Randomized Clinical Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disorder: Effects on Symptoms and Autobiographical Memory Recall
Publication: American Journal of Psychiatry
Abstract
Objective:
Patients with depression show blunted amygdala hemodynamic activity to positive stimuli, including autobiographical memories. The authors examined the therapeutic efficacy of real-time functional MRI neurofeedback (rtfMRI-nf) training aimed at increasing the amygdala’s hemodynamic response to positive memories in patients with depression.
Method:
In a double-blind, placebo-controlled, randomized clinical trial, unmedicated adults with depression (N=36) were randomly assigned to receive two sessions of rtfMRI-nf either from the amygdala (N=19) or from a parietal control region not involved in emotional processing (N=17). Clinical scores and autobiographical memory performance were assessed at baseline and 1 week after the final rtfMRI-nf session. The primary outcome measure was change in score on the Montgomery-Åsberg Depression Rating Scale (MADRS), and the main analytic approach consisted of a linear mixed-model analysis.
Results:
In participants in the experimental group, the hemodynamic response in the amygdala increased relative to their own baseline and to the control group. Twelve participants in the amygdala rtfMRI-nf group, compared with only two in the control group, had a >50% decrease in MADRS score. Six participants in the experimental group, compared with one in the control group, met conventional criteria for remission at study end, resulting in a number needed to treat of 4. In participants receiving amygdala rtfMRI-nf, the percent of positive specific memories recalled increased relative to baseline and to the control group.
Conclusions:
rtfMRI-nf training to increase the amygdala hemodynamic response to positive memories significantly decreased depressive symptoms and increased the percent of specific memories recalled on an autobiographical memory test. These data support a role of the amygdala in recovery from depression.
Depression is a common and disabling condition (1). With approximately two-thirds of patients not responding fully to treatment (2), investigation into novel therapeutic approaches is warranted. One novel approach is real-time functional MRI neurofeedback (rtfMRI-nf), in which an individual receives information about the blood-oxygen-level-dependent (BOLD) signal from their brain in real time and learns to self-modulate this signal (3, 4). Emerging evidence suggests that rtfMRI-nf has clinical utility in chronic pain (5), smoking cessation (6), anxiety (7), and depression (8, 9). In the present study, we conducted a randomized clinical trial to test the therapeutic potential of rtfMRI-nf training to enhance the amygdala hemodynamic response to positive autobiographical memory recall for depression.
Research supports a critical role of the amygdala in emotional memory (10). While much attention has focused on the amygdala’s role in processing and responding to negative and fearful emotional stimuli (11), evidence indicates that the amygdala more generally influences the perceived salience of stimuli and events (12), and amygdala engagement appears to be critical for emotional processing and responding to both negative and positive stimuli (13), including autobiographical memories (14, 15). Furthermore, the amygdala has neuroanatomical connections with regions governing affective memory and emotion regulation, including the hippocampus, anterior cingulate, and orbitofrontal cortices (16, 17), and it has reciprocal functional connectivity with these regions during tasks involved in emotion regulation (18) and emotional memory recall (19).
The amygdala also plays a major role in the pathology of depression (20). In depressed participants, the amygdala response is “doubly dissociated” relative to the response in control subjects, showing exaggerated responses to negative stimuli and attenuated responses to positive stimuli (21, 22), including autobiographical memories (15). Furthermore, the amygdala’s response to positive stimuli correlates with symptom severity (15, 22) and reverts to the pattern seen in healthy individuals after antidepressant treatment (21) or cognitive-control therapy (23). The negative emotional processing bias in depressed individuals is manifested in memory and includes deficits in the recall of emotionally positive autobiographical memories (15, 24). These findings, taken together with evidence that the amygdala links the domains of affective experience/response and emotional memory recall, suggest that enhancing amygdala processing of positive stimuli via rtfMRI-nf has therapeutic potential for depressed individuals.
We previously showed rtfMRI-nf training to be feasible in enhancing amygdala response to positive memories in healthy (25) and depressed individuals (9). In depressed study participants, training increased state measures of happiness and decreased state measures of anxiety (9). In the present study, we aimed to extend these findings by adding a baseline run to confirm that amygdala activity is hypoactive in our depressed sample, a second rtfMRI-nf session to determine whether additional sessions are useful, and a 1-week follow-up to examine changes in clinical symptoms and determine whether changes persist beyond the neurofeedback sessions. Furthermore, we administered the Autobiographical Memory Test to determine whether amygdala rtfMRI-nf training can also improve memory recall in depressed participants, as impaired recall for specific positive memories constitutes an enduring cognitive deficit in depression (26, 27) that is unaltered by current treatments (28). Should amygdala rtfMRI-nf training result in clinical and memory improvements, this would suggest that changing amygdala reactivity during autobiographical memory recall has a role in recovery from depression.
Method
Participants
Thirty-six right-handed, unmedicated adults 18–55 years of age who met DSM-IV-TR criteria for major depressive disorder in a current major depressive episode participated. All participants were recruited from the community via general advertisements for studies at the Laureate Institute for Brain Research and underwent screening evaluations, including the Structured Clinical Interview for DSM-IV Axis I disorders. Exclusion criteria included current pregnancy, general MRI exclusions, serious suicidal ideation, psychosis, major medical or neurological disorders, exposure to any medication likely to influence cerebral function or blood flow within 3 weeks, and meeting DSM-IV criteria for drug or alcohol abuse within the previous year or for lifetime alcohol or drug dependence (excepting nicotine). All participants were naive to rtfMRI-nf.
Participants gave written informed consent to participate in the study and received financial compensation. The research protocol was approved by the Western Institutional Review Board and registered on ClinicalTrials.gov (the CONSORT diagram is available in the data supplement that accompanies the online edition of this article).
