectory of low inattention (46.3%) had the lowest risk, with only 11.5% not graduating, while those in the increasing and decreasing trajectories had intermediate risks.
Our results clearly indicate that inattention is a strong predictor of high school graduation, whereas hyperactivity is not. Hence, associations between ADHD symptoms and school attainment reported in previous studies (
1,
2) are probably mainly the result of the inattentive component of the diagnosis or the rating scale. The hyperactivity component played neither an additive nor interactive role in the present study. Also supporting our finding of a main effect of inattention on high school graduation is the fact that when joint trajectories were examined, participants with a high trajectory for both inattention and hyperactivity were not at higher risk to not graduate from high school than participants with a high trajectory for inattention alone. Additionally, participants with a high trajectory only for hyperactivity were not at higher risk than the contrast group. Hyperactivity is more salient to the teacher, whereas inattentiveness is often missed, making hyperactive children more likely to be referred for preventive and corrective support. Our results suggest the need to differentiate inattention from hyperactivity and use inattention as a major focus of preventive and corrective interventions.
Our results also suggest that attention problems could be identified and addressed before entry into primary school. Experiments have shown that preschool children can substantially benefit from preventive interventions targeting attention problems (
33). However, the increasing and decreasing trajectories of inattention during the elementary school years suggest that interventions during this later period could decrease the number of children in the increasing trajectory and possibly prevent the increasing trajectory. Studies are needed to understand the mechanisms that underlie the increasing and decreasing trajectories. Our results suggest that time-varying covariates, such as changes in the family, might alter the direction of the inattention trajectory. This may also be the case for changes in school organizational settings (
34).
The present results clearly suggest that inattention on its own is conducive to later educational underachievement, irrespective of the presence of hyperactivity symptoms. Therefore, these results support the new developments under discussion for DSM-5 to introduce a restrictive, predominantly inattentive subtype with limited presence of hyperactivity symptoms or to offer a new stand-alone diagnosis of attention deficit disorder. Both of these options would have the heuristic value of promoting research on the precursors and consequences of inattention and could pave the way to consideration of a broader range of inattention symptoms that were excluded from DSM-IV (
35).
Strengths and Limitations
This study is the first to use data on developmental trajectories (and joint trajectories) of both inattention and hyperactivity in children from kindergarten to the end of elementary school. The use of a population sample, official records of high school graduation available for all participants, and a range of meaningful confounding variables provide additional strengths.
Although teachers seem more reliable than parents in the diagnosis of ADHD and its subtypes (
36,
37), their assessment could be biased by a general negative halo effect. However, the fact that both dimensions had a differentiated effect on educational attainment suggests that any such halo effect was limited. Teachers may have rated behaviors for several children, yielding a lack of independence of assessments. However, given the study design based on sampling of individual children, only a few children may have shared the same teacher, with a change in clustering each year. We were unable to model this complex effect. Additionally, the instrument used includes few items for the key predictors. However, it has proven to be predictive of a range of adult and adolescent outcomes in numerous studies, and our predictive results were based on seven repeated assessments over a 7-year period according to different raters at each time point. Lastly, an assessor bias is possible because teachers who know that their students have poorer academic performance may tend to give these students higher ratings in inattention symptoms, and school performance is highly correlated with educational attainment. Clinical and/or laboratory assessments of inattention by assessors who are blind to school performance are needed.
Acknowledgments
The authors thank the participants, their families, and their teachers for long-term commitment to this study. The authors also thank Xuecheng Liu and Alain Girard, for statistical expertise; Hélène Beaumont; the many research assistants; and the staff of the Research Unit on Children's Psychosocial Maladjustment, for assistance with data collection and administration.