This issue of the
Journal reflects the remarkable breadth of our field as well as our treatment approaches. Here, we include papers that provide new findings and perspectives related to psychotherapeutic, pharmacological, and neuromodulatory interventions that are aimed at improving outcomes in patients with various psychiatric disorders. Additionally, a clinical case conference is presented that is focused on the traumatic consequences of structural racism (
1). This case underscores the need to value and account for the traumatic effects of structural racism as these factors play out at the individual patient level in the course of psychiatric illnesses and their treatment.
Regarding psychotherapy, we begin with a commentary by Dr. John Markowitz and colleagues that addresses the neglected role of psychotherapeutic interventions for treatment-resistant depression (
2). Their commentary proposes that the definition of treatment-resistant depression should incorporate a lack of response to at least one course of evidence-based psychotherapy. This piece is complemented by a research paper that documents a trend in the reduction in the amount of outpatient psychotherapy that is provided by psychiatrists. An accompanying editorial addresses the challenges that psychiatrists face in providing psychotherapy, the importance of psychotherapy training for residents, and the potential negative impacts on patient care that could result from psychiatrists providing less psychotherapy.
New developments of potential importance are occurring in relation to psychopharmacology and neuromodulation treatment strategies. A review presented in this issue authored by members of the APA Research Council provides a helpful update on cannabinoids and indications for their use in medical practice. While of much interest to our patients and treating psychiatrists, this review concludes that there currently is not sufficient evidence for the use of cannabinoids in the treatment of psychiatric illnesses (
3). Ketamine is another psychoactive substance that has been the focus of intense interest, since at subanesthetic doses it can rapidly decrease depressive symptoms. While perhaps somewhat paradoxical, because ketamine is also a drug of abuse, its use is being explored as an adjunct to treatment for substance use disorders. Accordingly, this issue of the
Journal includes a paper that examines the use of ketamine infusions for reducing drinking behavior in individuals with alcohol use disorder. Ketamine is hypothesized to work, at least in part, by NMDA receptor antagonism, which has stimulated interest in developing other NMDA antagonists as psychiatric therapeutics. In this regard, we present an article reporting on findings from a double-blind randomized trial that examines the efficacy of esmethadone, the
d-isomer of methadone as an adjunctive treatment for major depression. This compound is interesting and may relate to the ketamine story because it is an NMDA antagonist and, unlike the
l-isomer of methadone, has weak effects at the mu opiate receptor. ADHD is a childhood-onset disorder that is effectively treated with stimulants, but what happens to ADHD children as they develop into young adults? A very interesting paper in this issue addresses this question by longitudinally following ADHD illness trajectories into early adulthood. Finally, in relation to the development of more effective neuromodulation strategies for patients with treatment-resistant depression, we include a paper that reports exciting findings from a double-blind clinical trial examining the efficacy of accelerated intermittent theta burst stimulation that also uses individualized functional magnetic resonance imaging (fMRI) neural targeting.
Declines in Psychiatrist Provided Outpatient Psychotherapy
Integrating biological and psychosocial approaches in psychiatry is important in conceptualizing factors that contribute to psychiatric illnesses as well as for the development of optimally effective treatment strategies. In this regard, psychotherapy is an important therapeutic approach supported by a strong evidence base that demonstrates efficacy of diagnosis-specific therapies as well as enhanced effectiveness for various illnesses when used in combination with pharmacologic treatments. When surveyed from 2004–2015, data suggest that, across this time period, the amount of psychotherapy that was delivered to adult patients by mental health practitioners remained stable (
4). Tadmon and Olfson specifically focus on the practices of psychiatrists by attempting to characterize the amount of psychotherapy that is performed in their practices. To estimate trends in the provision of psychotherapy by psychiatrists, the authors used data collected from 1996–2016 as part of the U.S. National Ambulatory Medical Care Survey. Perhaps not surprisingly, the data demonstrated a significant reduction in psychiatrist provided psychotherapy such that over this period the percentage of visits involving psychotherapy declined from 44.4% to 21.6%. From the 1996–2002 data, it was estimated that 27% of psychiatrists provided no psychotherapy in their practices, a rate that increased to 53% with the 2010–2016 data. This study also revealed significant health care inequities such that Black or Hispanic outpatients were less likely to receive psychotherapy from psychiatrists, as were individuals with Medicare or Medicaid compared with private insurance or self-pay. There are a variety of methodologic issues that are important to keep in mind in interpreting the findings from this paper, including the recognition that only a small number of psychiatrists were actually sampled for the survey and that the definition of psychotherapy that was used in this study required that visits had to be longer than 30 minutes. In his editorial, Dr. John Rush discusses the relevance of these decreasing trends to the practice of psychiatry, patient care, and residency training (
5).