Procedure
Participants completed four study visits. During visit 1, participants completed the Beck Depression Inventory–II (BDI-II) and the Snaith-Hamilton Pleasure Scale (SHAPS) (29) and were rated on the Montgomery-Åsberg Depression Rating Scale (MADRS) (30), the 21-item Hamilton Depression Rating Scale (HAM-D), the Hamilton Anxiety Rating Scale (HAM-A), and the Autobiographical Memory Test (31). Between 5 and 7 days later, at visit 2, participants completed their first rtfMRI-nf session and the same clinical and self-report measures as on visit 1. One week later, at visit 3, participants completed their second rtfMRI-nf session and the same measures as on previous visits. Visit 4, which occurred 5–7 days after visit 3, consisted of the clinical and self-report measures and the Autobiographical Memory Test.
The Autobiographical Memory Test is a cued memory test in which participants are presented with cue words and instructed to recall one specific memory after each word. Our version of the test consisted of 18 cue words presented orally, with six each of neutral, positive, and negative valence (for additional task details, see the online data supplement ).
rtfMRI-nf Paradigm
Under double-blind conditions, participants were randomly assigned to receive rtfMRI-nf from one of two regions of interest defined as 7-mm spheres in Talairach space: the left amygdala (coordinates, −21, −5, −16) or the left horizontal segment of the intraparietal sulcus (coordinates, −42, −48, 48), a region putatively not involved in emotion regulation (32, 33). Participants were instructed to retrieve positive memories while attempting to increase the hemodynamic activity in the assigned region to that of a blue bar representing the target activation level. Each neurofeedback run consisted of alternating 40-second blocks of rest, happy memories (up-regulate condition; red bar shown), and count (backward from 300 by a given one-digit integer). Each rtfMRI-nf session consisted of eight fMRI runs, each lasting 8 minutes and 40 seconds: a resting run, a baseline run in which no neurofeedback information was provided, a practice run, three training runs, a final transfer run in which no neurofeedback information was provided, and a final rest run. (For more detail on the paradigm and imaging parameters, see the online data supplement .)
Imaging was conducted using a GE Discovery MR750 whole-body 3-T scanner equipped with a custom rtfMRI neurofeedback system (25, 34). The neurofeedback signal for each happy memory condition was computed as the fMRI percent signal change relative to the average fMRI signal for the preceding rest block, updated every 2 seconds and displayed as a red bar. To reduce bar fluctuations due to noise in the fMRI signal, the bar height was computed at every time point as a moving average of the current and two preceding values. These percent signal change values were averaged over each run and used as a performance measure.
Neurofeedback success was defined as the mean percent signal change in the region of interest from the baseline run at visit 2 to the final transfer run at visit 3. Higher scores indicate more activity after training relative to baseline (see Figure S3 in the data supplement ).
An exploratory whole-brain analysis was performed to determine which regions showed a significant change in hemodynamic activity from the baseline run to the final transfer run in the experimental relative to the control group (see the data supplement ).
Behavioral Data Analysis
SPSS, version 23 (IBM Corp., Armonk, N.Y.) was used for statistical analysis. To compare groups on baseline characteristics, independent-samples t tests and Fisher’s exact tests were performed. Change in MADRS score was used as the primary outcome measure, as the MADRS includes a higher proportion of items reflecting emotional processing than the HAM-D (35, 36). To examine change in MADRS score, a linear mixed-effects model with the fixed factors of visit (visits 1, 2, 3, 4) and group (experimental, control) was used. The neurofeedback training effect was evaluated via a linear mixed-effects model with the fixed factors of run (baseline, practice, run 1, run 2, run 3, transfer), visit (visits 2, 3), region of interest (amygdala, intraparietal), and group (experimental, control) for regional percent signal change. For autobiographical memory performance, a mixed-effects model was used with the fixed factors of visit (visits 1, 4), type (specific, categorical, extended, semantic), valence (positive, negative), and group (experimental, control). In all cases, autocorrelations were modeled with the covariance structure that minimized the Akaike information criterion, with participant as the random effect. Associated t tests were performed to characterize significant differences underlying main effects and interactions. Association between neurofeedback success, change in autobiographical memory performance, and change in MADRS score was determined via linear regression using the unstandardized residuals calculated from the final score with the influence of the baseline score regressed out.
Results
Demographic and Clinical Characteristics
One participant in each group withdrew from the study because of physical discomfort during imaging, and data from one participant in the control group were excluded because of excessive head motion (the removal threshold was >3 mm displacement, and this participant averaged 12 mm), leaving a final sample of 18 experimental and 15 control participants.
At pretreatment visit 1 (Table 1; see also Table S1 in the data supplement ), the groups did not differ significantly in mean age, time since last antidepressant medication, length of current depressive episode, or scores on the BDI-II, SHAPS, MADRS, HAM-D, or HAM-A. A Fisher’s exact test revealed no significant difference between groups in the proportion of females, number of major depressive episodes experienced, or number of previous antidepressant medications. Average depression scores were in the moderate severity range. Three-quarters of participants were chronically depressed, and more than half had previously received antidepressant pharmacotherapy.
| Visit 1: Baseline | Visit 2: rtfMRI-nf | Visit 3: rtfMRI-nf | Visit 4: Follow-Up | |||||
|---|---|---|---|---|---|---|---|---|
| Measure and Group | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Montgomery-Åsberg Depression Rating Scale | ||||||||
| Experimental group | 23.5 | 9.9 | 22.5 | 10.2 | 14.4a | 9.8 | 11.9a | 9.0 |
| Control group | 23.8 | 6.7 | 22.5 | 7.8 | 22.6b | 8.4 | 21.9b | 8.1 |
| Hamilton Depression Rating Scale (21 item) | ||||||||
| Experimental group | 19.4 | 7.9 | 19.1 | 8.2 | 12.8a | 7.5 | 10.4a | 7.1 |
| Control group | 19.1 | 4.4 | 19.3 | 5.6 | 17.2b | 5.8 | 17.2b | 5.0 |
| Hamilton Anxiety Rating Scale | ||||||||
| Experimental group | 18.8 | 7.5 | 16.9 | 9.5 | 14.1a | 8.2 | 12.3a | 7.7 |
| Control group | 18.1 | 6.3 | 17.1 | 6.6 | 16.8 | 7.3 | 13.9a | 7.5 |
| Beck Depression Inventory–II | ||||||||
| Experimental group | 27.2 | 10.7 | 26.8 | 11.1 | 18.4a | 9.3 | 16.1a | 9.7 |
| Control group | 26.6 | 13.4 | 25.8 | 13.1 | 25.3b | 12.2 | 24.3b | 12.3 |
| Snaith-Hamilton Pleasure Scale | ||||||||
| Experimental group | 31.3 | 5.6 | 39.2 | 7.4 | 27.6a | 7.5 | 25.6a | 7.9 |
| Control group | 32.3 | 5.1 | 32.6 | 8.8 | 31.9 | 7.3 | 31.1b | 6.9 |
a
Significant difference from baseline, p<0.05.
b
Significant difference from the experimental group, p<0.05.
