As a growing number of states are legalizing medicinal and recreational marijuana use, it is increasingly important to understand the consequences that regular use may have on physical and mental health. One area of particular concern is the effect that adolescent marijuana use may have on the development of psychotic symptoms (e.g., hallucinations, paranoia). Multiple longitudinal and cross-sectional studies have reported that marijuana use, particularly during adolescence, is related to acute psychotic episodes and future psychotic disorders (
1–
4). More recent research suggests that regular marijuana use might increase adolescents’ risk for developing a psychotic illness by causing them to experience persistent subclinical psychotic symptoms, which are typically transitory and fairly common during adolescence (
5). However, we are not aware of any published longitudinal studies that have examined whether adolescents who regularly use marijuana (i.e., weekly or more often) over several years exhibit a systematic increase in their subclinical psychotic symptoms that persists during periods of sustained abstinence.
One critical issue is to determine whether a prior history of regular marijuana use, independent of current use, increases an adolescent’s risk for experiencing persistent psychotic symptoms. Experimental administration of the primary psychoactive chemical in marijuana, tetrahydrocannabinol (THC), can cause acute feelings of paranoia and other features of psychosis in healthy volunteers (
6–
9), but these symptoms largely subside when acute intoxication wanes (
10). Many negative effects of adolescent marijuana use on cognitive functioning also tend to dissipate following a few months of abstinence (
11). Nearly all prior longitudinal studies examining the association between marijuana use and future psychotic symptoms have not controlled for recent patterns of use (
12–
17), have not repeatedly assessed marijuana use across adolescence, or have combined prior and recent use (
18). Therefore, it is impossible to delineate the enduring effect that regular use has on emergent psychotic symptoms and whether this effect is sustained when individuals remain abstinent for several months.
A second issue is whether the association between adolescent marijuana use and later psychotic symptoms is causal or a function of confounding factors (
19–
23). Together, prior studies have collectively controlled for approximately 60 confounding factors (e.g., other substance use, mental health problems), with estimates suggesting that these factors account for nearly half of the association between marijuana use and psychosis (
3). Although no single study can accurately, comprehensively, and directly quantify the myriad preexisting individual differences that may explain the linkage between marijuana use and psychosis, it is possible to eliminate these factors as potential confounds by using within-individual change models. By examining the association between changes in marijuana use and psychotic symptoms within individuals over time, all preexisting time-stable differences between individuals (whether measured or not) are eliminated as potential confounds (
24). Moreover, only within-individual change models can address two key questions regarding the association between adolescent marijuana use and psychotic symptoms: 1) During periods of regular marijuana use, do adolescents experience an increase in their psychotic symptoms (concurrent effect)? and 2) Do adolescents who engage in regular marijuana use across multiple years exhibit an incremental and sustained increase in their psychotic symptoms that remains even during periods of abstinence (cumulative/sustained effect)?
Findings from, to our knowledge, the only published longitudinal study that has examined the association between within-individual changes in marijuana use and subclinical psychotic symptoms indicated that adolescents experienced a significant increase in their psychotic symptoms during years when they increased their marijuana use; however, whether this increase was short-lived or persisted across multiple years was not examined (
25).
The direction of any causal association between marijuana use and psychotic symptoms is also debated. For example, the self-medication hypothesis suggests that adolescents may begin engaging in regular marijuana use as a way to cope with prodromal psychotic symptoms. Studies directly examining the self-medication hypothesis have produced mixed findings. Fergusson and colleagues (
25) found that within-individual increases in subclinical psychotic symptoms were unrelated to concurrent changes in adolescent marijuana use after controlling for several time-varying confounds. In contrast, another longitudinal study found evidence of a bidirectional association between psychosis vulnerability and marijuana use in adolescence (
26).
The present study was designed to address several key issues regarding the association between adolescent marijuana use and subclinical psychotic symptoms. Using within-individual change modeling, analyses examined whether adolescents experienced a systematic increase in their subclinical psychotic symptoms during periods when they used marijuana regularly (concurrent effect) and whether this increase persisted over time, even during periods of sustained abstinence (cumulative/sustained effect). These effects were further examined for different features of psychosis (e.g., paranoia, hallucinations, bizarre behavior). Analyses controlled for all time-stable factors and several potential time-varying confounds (e.g., other substance use, externalizing and internalizing problems). The possibility of reverse causation was also tested by examining whether increases in subclinical psychotic symptoms predicted current and/or sustained increases in regular marijuana use.
