Mental Health Service Use and Psychopharmacological Treatment Following Psychotic Experiences in Preadolescence
Abstract
Objective:
Methods:
Results:
Conclusions:
Methods
Study Population
Child Assessments
Psychotic experiences.
Mental disorders at age 11.
IQ proxy.
Register Data
ICD-10 hospital diagnoses.
Psychotropic medications.
Register-based covariates.
Statistical Analysis
Ethics
Results
| Variable | Register Diagnosis Before Examination (N=60) | Register Diagnosis During Follow-Up (N=90) | All Participants (N=1,632) | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Psychotic experiences | 7 | 11.7 | 23 | 25.6 | 172 | 10.5 |
| Any DAWBA diagnosisa | 40 | 67.9 | 27 | 30.0 | 224 | 13.8 |
| Register diagnoses | ||||||
| Neurodevelopmental diagnosis | 53 | 88.3 | 48 | 53.3 | 101 | 6.2 |
| Emotional diagnosis | 21 | 35.0 | 57 | 63.3 | 78 | 4.8 |
| Other diagnosis | 12 | 20 | 37 | 41.1 | 49 | 3.0 |
| Any Mental Disorder (N=90) | Model 1b | Model 2c | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | N | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p |
| No psychotic experiences | 1,407 | Reference | Reference | Reference | ||||||
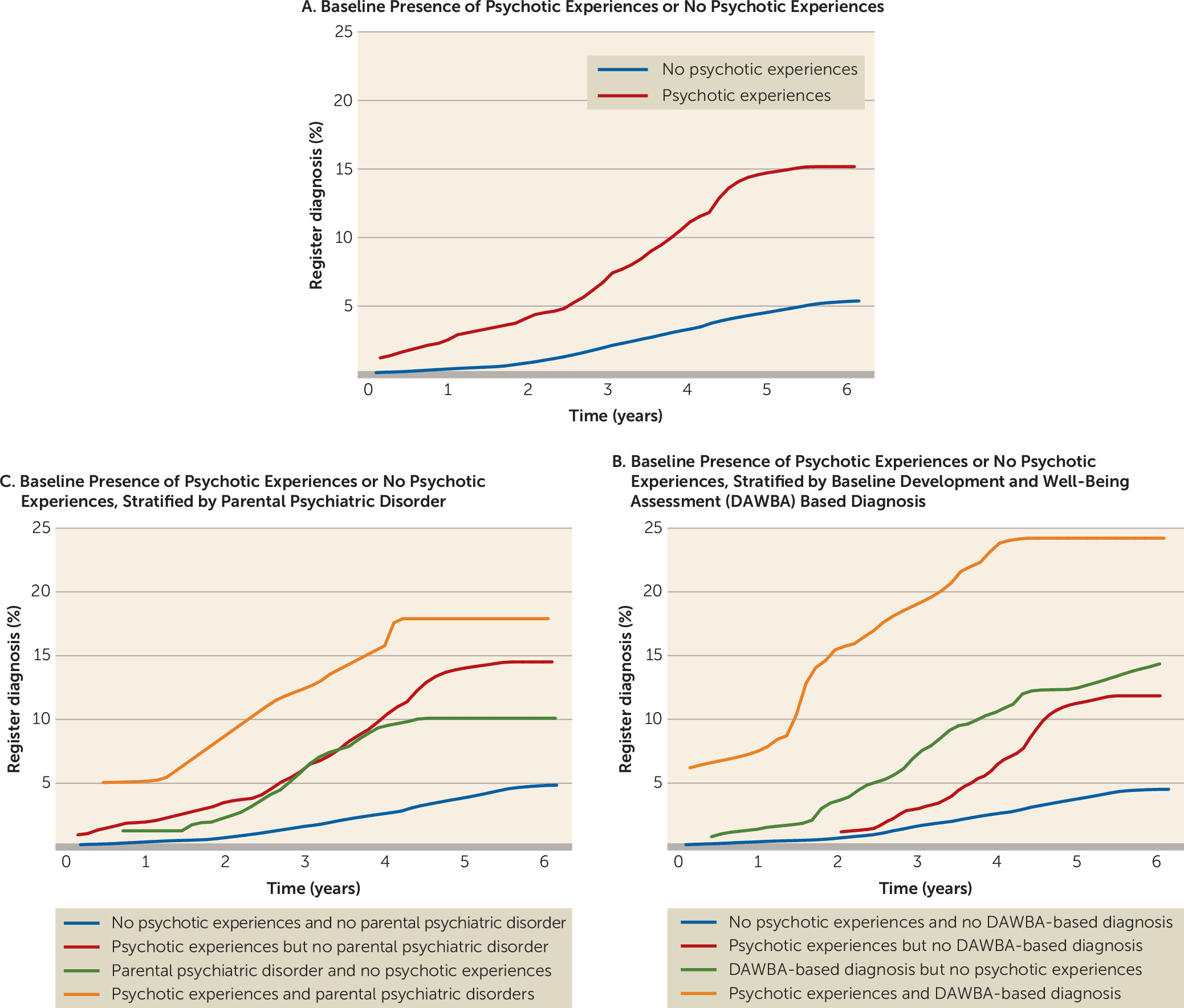
| Psychotic experiences | 165 | 3.08 | 1.92, 4.95 | <0.001 | 3.14 | 1.94, 5.09 | <0.001 | 3.13 | 1.93, 5.07 | <0.001 |
| Stratification by DAWBA ICD-10 diagnosis at baselined | ||||||||||
| No psychotic experiences and no DAWBA ICD-10 diagnosis | 1,260 | Reference | Reference | Reference | ||||||
| Psychotic experiences without DAWBA ICD-10 diagnosis | 119 | 2.81 | 1.53, 5.17 | 0.001 | 2.78 | 1.49, 5.18 | 0.001 | 2.76 | 1.48, 5.13 | 0.001 |
| DAWBA ICD-10 diagnosis without psychotic experiences | 138 | 3.28 | 1.89, 5.69 | <0.001 | 3.33 | 1.90, 5.81 | <0.001 | 3.29 | 1.88, 5.77 | <0.001 |
| Psychotic experiences with DAWBA ICD-10 diagnosis | 46 | 6.40 | 3.25, 12.62 | <0.001 | 7.73 | 3.88, 15.37 | <0.001 | 7.85 | 3.94, 15.63 | <0.001 |
| Stratification by parental history of register mental disorder from 1995 to 2011 | ||||||||||
| No psychotic experiences and no parental history of mental disorder | 1,249 | Reference | Reference | Reference | ||||||
| Psychotic experiences without parental history of mental disorder | 135 | 3.36 | 1.96, 5.74 | <0.001 | 3.56 | 2.06, 6.13 | <0.001 | 3.55 | 2.06, 6.12 | <0.001 |