Paired-sample t tests within each group were used to examine whether scores significantly changed from visit 1 to visit 4. In the experimental group, all ratings significantly decreased from visit 1 (MADRS: t=7.70, df=17, p<0.001, d=1.22; BDI-II: t=4.70, df=17, p<0.001, d=1.09; HAM-A: t=5.61, df=17, p<0.001, d=1.04; SHAPS: t=2.67, df=17, p=0.01, d=0.54). In the control group, HAM-A score decreased significantly from visit 1 (t=2.60, df=14, p=0.02, d=0.89), while the other ratings did not change significantly.
A linear mixed model using the Toeplitz covariance structure revealed a significant group-by-visit interaction (F values, >12.0; df=3, 53; p values, <0.001). As stated above, the groups did not differ significantly from each other in any score at visit 1; scores also did not differ between groups at visit 2. The experimental group had lower scores than the control group on the MADRS, BDI-II, and HAM-D at visit 3 (MADRS: t=1.61, df=32, p=0.01, d=0.90; BDI-II: t=2.06, df=32, p=0.04, d=0.71; HAM-D: t=2.61, df=32, p=0.01, d=0.66) and visit 4 (MADRS: t=3.40, df=32, p<0.001, d=1.17; BDI-II: t=2.17, df=32, p=0.03, d=0.74; HAM-D: t=2.64, df=32, p=0.01, d=0.92). SHAPS scores did not differ significantly between groups at visit 3 but were lower in the experimental group relative to the control group at visit 4 (t=3.40, df=32, p=0.002, d=0.54). HAM-A scores did not differ significantly between groups at any visit.
Twelve participants in the experimental group responded to neurofeedback (at least a 50% decrease in MADRS score), compared with two participants in the control group. Six participants in the experimental group and one in the control group met criteria for remission at study end (MADRS score <10), making a number needed to treat, assuming all dropouts were nonresponders, of 4 (95% CI=2, 50).
Neurofeedback Performance
For the linear mixed model using the ARMA1 (autoregressive moving average) covariance structure, there were significant region of interest-by-group (F=4.97, df=1, 120, p=0.03) and region of interest-by-group-by-run-by-visit (F=2.37, df=5, 517, p=0.04) interactions. The region of interest-by-group interaction showed that the experimental group had significantly elevated amygdala activity compared with the control group (the mean percent signal change over all runs/days was 0.19 [SD=0.03] for the experimental group and −0.02 [SD=0.02] for the control group [t=7.63, df=403, p<0.001, d=1.44]). Within the intraparietal region, the average percent signal change was significantly higher in the control group than in the experimental group (mean over all runs/days, −0.06 [SD=0.04] for the experimental group and 0.03 [SD=0.02] for the control group [t=2.74, df=403, p=0.04, d=0.89]).
The region of interest-by-group-by-run-by-visit interaction (Figure 1A) showed that the groups did not differ significantly in amygdala activity during the visit 2 baseline or practice but differed significantly from each other during all subsequent runs (t values, >2.52; df=31; p values, <0.02; d values, >0.87). The control group had significantly higher intraparietal activity than the experimental group during the third training and transfer runs at visit 3 (t values, >2.34; df=31; p values, <0.03; d values, >0.84) but did not differ significantly from the experimental group at any other run.

FIGURE 1. Regional Percent Signal Change for Each Region of Interest, Run, and Group in a Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disordera
a In each group, the average percent signal change for the happy-rest condition for each run in the left amygdala (panel A) and in the left horizontal segment of the intraparietal sulcus (panel B).
b Significant difference from the initial pre-neurofeedback baseline run, p<0.05.
c Significant difference from the corresponding run in the experimental group, p<0.05.
Paired-sample t tests were performed to examine whether activity increased significantly from pre-neurofeedback baseline in each group and run. In the control group, there was no run in which amygdala activity differed significantly from baseline. In the experimental group, amygdala activity during the visit 2 practice run was not significantly elevated above baseline, but all subsequent runs, including visit 3 baseline and both transfer runs, were (t values, >2.67; df=17; p values, <0.02; d values, >0.61). In the intraparietal region (Figure 1B), the control group had significantly increased intraparietal activity from baseline during run 3 and the final transfer run at visit 3 (t values, >2.42; df=14; p values, <0.02; d values, >0.69). No other runs showed a significant change in the control group. In the experimental group, there was no run in which intraparietal activity differed from baseline. An independent-samples t test comparing neurofeedback success in the experimental group (for amygdala activity) and the control group (for intraparietal activity) was not significant, indicating that by study end the control group was as effective at regulating hemodynamic activity in the intraparietal region as the experimental group was at regulating activity in the amygdala.