Method
Participants and Procedures
The participants were 1,009 boys (55.1% black, 41.1% white, 3.8% other) who were recruited from a list of students enrolled in the 1st and 7th grades (referred to as the youngest and oldest cohorts, respectively) in Pittsburgh public schools in 1987–1988. Students enrolled in classes for severe intellectual and physical disabilities were not eligible for the study. A random sample of boys enrolled in each grade was selected for a multi-informant (parents, teachers, self-report) screening to assess conduct problems (e.g., fighting, stealing). Parental consent rates for the screening were 84.6% (N=849) and 83.9% (N=855) for the youngest and oldest cohorts, respectively. Boys who scored in the upper 30th percentile on the screener within each grade were selected for longitudinal follow-up (youngest cohort: N=256; oldest cohort: N=257), along with an approximately equal number of boys who were randomly selected from those scoring below the 70th percentile (youngest: N=247; oldest: N=249). At screening, boys in the youngest cohort (age: mean=6.96 years, SD=0.55) and oldest cohort (age: mean=13.38 years, SD=0.79) were predominantly living with their biological mother (95% and 92%, respectively), and approximately half had a biological father living in the home (42% and 44%, respectively). In both the youngest and oldest cohorts, approximately one-fifth of the mothers (20.6% and 22.8%, respectively) and fathers (16.9% and 23.3%, respectively) living in the home had not graduated from high school. The proportion of families with no employed parental figure in the oldest and youngest cohorts was 14.5% and 12.0%, respectively. Boys in the follow-up sample were not significantly different from the screening sample in terms of race, family composition, and parental education and employment (
27).
Following screening, the boys in the youngest cohort were interviewed every 6 months for 4 years, followed by nine annual assessments and follow-ups when participants were, on average, ages 26 and 29. Following screening, the boys in the oldest cohort were assessed every 6 months for 30 months, then annually for 10 years, and again when they were, on average, age 36. For this analysis, data from the two cohorts were combined by aligning assessments by participant age at the time of the interview, resulting in overlapping annual assessments from age 13 to 18. We focused on this age range because 1) the last annual assessment for participants in the 1st-grade cohort was conducted when they were approximately 18 years old and 2) prior studies have suggested that regular marijuana use during adolescence is most strongly associated with psychotic symptoms and other forms of cognitive impairment (
1,
3,
12,
28). Further details about the sample and study methods are available elsewhere (
27).
Measures
Regular marijuana use.
Marijuana use was assessed with the youth-reported Substance Use Questionnaire (
29). At each annual assessment, the participants reported the number of days they used marijuana in the past year. Adjacent 6-month assessments for the oldest cohort were summed to index past year use. A binary variable, created at each age to index at least weekly marijuana use (i.e., ≥52 times), was used given evidence suggesting that weekly use before age 18 might be associated with longer-term impairments in cognitive functioning (
28). A cumulative history of marijuana use was indexed at each age by counting the number of prior years participants reported weekly use. Cumulative years of weekly use was truncated at 2 years because only 3.7 % of participants had 3 or more years of prior weekly use by age 18.
Subclinical psychotic symptoms.
Five items from the Youth Self Report (
30) were used to index subclinical psychotic symptoms in the past year at each age. As in prior studies, a symptom was considered present if a youth rated it as “sometimes true” or “very true” (
31). The items indexed feelings of paranoia (“You feel that others are out to get you”), hallucinations (“You see things that nobody else seems able to see,” “You hear things that nobody else seems able to hear”), and bizarre thinking (“You have thoughts that other people would think are strange,” “You do things that other people think are strange”). A count of past-year subclinical psychotic symptoms was calculated for each age, as well as three binary variables indexing whether participants experienced each symptom subtype (i.e., paranoia, hallucinations, bizarre thinking). Longitudinal evidence indicates that adolescents who endorse experiencing these subclinical symptoms are at increased risk for developing a psychotic disorder later in life (
32).
Time-Varying Covariates
Prior subclinical psychotic symptoms (T−1).
Psychotic symptoms at the prior assessment wave (T−1) were included as covariates. For total psychotic symptoms, the number of symptoms at T−1 was truncated at 2 (i.e., upper 9%−20% at each age). For analyses involving symptom subtypes, binary items indexing the presence/absence of the symptom at T−1 were used.
Other substance use.