| Parental history of mental disorder without psychotic experiences | 158 | 2.41 | 1.36, 4.28 | 0.003 | 2.61 | 1.44, 4.73 | 0.002 | 2.63 | 1.45, 4.77 | 0.001 |
| Psychotic experiences with parental history of mental disorder | 30 | 4.44 | 1.77, 11.12 | 0.001 | 4.74 | 1.85, 12.11 | 0.001 | 4.67 | 1.83, 11.92 | 0.001 |
| Any Psychopharmaceutical (N=58) | Model 1b | Model 2c | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | N | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p |
| No psychotic experiences | 1,394 | Reference | Reference | Reference | ||||||
| Psychotic experiences | 162 | 2.85 | 1.56, 5.20 | 0.001 | 2.71 | 1.47, 5.00 | 0.001 | 2.70 | 1.46, 5.00 | 0.001 |
| Stratification by DAWBA ICD-10 diagnosis at baselined | ||||||||||
| No psychotic experiences and no DAWBA ICD-10 diagnosis | 1,256 | Reference | Reference | Reference | ||||||
| Psychotic experiences without DAWBA ICD–10 diagnosis | 119 | 2.24 | 0.93, 5.40 | 0.072 | 2.06 | 0.85, 5.00 | 0.111 | 2.03 | 0.84, 4.95 | 0.118 |
| DAWBA ICD-10 diagnosis without psychotic experiences | 129 | 5.28 | 2.83, 9.86 | <0.001 | 4.96 | 2.65, 9.29 | <0.001 | 4.91 | 2.61, 9.25 | <0.001 |
| Psychotic experiences with DAWBA ICD-10 diagnosis | 43 | 8.86 | 4.05, 19.38 | <0.001 | 9.73 | 4.41, 21.48 | <0.001 | 9.87 | 4.47, 21.83 | <0.001 |
| Stratification by parental history of register mental disorder from 1995 to 2011 | ||||||||||
| No psychotic experiences and no parental history of mental disorder | 1,241 | Reference | Reference | Reference | ||||||
| Psychotic experiences without parental history of mental disorder | 133 | 2.34 | 1.13, 3.4.85 | <0.022 | 2.28 | 1.09, 4.76 | 0.028 | 2.27 | 1.09, 4.74 | 0.029 |
| Parental history of mental disorder without psychotic experiences | 153 | 1.60 | 0.71, 3.59 | 0.254 | 1.56 | 0.68, 3.57 | 0.292 | 1.57 | 0.69, 3.60 | 0.282 |
| Psychotic experiences with parental history of mental disorder | 29 | 6.44 | 2.53, 16.39 | <0.001 | 6.06 | 2.31, 15.90 | <0.001 | 6.01 | 2.29, 15.77 | <0.001 |
Discussion
Main Findings
Methodological Considerations
Interpretation
Acknowledgments
Supplementary Material
- View/Download
- 525.62 KB
References
Information & Authors
Information
Published In
History
Keywords
Authors
Competing Interests
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).