Autobiographical Memory Performance
For the linear mixed model using the ARMA1 covariance structure, there was a significant group-by-visit-by-type interaction (F=29.2, df=3, 61, p<0.001) and a significant group-by-visit-by-type-by-valence interaction (F=5.58, df=3, 66, p=0.002) (Table 2).
| Percent of Memories | ||||||||
|---|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | |||||||
| Baseline | Follow-up | Baseline | Follow-Up | |||||
| Memory Typea | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Specific | 52.5 | 13.1 | 69.5b | 10.0 | 54.8 | 16.9 | 52.1c | 14.7 |
| Positive | 33.1 | 10.8 | 46.8b | 12.7 | 34.1 | 11.1 | 33.3c | 13.1 |
| Negative | 19.4 | 8.9 | 22.7 | 8.6 | 20.7 | 9.2 | 18.8 | 8.9 |
| Categorical | 22.5 | 10.0 | 14.0b | 8.6 | 21.2 | 7.9 | 26.0c | 14.2 |
| Positive | 11.7 | 7.2 | 3.7b | 6.7 | 11.8 | 9.0 | 14.4c | 8.6 |
| Negative | 10.8 | 8.7 | 10.4 | 8.4 | 10.4 | 7.4 | 11.6 | 6.9 |
| Extended | 13.3 | 9.1 | 6.0b | 4.2 | 14.1 | 10.7 | 10.7c | 7.1 |
| Positive | 4.6 | 5.8 | 1.6b | 2.7 | 5.1 | 6.0 | 3.4c | 2.8 |
| Negative | 8.7 | 7.4 | 4.4b | 4.6 | 9.0 | 7.6 | 6.4 | 4.8 |
| Semantic | 7.8 | 4.1 | 6.0 | 8.0 | 7.4 | 7.8 | 8.9 | 7.2 |
| Positive | 4.6 | 4.5 | 4.0 | 6.2 | 3.7 | 4.6 | 5.9 | 6.4 |
| Negative | 3.2 | 4.2 | 1.9 | 3.7 | 3.7 | 4.3 | 3.0 | 4.0 |
| None | 3.9 | 4.6 | 4.5 | 5.2 | 2.5 | 2.3 | 2.3 | 3.7 |
a
A specific memory was defined as memory for a single event that took place at an identified place and did not last longer than 1 day. A categorical memory was defined as a memory referring to a category of events containing a number of specific episodes, without reference to one specific event. An extended memory was defined as a memory that referred to an extended period of time without reference to a specific event within the time period. A semantic memory was defined as a statement of fact without an associated event. These are the standard memory type definitions (26). It is a consistently replicated finding that individuals with depression recall fewer specific and more categorical autobiographical memories compared with healthy individuals (26) and that this cognitive deficit persists despite remission of symptoms (28).
b
Significant difference from baseline, p<0.05.
c
Significant difference from the experimental group, p<0.05.
The group-by-visit-by-type interaction revealed that at visit 1, the groups did not differ significantly on the percent of memories recalled at any specificity. At visit 4, the experimental group recalled more specific and fewer categorical and extended memories than the control group (t values, >3.03; df=54; p values, <0.004; d values, >0.74). The percent of semantic memories recalled did not differ at visit 4. The group-by-type-by-valence-by-visit interaction revealed that these effects were driven by a change in the percent of positive memories recalled. The experimental group recalled more positive specific memories at visit 4 than the control group (t=2.87, df=31, p<0.001, d=0.99) but did not differ in the percent of specific negative memories recalled at visit 4. The experimental group recalled fewer positive categorical and extended memories than the control group at visit 4 (t values, >2.40; df=31; p values, <0.02; d values, >0.83). The percent of distinctly valenced semantic memories recalled did not differ between groups, and in no case did any score at visit 1 differ between groups.
Paired-sample t tests were performed within each group to examine whether scores significantly changed from baseline to follow-up. In the experimental group, the percent of positive specific and overall specific memories recalled increased significantly (t values, >4.59; df=17; p values, <0.001; d values, >1.10) and the percent of categorical positive, overall categorical, extended positive, extended negative, and overall extended memories recalled decreased significantly at visit 4 relative to visit 1 (t values, >2.32; df=17; p values, <0.03; d values, >0.60). In the control group, there was no significant change in memory recall.
Association Between Memory Recall, Neurofeedback Success, and MADRS Change
Using linear regression, we examined the association between residualized MADRS scores at follow-up and residualized amygdala activity during the final transfer run. Residual MADRS scores at the final visit were significantly correlated with residual amygdala activity during the final transfer run (β=−15.5, t=3.09, p=0.004; adjusted R2=0.21). While the association with intraparietal success was in the same direction, it was not significant (β=−2.46, t=0.81, p=0.43; adjusted R2=0.09), and it was significantly different from the model examining the association between residual amygdala activity and residual MADRS scores (z=2.66, p=0.004).
A regression analysis was performed for residual positive specific memory recall and residual MADRS scores at follow-up. The same pattern was seen as with amygdala neurofeedback success; residual positive specific memory recall was associated with decreased residual MADRS scores (β=−0.19, t=2.16, p=0.04; adjusted R2=0.13). Residual positive specific memory recall was also significantly associated with residual amygdala activity during the final transfer run (β=29.1, t=3.10, p=0.004; adjusted R2=0.21).
To determine whether residual amygdala activity was a mediator of the association between residual positive specific memory recall and residual MADRS change, we performed a Sobel test, which was significant (Z=2.18, p=0.03) (Figure 2). When both residual amygdala activity and residual positive specific memory recall were included in the model, the effects of memory recall were no longer significant (β=−0.07, t=0.71, p=0.48), while amygdala activity was (β=13.5, t=2.33, p=0.027; final model adjusted R2=0.25).
