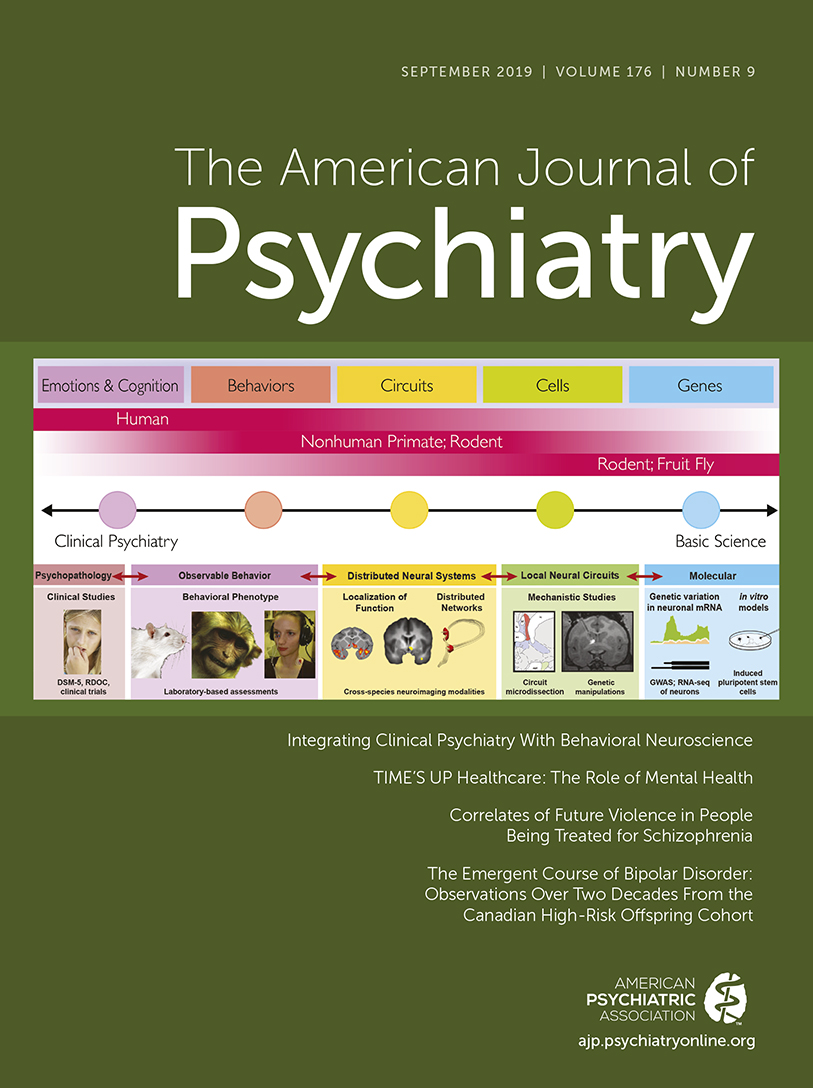
TIME’S UP Healthcare: The Role of Mental Health
| TIME’S UP Healthcare Goal | Potential Steps for Mental Health Care Providers |
|---|---|
| Unite health care workers across fields | • Sign up for TIME’S UP Healthcare listserv to receive updates on the organization’s initiatives. • Encourage interdisciplinary team members to join. • Develop cross-disciplinary women’s peer-mentorship groups at your institution. |
| Improve care for targets of harassment and inequity | • Provide affected individuals with access to resources through the TIME’S UP web site. • Understand the steps for reporting in your own institution and share with colleagues. • Understand what kind of trauma-informed care is available at your institution for referrals. • Support patients, trainees, and colleagues who turn to you with these issues using a nonjudgmental, trauma-informed stance. • Understand that trainees may be afraid of being alone with a patient, and consider accompanying them, specifically in high-risk situations. |
| Raise awareness and knowledge | • Talk about gender inequity and harassment with colleagues. • Wear TIME’S UP pins or scrubs or place stickers on laptops to facilitate discussion with colleagues. • Present about gender harassment and discrimination in grand rounds and workshops in national and international meetings. • Identify and name instances of sexual harassment and inequity when they occur in the workplace. • Provide routine education about harassment for the entire health care workforce in your own health care delivery setting. • Help individuals understand what defines sexual harassment, including the range of verbal and nonverbal behaviors that convey coercion, hostility, intimidation, objectification, exclusion, and behaviors or practices that convey or enforce the second-class status of women. |
| Support health care organizations in making this issue central and visible | • Encourage your health care organization to sign on as a signatory institution to TIME’S UP Healthcare (https://www.timesuphealthcare.org/signatories). • Make your sexual harassment policies accessible and visible, including posting signs about having zero tolerance of harassment in your institution. • Consider encouraging your institution to adopt online reporting systems like Callisto (www.projectcallisto.org), which has been shown to reduce time and increase reporting of sexual assault. • Promote gender equity by inviting women to speak at grand rounds at your organization and/or to be on panels at national and international conferences. • Begin to address underlying gender inequities at your home institution by developing structural processes to promote sponsorship and nomination of women and other intersectional minority groups for awards and promotion. |
| Provide a link to the TIME’S UP Legal Defense Fund | • Refer health care workers to the TIME’S UP Legal Defense Fund, which connects those who experience sexual misconduct with legal and public relations assistance. This includes people who experience assault, harassment, abuse, and related retaliation in the workplace or when trying to advance their careers. |
| Advocate for meaningful standards | • Advocate for a zero-tolerance policy at your home institution. • Advocate for bystander training and improved sexual harassment training at your home institution. • Advocate at the state and national level for clear rules about sexual harassment and response to the perpetrator. • Advocate for funding organizations (federal, state, and philanthropic) to consider the role of sexual harassment allegations in grant funding opportunities. • Identify metrics to ensure existing policies and procedures are implemented effectively and to measure critical outcomes like attrition of women and underrepresented minorities; resource allocation equity; and occupational, mental, and general medical health outcomes of targets after harassment. • Perform root cause analysis of harassment cases to shed light on organization factors fostering harassment and inequities. |
| Advance research on harassment and inequity | • Study the prevalence of sexual harassment in mental health care settings and training programs. • Study the influence of workplace gender inequity on mental health and burnout. • Develop and study novel interventions to eliminate gender inequities in health care. |
Acknowledgments
References
Information & Authors
Information
Published In
History
Keywords
Authors
Competing Interests
Competing Interests
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).