The Substance Use Questionnaire was used to assess the number of days participants used alcohol, tobacco, and other illicit drugs (tranquilizers, barbiturates, or codeine without prescription; other prescription drugs without prescription; amphetamines; hallucinogens; cocaine; crack; heroin; PCP) in the past year. As with marijuana use, alcohol use was dichotomized to index at least weekly use (≥52 days). Tobacco use was dichotomized to index near daily or daily use (≥312 days). Other illicit drug use was dichotomized to index use or nonuse due to the low prevalence at each age (i.e., 2%−6%). Variables indexing a prior history of use were created for each age by summing the number of prior years of weekly alcohol use (truncated at 2; 3.7% used weekly for 3 or more years by age 18), daily tobacco use (truncated at 3; 5.7% used daily for 4 or more years by age 18), and other illicit drug use (truncated at 1; 4.0% used for 2 or more years by age 18).
Internalizing and externalizing problems.
The extensively validated internalizing and externalizing problems scales from the Youth Self Report were used to control for fluctuations in other forms of psychopathology (
33). Participants rated items using a 3-point scale (0=not true to 2=very true/often true), and items were summed to generate scores for internalizing problems (34 items) and externalizing problems (34 items). The item “You feel that others are out to get you” was excluded from the internalizing scale because it was used as an index of paranoia.
Data Analysis Plan
Fixed-effects regressions in Stata 13.1 (
34) were used to examine the within-individual association between changes in weekly marijuana use and psychotic symptoms between ages 13 and 18. Because these models focus exclusively on modeling within-individual change, all time-stable factors that may vary between individuals are ruled out as potential confounds (
24). Poisson fixed-effects regression models (for total subclinical symptoms) and logistic fixed-effects regression models (for binary symptom subtypes) were used. Incidence rate ratios are reported for total symptoms, and odds ratios are reported for symptom subtypes. A series of three models were run for each outcome (for the formulas, see Table S1 in the
data supplement accompanying the online version of this article). The base model examined the effects of current weekly marijuana use and prior years of weekly marijuana use on subclinical psychotic symptoms, after controlling for age-related changes in subclinical psychotic symptoms. Next, all time-varying covariates were added to the model to control for potential confounds (i.e., psychotic symptoms at T−1, current internalizing and externalizing problems, current and prior use of tobacco, alcohol, and illicit drugs). In the final model, the number of years of prior marijuana use was subdivided into two orthogonal variables to delineate the impact of prior use on subsequent subclinical psychotic symptoms during years when adolescents reported no marijuana use versus years when they reported some use. This model tested whether the cumulative effect of prior marijuana use dissipated or remained significant during subsequent periods of year-long abstinence.
To examine the possibility of reverse causation, logistic fixed-effects regressions examined whether changes in current and prior subclinical psychotic symptoms predicted changes in weekly marijuana use. A variable indexing a cumulative history of subclinical psychotic symptoms was created by counting the number of prior years with 2 or more subclinical symptoms (truncated at 2; 7.9% had 3 or more years with 2 or more symptoms). The same covariates were included in these models, except that reports of prior use of tobacco, alcohol, and hard drugs were not included as covariates, and marijuana use at the preceding assessment (T−1) was included.
Missing Data
The models were run by using conditional maximum likelihood estimation, which uses all available information in a time series to generate model parameters rather than resorting to complete case analysis. The parameters are unbiased when data in a time series are missing at random (
35), meaning the probability that the dependent variable Y is missing is not associated with the value of Y after controlling for all observed covariates (
24).
Sample retention at the measurement occasions used in the present study ranged from 83% to 99%. Of the original 1,009 participants, 69.6% (N=702) had no missing data, 14.4% (N=145) were missing 1 year of data, 5.0% were missing 2 years (N=50), 4.8% were missing 3 years (N=48), 2.8% were missing 4 years (N=28), 1.6% were missing 5 years (N=16), and 2.0% were missing all 6 years (N=20). Compared with participants with complete data, individuals with missing data were more likely to be black and to have higher levels of subclinical psychotic symptoms, internalizing problems, and externalizing problems. However, these variables were only weakly associated with missingness (r values from 0.07 to 0.19), suggesting that any deviation from the missing-at-random assumption was likely minor.
Results
Descriptive Statistics
Table 1 contains descriptive statistics for substance use and subclinical psychotic symptoms by age. Between ages 13 and 18, the prevalence of psychotic symptoms gradually declined. By the last assessment, 695 participants had reported at least one subclinical psychotic symptom, 391 had reported paranoia, 231 had reported hallucinations, and 574 had reported bizarre thinking.