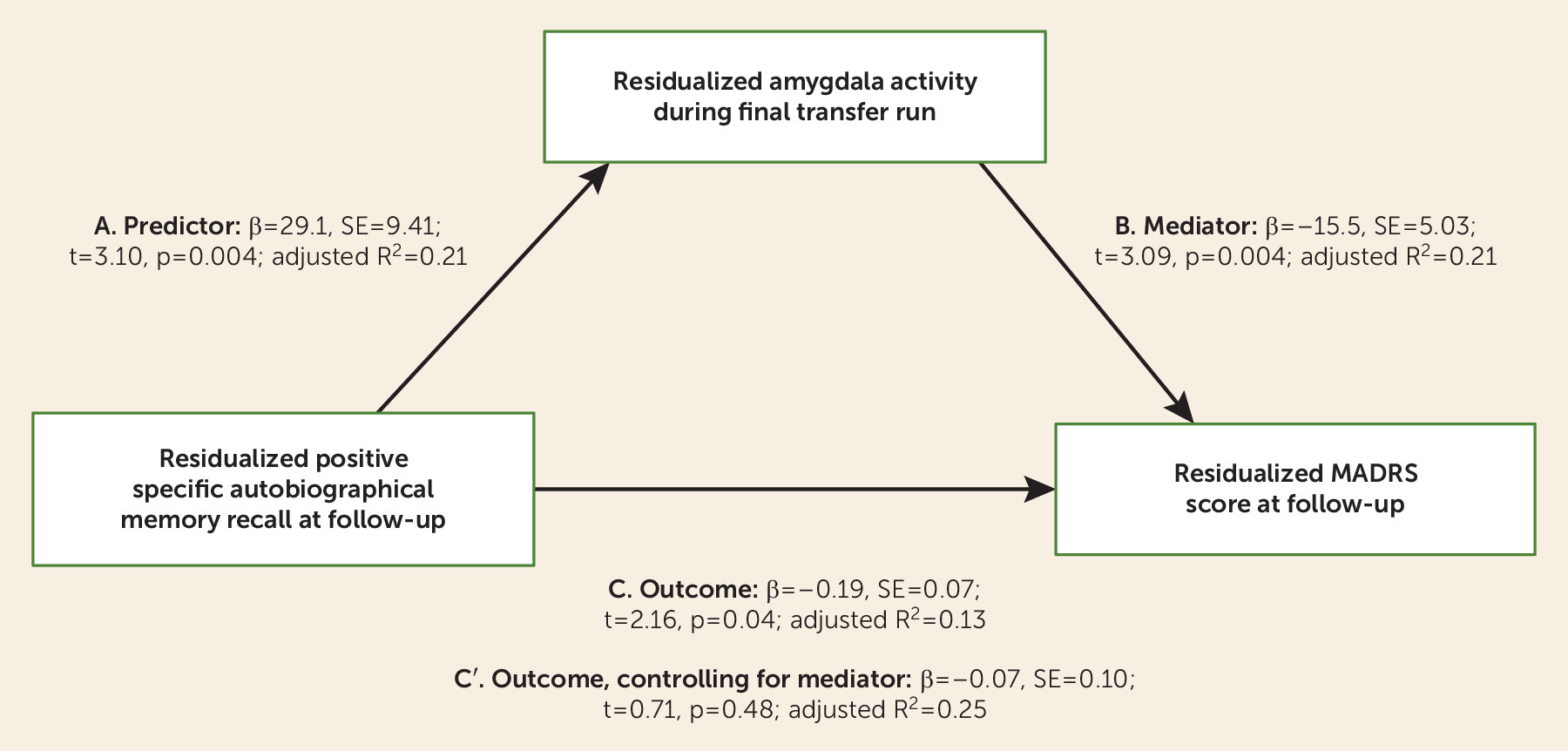
FIGURE 2. Overall Mediation Model in a Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disordera
a MADRS=Montgomery-Åsberg Depression Rating Scale. In A, the predictor is residualized positive specific autobiographical memory recall at follow-up. In B, the mediator is residual amygdala activity during the final transfer run. In C, outcome is residual depressive symptoms. C denotes the relationship between predictor and outcome, and C′ denotes the same relationship after controlling for the effect of the mediator.
Discussion
In this randomized clinical trial, we found that training that enhances the amygdala’s hemodynamic response to positive memories significantly reduced depressive symptoms in depressed participants. These data qualitatively replicate and extend results from our previous study in an independent sample of depressed participants (9), which showed that in a single amygdala rtfMRI-nf session, participants learned to regulate their amygdala response during positive memory recall and manifested mood improvements. In the present study, the experimental group showed a mean decrease in MADRS score of 50% over the course of the intervention, and 32% of participants met criteria for remission at study end. This remission rate is similar to rates seen with antidepressant medications (37) and cognitive-behavioral therapy (38). The average decrease in MADRS score in the control group was 8%, and 6% of control participants met criteria for remission at study end, demonstrating a modest placebo response and suggesting that while the mental strategy of recalling positive memories likely played some part in symptom improvement, neurofeedback from the amygdala was crucial.
The importance of amygdala neurofeedback to the antidepressant effect is further highlighted by the results of a previous study (39) that found that simply instructing depressed individuals to recall positive memories to improve mood actually worsened mood ratings. Our results suggest that positive memory retrieval while engaging the amygdala, which notably improved the recall of specific positive memories, instead holds the potential to improve mood. The finding that intraparietal activity did not change in the experimental group suggests that feedback from the amygdala is necessary for enhancing control of that region. In contrast, the control group did increase intraparietal response to a degree similar to the experimental group’s increase in amygdala response, but depressive symptoms improved to a greater extent in the experimental group, suggesting that the observed effects were due to amygdala rtfMRI-nf in combination with positive memory recall. Furthermore, while the correlation between residual intraparietal activity and residual MADRS scores was in the same direction as that observed between amygdala activity and MADRS scores, the association was not significant, supporting the hypothesis that enhanced control of amygdala activity led to the clinical effects, and not simply control over hemodynamic activity more generally.
Our interpretation that the amygdala response to positive memory recall is involved in recovery from depression is further supported by the mediation analysis. These data showed that while residual positive specific memory recall at follow-up was negatively associated with residual MADRS scores at follow-up, residual amygdala activity during the final transfer run accounted for a significant amount of variance in this correlation. This proposed model suggests that recalling more positive specific memories can reduce depressive symptoms, but more so when the amygdala is engaged. As the amygdala is part of the salience network (12), and our whole-brain analysis revealed increased activity in multiple nodes of the salience network after training, training participants with depression to engage the amygdala during positive memory recall conceivably enhances the affective or attentional significance of these memories. We thus propose that the synergy between amygdala activity and positive memory recall drives the clinical improvements.
The rtfMRI-nf training also resulted in an increase in the percent of specific memories recalled and a decrease in the percent of overgeneral memories recalled in the experimental group. This effect was predominantly attributable to positive memories. Overgeneral memory recall, especially for positive events, is an enduring cognitive deficit observed in patients with depression (26) that is not addressed by current treatments (28) and reportedly confers vulnerability to persistent depressive episodes (40). The finding that rtfMRI-nf improved positive specific memory recall thus suggests that this intervention may reverse a pathological construct that predisposes to or maintains depressive episodes.
Several study limitations merit comment. First, only two rtfMRI-nf sessions were performed. While improved clinical scores could be seen after a single session, additional score improvements were evident after a second session. Furthermore, while baseline amygdala activity during positive memory recall was higher during the second session relative to the first, this activity was still lower than that observed during the transfer runs, suggesting that additional learning might have occurred. Determining the optimal number of sessions and whether booster sessions are needed is an important future direction for this research. Additionally, our entrance criteria resulted in a large proportion of patients being excluded (primarily because of medication status or not meeting DSM-IV-TR criteria for major depressive disorder), limiting the generalizability of our findings. Further testing in larger, more heterogeneous samples that include medicated individuals is necessary to determine the subpopulations or characteristics for whom this intervention is best suited. Finally, patients were only followed for 1 week after the final rtfMRI-nf session, whereas acute treatment trials more commonly include follow-up periods lasting 2–8 weeks. Therefore, while we were able to show that amygdala rtfMRI-nf resulted in significant and large clinical improvements, the duration of this improvement was not assessed.
In conclusion, we have shown that rtfMRI-nf training aimed at increasing amygdala response to positive memory recall results in significant clinical improvement in patients with depression and increases the percent of specific memories recalled on an autobiographical memory test. This neurofeedback intervention targets a specific fundamental mechanism identified by neuroimaging research (blunted amygdala activity during positive memory recall), it appears safe and well tolerated, and it gives patients a sense of control over their treatment and symptom improvement. This novel intervention therefore merits further testing as a potential treatment for depression, and it can serve as a model for novel neuroscience-based interventions.
Acknowledgments
Supported in part by NIMH grant K99MH101235 and by a NARSAD Young Investigator Grant from the Brain and Behavior Research Foundation.
Footnote
ClinicalTrials.gov identifier: NTC02079610.
Supplementary Material
File (appi.ajp.2017.16060637.ds001.pdf)
- View/Download
- 929.15 KB
References
1.
World Health Organization (WHO): The World Health Report 2004: Changing History. Geneva, WHO, 2004
2.
Cain RA: Navigating the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study: practical outcomes and implications for depression treatment in primary care. Prim Care 2007; 34:505–519
3.
Cox RW, Jesmanowicz A, Hyde JS: Real-time functional magnetic resonance imaging. Magn Reson Med 1995; 33:230–236
4.
deCharms RC: Applications of real-time fMRI. Nat Rev Neurosci 2008; 9:720–729
5.
deCharms RC, Maeda F, Glover GH, et al: Control over brain activation and pain learned by using real-time functional MRI. Proc Natl Acad Sci USA 2005; 102:18626–18631
6.
Hartwell KJ, Hanlon CA, Li X, et al: Individualized real-time fMRI neurofeedback to attenuate craving in nicotine-dependent smokers. J Psychiatry Neurosci 2016; 41:48–55
7.
Zilverstand A, Sorger B, Sarkheil P, et al: fMRI neurofeedback facilitates anxiety regulation in females with spider phobia. Front Behav Neurosci 2015; 9:148
8.
Linden DE, Habes I, Johnston SJ, et al: Real-time self-regulation of emotion networks in patients with depression. PLoS One 2012; 7:e38115
9.
Young KD, Zotev V, Phillips R, et al: Real-time fMRI neurofeedback training of amygdala activity in patients with major depressive disorder. PLoS One 2014; 9:e88785
10.
Hamann S: Cognitive and neural mechanisms of emotional memory. Trends Cogn Sci 2001; 5:394–400
11.
LeDoux J: The emotional brain, fear, and the amygdala. Cell Mol Neurobiol 2003; 23:727–738
12.
Davis M, Whalen PJ: The amygdala: vigilance and emotion. Mol Psychiatry 2001; 6:13–34
13.
Sergerie K, Chochol C, Armony JL: The role of the amygdala in emotional processing: a quantitative meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev 2008; 32:811–830
14.
Markowitsch HJ, Vandekerckhove MM, Lanfermann H, et al: Engagement of lateral and medial prefrontal areas in the ecphory of sad and happy autobiographical memories. Cortex 2003; 39:643–665
15.
Young KD, Siegle GJ, Bodurka J, et al: Amygdala activity during autobiographical memory recall in depressed and vulnerable individuals: association with symptom severity and autobiographical overgenerality. Am J Psychiatry 2016; 173:78–89
16.
Sah P, Faber ES, Lopez De Armentia M, et al: The amygdaloid complex: anatomy and physiology. Physiol Rev 2003; 83:803–834
17.
Amaral DG, Price JL: Amygdalo-cortical projections in the monkey (Macaca fascicularis). J Comp Neurol 1984; 230:465–496
18.
Banks SJ, Eddy KT, Angstadt M, et al: Amygdala-frontal connectivity during emotion regulation. Soc Cogn Affect Neurosci 2007; 2:303–312
19.
Kilpatrick L, Cahill L: Amygdala modulation of parahippocampal and frontal regions during emotionally influenced memory storage. Neuroimage 2003; 20:2091–2099
20.
Whalen PJ, Shin LM, Somerville LH, et al: Functional neuroimaging studies of the amygdala in depression. Semin Clin Neuropsychiatry 2002; 7:234–242
21.
Victor TA, Furey ML, Fromm SJ, et al: Relationship between amygdala responses to masked faces and mood state and treatment in major depressive disorder. Arch Gen Psychiatry 2010; 67:1128–1138
22.