As expected, substance use increased from age 13 to 18. By the last assessment, 270 participants had used marijuana weekly, 325 had used alcohol weekly, 377 had used tobacco daily, and 134 had used other illicit drugs at least once. The average age at onset was 16.1 years (SD=1.6) for weekly marijuana use, 16.3 (SD=1.6) for weekly alcohol use, 15.6 (SD=1.7) for daily tobacco use, and 15.7 (SD=1.7) for any other illicit drug use.
Predicting Changes in Subclinical Psychotic Symptoms
The primary results for total subclinical psychotic symptoms and symptom subtypes are presented in
Table 2 and
Table 3, respectively. Sample sizes for these analyses vary because participants with no variation in the dependent variable (i.e., no within-individual change) are excluded by default from Poisson and logistic fixed-effects models (
24). Findings related to significant model covariates are included in Table S2 in the
online data supplement.
Changes in current weekly marijuana use and the number of prior years of weekly use were both significantly associated with increases in total number of subclinical psychotic symptoms before covariate adjustment (
Table 2). However, only the cumulative effect of prior weekly marijuana use remained significant after controlling for all time-varying covariates. In the model with covariates, linear trend analysis indicated that for each additional year adolescents engaged in weekly marijuana use, their expected number of subsequent psychotic symptoms rose by 21%.
Models examining specific symptom subtypes indicated that current weekly use and the number of prior years of weekly marijuana use were both significantly associated with paranoia, before and after controlling for time-varying covariates (
Table 3). Linear trend analysis in the model with covariates indicated that for each additional year adolescents engaged in weekly marijuana use, their predicted odds of experiencing subsequent paranoia rose by 133%. Similarly, the number of prior years adolescents engaged in weekly marijuana use was significantly associated with subclinical hallucinations, although the effect of current weekly marijuana use was not significant (
Table 3). Linear trend analysis in the model with covariates indicated that for each additional year adolescents engaged in weekly marijuana use, their expected odds of experiencing future hallucinations rose by 92%. Current and prior marijuana use were not associated with changes in bizarre thinking (
Table 3).
Cumulative Effect of Weekly Marijuana Use Following Abstinence
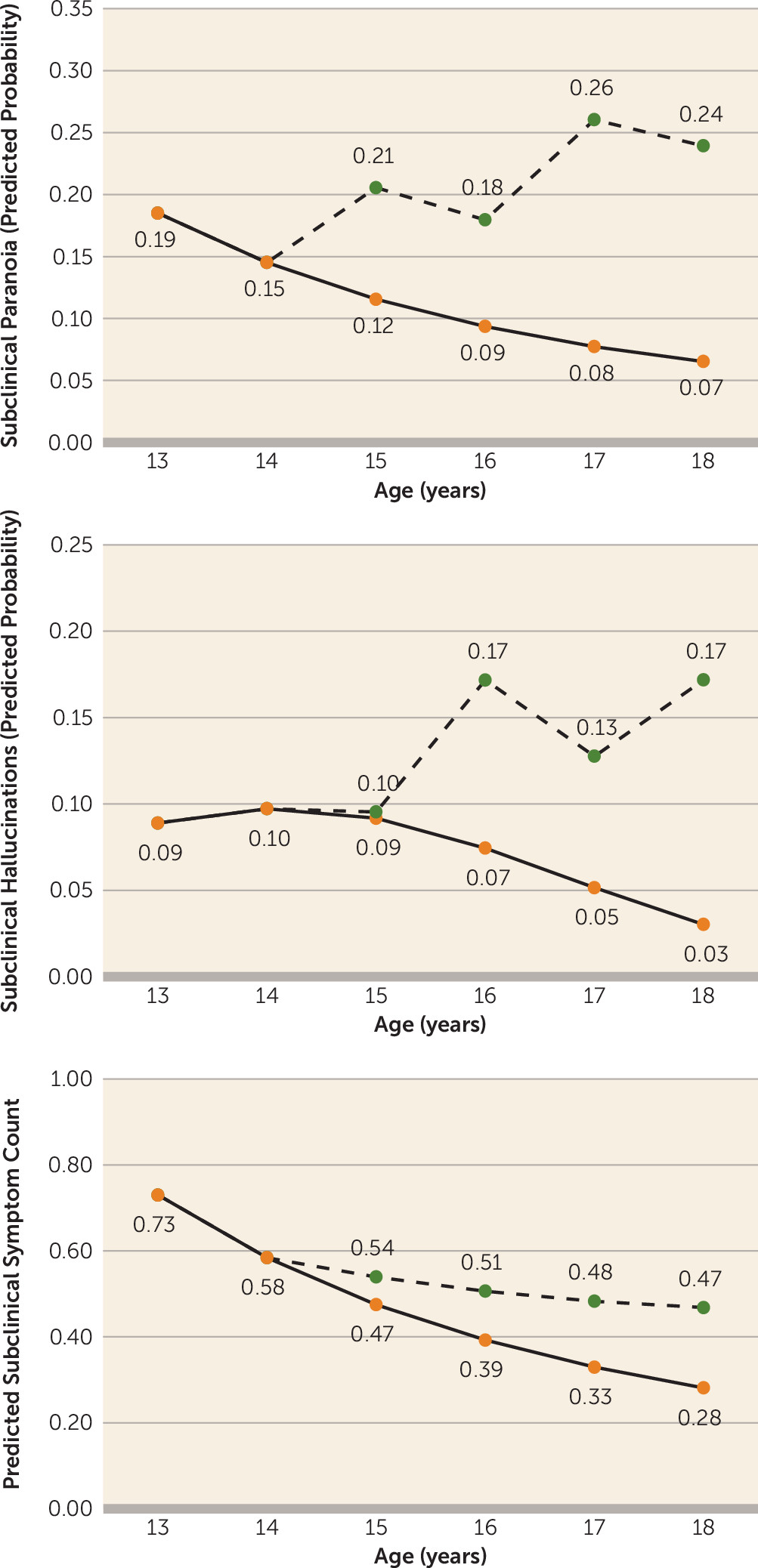
The results indicate that the linear effect of the number of prior years of weekly marijuana use on total subclinical psychotic symptoms, paranoia, and hallucinations persisted even when adolescents stopped using marijuana for a year (
Table 4,
Figure 1). The results from the model with covariates indicate that for each additional year adolescents engaged in weekly marijuana use, their expected number of total subclinical psychotic symptoms rose by 29% during subsequent periods of year-long abstinence, and their expected odds of experiencing paranoia and hallucinations rose by 112% and 158%, respectively.
Potential Reverse Causation
Models examining whether changes in current and prior psychotic symptoms predicted changes in weekly marijuana use are presented in Table S3 in the online data supplement. After controlling for time-varying covariates, changes in prior and current psychotic symptoms did not predict increases in weekly marijuana use. Instead, there was some indication that prior psychotic symptoms were associated with a reduced likelihood of engaging in weekly marijuana use.
Discussion
This study found evidence suggesting that regular marijuana use may increase an adolescent’s risk of experiencing persistent subclinical psychotic symptoms. This association remained significant after the models controlled for all stable between-individual factors and within-individual changes in current marijuana use, current and prior use of tobacco, alcohol, and other illicit drugs, and internalizing and externalizing problems. Importantly, the effect of prior weekly marijuana use on subclinical psychotic symptoms did not dissipate when adolescents remained abstinent for a year. Moreover, no support was found for the self-medication hypothesis; adolescents were not more likely to engage in regular marijuana use following an increase in their psychotic symptoms. The cumulative effect of regular marijuana use was most pronounced for subclinical symptoms of paranoia and hallucinations.
Transient Versus Sustained Effect of Regular Marijuana Use
Consistent with findings in prior studies, the prevalence of subclinical psychotic symptoms tended to decrease from early to late adolescence (
36–
39). Despite this normative developmental decline, our findings indicate that regular marijuana use increases the likelihood that teens will experience persistent subclinical psychotic symptoms across adolescence, particularly paranoia. These findings build on experimental work showing that acute administration of THC can cause paranoia among healthy adult volunteers in laboratory settings (
10). Although feelings of paranoia typically subside within 24 hours in experimental studies, our findings suggest that as adolescents regularly use marijuana over multiple years, their odds of experiencing chronic paranoia increase. More concerning, evidence suggests that this effect persists even when adolescents abstain from using marijuana for 1 year. A cumulative history of regular marijuana use also increased adolescents’ risk of experiencing subclinical hallucinations, which also persisted during periods of year-long abstinence. This effect is particularly concerning as evidence suggests that adolescents who report chronic subclinical hallucinations are at heightened risk for developing psychotic disorders by young adulthood (
31).