Suslow T, Konrad C, Kugel H, et al: Automatic mood-congruent amygdala responses to masked facial expressions in major depression. Biol Psychiatry 2010; 67:155–160
23.
Siegle GJ, Ghinassi F, Thase ME: Neurobehavioral therapies in the 21st century: summary of an emerging field and an extended example of cognitive control training for depression. Cognit Ther Res 2007; 31:235–262
24.
Young KD, Bellgowan PS, Bodurka J, et al: Behavioral and neurophysiological correlates of autobiographical memory deficits in patients with depression and individuals at high risk for depression. JAMA Psychiatry 2013; 70:698–708
25.
Zotev V, Krueger F, Phillips R, et al: Self-regulation of amygdala activation using real-time fMRI neurofeedback. PLoS One 2011; 6:e24522
26.
Williams JM, Barnhofer T, Crane C, et al: Autobiographical memory specificity and emotional disorder. Psychol Bull 2007; 133:122–148
27.
Young KD, Bellgowan PS, Bodurka J, et al: Neurophysiological correlates of autobiographical memory deficits in currently and formerly depressed subjects. Psychol Med 2014; 44:2951–2963
28.
Nandrino JL, Pezard L, Posté A, et al: Autobiographical memory in major depression: a comparison between first-episode and recurrent patients. Psychopathology 2002; 35:335–340
29.
Snaith RP, Hamilton M, Morley S, et al: A scale for the assessment of hedonic tone: the Snaith-Hamilton Pleasure Scale. Br J Psychiatry 1995; 167:99–103
30.
Montgomery SA, Asberg M: A new depression scale designed to be sensitive to change. Br J Psychiatry 1979; 134:382–389
31.
Williams JM, Broadbent K: Autobiographical memory in suicide attempters. J Abnorm Psychol 1986; 95:144–149
32.
Fias W, Lammertyn J, Caessens B, et al: Processing of abstract ordinal knowledge in the horizontal segment of the intraparietal sulcus. J Neurosci 2007; 27:8952–8956
33.
Dehaene S, Piazza M, Pinel P, et al: Three parietal circuits for number processing. Cogn Neuropsychol 2003; 20:487–506
34.
Bodurka J, Bandettini P: Real-time software for monitoring MRI scanner operation. Neuroimage 2008; 41:S85
35.
Suzuki A, Aoshima T, Fukasawa T, et al: A three-factor model of the MADRS in major depressive disorder. Depress Anxiety 2005; 21:95–97
36.
Iannuzzo RW, Jaeger J, Goldberg JF, et al: Development and reliability of the HAM-D/MADRS interview: an integrated depression symptom rating scale. Psychiatry Res 2006; 145:21–37
37.
Arroll B, Macgillivray S, Ogston S, et al: Efficacy and tolerability of tricyclic antidepressants and SSRIs compared with placebo for treatment of depression in primary care: a meta-analysis. Ann Fam Med 2005; 3:449–456
38.
Cuijpers P, Smit F, Bohlmeijer E, et al: Efficacy of cognitive-behavioural therapy and other psychological treatments for adult depression: meta-analytic study of publication bias. Br J Psychiatry 2010; 196:173–178
39.
Joormann J, Siemer M, Gotlib IH: Mood regulation in depression: differential effects of distraction and recall of happy memories on sad mood. J Abnorm Psychol 2007; 116:484–490
40.
Peeters F, Wessel I, Merckelbach H, et al: Autobiographical memory specificity and the course of major depressive disorder. Compr Psychiatry 2002; 43:344–350
Information & Authors
Information
Published In
History
Received: 3 June 2016
Revision received: 4 October 2016
Revision received: 20 December 2016
Revision received: 27 January 2017
Accepted: 7 March 2017
Published online: 14 April 2017
Published in print: August 01, 2017
Keywords
Authors
Competing Interests
Dr. Drevets is an employee of Janssen Research and Development (of Johnson & Johnson) and is a stockholder in Johnson & Johnson. The other authors report no financial relationships with commercial interests.
Funding Information
National Institute of Mental Health10.13039/100000025: K99MH101235
Brain and Behavior Research Foundation10.13039/100000874: NARSAD Young Investigator Award
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
FIGURE 1. Regional Percent Signal Change for Each Region of Interest, Run, and Group in a Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disordera
a In each group, the average percent signal change for the happy-rest condition for each run in the left amygdala (panel A) and in the left horizontal segment of the intraparietal sulcus (panel B).
b Significant difference from the initial pre-neurofeedback baseline run, p<0.05.
c Significant difference from the corresponding run in the experimental group, p<0.05.
FIGURE 2. Overall Mediation Model in a Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disordera
a MADRS=Montgomery-Åsberg Depression Rating Scale. In A, the predictor is residualized positive specific autobiographical memory recall at follow-up. In B, the mediator is residual amygdala activity during the final transfer run. In C, outcome is residual depressive symptoms. C denotes the relationship between predictor and outcome, and C′ denotes the same relationship after controlling for the effect of the mediator.
Tables
Media
References
References
1.
World Health Organization (WHO): The World Health Report 2004: Changing History. Geneva, WHO, 2004
2.
Cain RA: Navigating the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study: practical outcomes and implications for depression treatment in primary care. Prim Care 2007; 34:505–519
3.
Cox RW, Jesmanowicz A, Hyde JS: Real-time functional magnetic resonance imaging. Magn Reson Med 1995; 33:230–236
4.
deCharms RC: Applications of real-time fMRI. Nat Rev Neurosci 2008; 9:720–729
5.
deCharms RC, Maeda F, Glover GH, et al: Control over brain activation and pain learned by using real-time functional MRI. Proc Natl Acad Sci USA 2005; 102:18626–18631
6.
Hartwell KJ, Hanlon CA, Li X, et al: Individualized real-time fMRI neurofeedback to attenuate craving in nicotine-dependent smokers. J Psychiatry Neurosci 2016; 41:48–55
7.