Current and cumulative marijuana use were not associated with an increase in strange thoughts or behaviors. The prevalence of these symptoms was fairly high in the current sample, with approximately one-third of participants reporting some odd thinking or behavior at age 13. This finding might reflect the fact that participants were asked to indicate whether “others” viewed their thoughts or behaviors as strange. During adolescence, many youths may feel misunderstood by parents and other authority figures as they begin establishing their autonomy. As a result, endorsement of these items may be more indicative of a normative individuation process than emergent psychopathology.
Accounting for Potential Confounds
An area of contentious debate is whether the well-established link between adolescent marijuana use and features of psychosis is due to pre-existing individual differences (
19–
23). By focusing on the association between changes in marijuana use and changes in subclinical psychotic symptoms within individuals, the current study eliminated all preexisting time-stable individual differences as potential confounds. In these models, for example, a genetic predisposition toward schizophrenia cannot directly explain why an adolescent’s psychotic symptoms fluctuate from year to year (within-individual change), although it may explain why some people are more likely than others to develop psychotic symptoms when exposed to environmental risk factors (between-individual differences). Furthermore, by including a series of time-varying confounding variables in the analysis, the findings indicate that this association was not accounted for by recent and cumulative changes in other substance use. In fact, during periods when adolescents used other substances, they did not experience an increase in subclinical psychotic symptoms. The unique linkage between regular marijuana use and increases in adolescents’ subclinical psychotic symptoms was further exemplified by the fact that the significant associations remained after the models controlled for changes in other forms of psychopathology.
Accounting for Potential Reverse Causation
Consistent with prior work, the present study also found no evidence supporting a possible reverse causal pathway model (
14,
25). After controlling for several time-varying covariates, the results indicated that adolescents were not more likely to engage in weekly marijuana use during years when their subclinical psychotic symptoms increased. Furthermore, no consistent evidence supported a systematic association between a cumulative history of psychotic symptoms and an increased risk for engaging in weekly marijuana use.
Limitations and Future Directions
The findings presented here must be considered in the context of several limitations. First, the findings were based on a longitudinal sample of urban boys followed between ages 13 and 18 in one geographical area. Future research should investigate whether these findings hold for girls and adults living in geographically diverse locales and whether the effect of regular adolescent marijuana use on subclinical psychotic symptoms persists into adulthood.
It is also important to note that this study investigated subclinical symptoms by using a self-report rating scale. Although evidence suggests that adolescents who report experiencing subclinical symptoms are at a heightened risk for developing psychotic disorders later in life (
31,
32,
36), these symptoms are transient for many youths and may reflect accurate appraisals of reality rather than cognitive distortions. Consistent with this notion, data collected on participants at follow-up assessments in adulthood indicated that only 2.3% of participants in the current study had developed a psychotic disorder by their late 20s or early 30s (
Table 5). Although adolescents who engaged in heavy marijuana use across multiple years and those who experienced chronic paranoia and hallucinations were at significantly greater risk for developing a psychotic disorder, this adverse outcome occurred for only a small proportion of these participants and other between-individual difference factors may account for these associations (
Table 5). It will be important for future studies with much larger samples to examine why only a subset of adolescents who engage in regular marijuana use develop chronic subclinical psychotic symptoms, why an even smaller portion develop psychotic disorders, and whether these linkages remain significant after controlling for potential confounding factors.
Another limitation is that only self-reported frequency of marijuana use was assessed in the present study. Other factors, such as THC potency and mode of administration, may affect the association between marijuana use and psychotic symptoms. Given that the data presented here were collected in the mid-1990s and early 2000s and that the THC concentration in marijuana has increased in recent years (
41), our analysis might underestimate the risks associated with regular use. Future research should investigate how potent marijuana concentrates that can be vaporized, inhaled, or eaten may affect current and future psychotic symptoms. Future experimental research should also investigate whether reducing the proportion of THC (and increasing the proportion of cannabidiol) in medical and recreational marijuana may reduce the risk of experiencing subclinical psychotic symptoms.
Conclusions
This study demonstrates that adolescents are more likely to experience subclinical psychotic symptoms (particularly paranoia) during and after years of regular marijuana use. Perhaps the most concerning finding is that the effect of prior weekly marijuana use persists even after adolescents have stopped using for 1 year. For every additional year adolescents engage in regular marijuana use, their risk of exhibiting subclinical paranoia and hallucinations in future years increases in a linear manner, and the effect of cumulative use remains significant even during periods of abstinence lasting a year. Given the recent proliferation of marijuana legalization across the country, it will be important to enact preventive policies and programs to keep adolescents from engaging in regular marijuana use, as chronic use seems to increase their risk of developing persistent subclinical psychotic symptoms.