Zilverstand A, Sorger B, Sarkheil P, et al: fMRI neurofeedback facilitates anxiety regulation in females with spider phobia. Front Behav Neurosci 2015; 9:148
8.
Linden DE, Habes I, Johnston SJ, et al: Real-time self-regulation of emotion networks in patients with depression. PLoS One 2012; 7:e38115
9.
Young KD, Zotev V, Phillips R, et al: Real-time fMRI neurofeedback training of amygdala activity in patients with major depressive disorder. PLoS One 2014; 9:e88785
10.
Hamann S: Cognitive and neural mechanisms of emotional memory. Trends Cogn Sci 2001; 5:394–400
11.
LeDoux J: The emotional brain, fear, and the amygdala. Cell Mol Neurobiol 2003; 23:727–738
12.
Davis M, Whalen PJ: The amygdala: vigilance and emotion. Mol Psychiatry 2001; 6:13–34
13.
Sergerie K, Chochol C, Armony JL: The role of the amygdala in emotional processing: a quantitative meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev 2008; 32:811–830
14.
Markowitsch HJ, Vandekerckhove MM, Lanfermann H, et al: Engagement of lateral and medial prefrontal areas in the ecphory of sad and happy autobiographical memories. Cortex 2003; 39:643–665
15.
Young KD, Siegle GJ, Bodurka J, et al: Amygdala activity during autobiographical memory recall in depressed and vulnerable individuals: association with symptom severity and autobiographical overgenerality. Am J Psychiatry 2016; 173:78–89
16.
Sah P, Faber ES, Lopez De Armentia M, et al: The amygdaloid complex: anatomy and physiology. Physiol Rev 2003; 83:803–834
17.
Amaral DG, Price JL: Amygdalo-cortical projections in the monkey (Macaca fascicularis). J Comp Neurol 1984; 230:465–496
18.
Banks SJ, Eddy KT, Angstadt M, et al: Amygdala-frontal connectivity during emotion regulation. Soc Cogn Affect Neurosci 2007; 2:303–312
19.
Kilpatrick L, Cahill L: Amygdala modulation of parahippocampal and frontal regions during emotionally influenced memory storage. Neuroimage 2003; 20:2091–2099
20.
Whalen PJ, Shin LM, Somerville LH, et al: Functional neuroimaging studies of the amygdala in depression. Semin Clin Neuropsychiatry 2002; 7:234–242
21.
Victor TA, Furey ML, Fromm SJ, et al: Relationship between amygdala responses to masked faces and mood state and treatment in major depressive disorder. Arch Gen Psychiatry 2010; 67:1128–1138
22.
Suslow T, Konrad C, Kugel H, et al: Automatic mood-congruent amygdala responses to masked facial expressions in major depression. Biol Psychiatry 2010; 67:155–160
23.
Siegle GJ, Ghinassi F, Thase ME: Neurobehavioral therapies in the 21st century: summary of an emerging field and an extended example of cognitive control training for depression. Cognit Ther Res 2007; 31:235–262
24.
Young KD, Bellgowan PS, Bodurka J, et al: Behavioral and neurophysiological correlates of autobiographical memory deficits in patients with depression and individuals at high risk for depression. JAMA Psychiatry 2013; 70:698–708
25.
Zotev V, Krueger F, Phillips R, et al: Self-regulation of amygdala activation using real-time fMRI neurofeedback. PLoS One 2011; 6:e24522
26.
Williams JM, Barnhofer T, Crane C, et al: Autobiographical memory specificity and emotional disorder. Psychol Bull 2007; 133:122–148
27.
Young KD, Bellgowan PS, Bodurka J, et al: Neurophysiological correlates of autobiographical memory deficits in currently and formerly depressed subjects. Psychol Med 2014; 44:2951–2963
28.
Nandrino JL, Pezard L, Posté A, et al: Autobiographical memory in major depression: a comparison between first-episode and recurrent patients. Psychopathology 2002; 35:335–340
29.
Snaith RP, Hamilton M, Morley S, et al: A scale for the assessment of hedonic tone: the Snaith-Hamilton Pleasure Scale. Br J Psychiatry 1995; 167:99–103
30.
Montgomery SA, Asberg M: A new depression scale designed to be sensitive to change. Br J Psychiatry 1979; 134:382–389
31.
Williams JM, Broadbent K: Autobiographical memory in suicide attempters. J Abnorm Psychol 1986; 95:144–149
32.
Fias W, Lammertyn J, Caessens B, et al: Processing of abstract ordinal knowledge in the horizontal segment of the intraparietal sulcus. J Neurosci 2007; 27:8952–8956
33.
Dehaene S, Piazza M, Pinel P, et al: Three parietal circuits for number processing. Cogn Neuropsychol 2003; 20:487–506
34.
Bodurka J, Bandettini P: Real-time software for monitoring MRI scanner operation. Neuroimage 2008; 41:S85
35.
Suzuki A, Aoshima T, Fukasawa T, et al: A three-factor model of the MADRS in major depressive disorder. Depress Anxiety 2005; 21:95–97
36.
Iannuzzo RW, Jaeger J, Goldberg JF, et al: Development and reliability of the HAM-D/MADRS interview: an integrated depression symptom rating scale. Psychiatry Res 2006; 145:21–37
37.
Arroll B, Macgillivray S, Ogston S, et al: Efficacy and tolerability of tricyclic antidepressants and SSRIs compared with placebo for treatment of depression in primary care: a meta-analysis. Ann Fam Med 2005; 3:449–456
38.
Cuijpers P, Smit F, Bohlmeijer E, et al: Efficacy of cognitive-behavioural therapy and other psychological treatments for adult depression: meta-analytic study of publication bias. Br J Psychiatry 2010; 196:173–178
39.
Joormann J, Siemer M, Gotlib IH: Mood regulation in depression: differential effects of distraction and recall of happy memories on sad mood. J Abnorm Psychol 2007; 116:484–490
40.
Peeters F, Wessel I, Merckelbach H, et al: Autobiographical memory specificity and the course of major depressive disorder. Compr Psychiatry 2002; 43:344–350