Esmethadone as an Adjunctive Treatment for Major Depression
Considerable interest in investigating NMDA receptor antagonists for the treatment of depression has arisen from studies suggesting that ketamine’s efficacy is linked to its NMDA antagonistic properties. Fava and colleagues (
6) report the results from a double-blind randomized study in which the safety and efficacy of two different doses of esmethadone, another NMDA receptor antagonist, are compared with placebo when added to patients’ existing antidepressant regimens. Esmethadone, or dextromethadone, is the
d-isomer of racemic methadone and when compared with the
l-isomer has a considerably lower affinity at the mu opiate receptor. The relative low mu opiate receptor affinity of this compound makes it an attractive drug candidate from the standpoint of concerns related to potential abuse. Interestingly, other work suggests that ketamine’s interactions with opiate systems are important in mediating its antidepressant efficacy (
7). In the current study, three groups of approximately 20 patients received either placebo, esmethadone (25 mg), or esmethadone (50 mg), for 7 days of treatment. The study drug was added to patients’ existing antidepressant medication, which had not been effective in treating their symptoms. Patients were followed for an additional 7 days after completion of study drug administration. Results demonstrated general tolerability of esmethadone with no serious adverse effects, including a lack of dissociative effects, psychotic symptoms, or symptoms related to opiate withdrawal. Both esmethadone doses demonstrated significant reductions in Montgomery-Asberg Depression Rating Scale (MADRS) scores at days 7 and 14 when compared with placebo, and at day 14 significantly greater rates of remission (placebo group: 5%; esmethadone, 25 mg: 31%; esmethadone, 50 mg: 39%). While it is very early in the investigation of this drug, the findings are potentially exciting, especially in relation to the rapid onset of antidepressant effects in patients not responding to their current antidepressant medications. In an editorial, Dr. Charles Nemeroff from the University of Texas at Austin reviews the development of novel antidepressants with respect to these new esmethadone findings and discusses the complexities of understanding esmethadone’s putative mechanism(s) of action regarding NMDA antagonism and possible opiate interactions (
8).
Efficacy of High-Dose Intermittent Theta-Burst Stimulation With Functional Imaging Guided Targeting for Treatment Resistant Depression
Repetitive transcranial stimulation (rTMS) applied to the left dorsolateral prefrontal cortex (dlPFC) region is a neuromodulation therapy that is effective for treatment-resistant depression. More recently, investigators have explored the use of intermittent theta-burst stimulation (iTBS) for treatment-resistant depression. This is a method that is based on the idea that naturally occurring theta rhythms (4–7Hz) in the hippocampus and other cortical regions are linked to neuroplasticity, memory, and learning. iTBS, initially developed as a more efficient treatment strategy than rTMS, employs intermittent bursts of high-frequency stimulation (50hz) applied in triplets with an interval in the theta range of 5 Hz. A key clinical trial used to support FDA approval of iTBS demonstrated that 3 minutes/day of iTBS applied 5 days/week over a 4–6-week period was not inferior to a course of rTMS (10Hz) administered for 37.5 minutes per day over the same time period (
9). In an attempt to improve on the efficacy of rTMS as well as to reduce the overall amount of time required for treatment, the Stanford group developed a protocol for the accelerated use of higher dose iTBS with individualized targeting based on measures of resting state functional connectivity. Initial data from an open-label study suggested that this accelerated, high dose, neural targeting method showed considerable promise at not only reducing treatment time but also in improving efficacy (
10). In this issue of the
Journal, Cole et al. (
11) confirm these findings by reporting results from a double-blind randomized clinical trial in which the efficacy of accelerated iTBS with functional imaging targeting was compared with sham treatment in patients with treatment-resistant depression. Fourteen subjects received active treatment, and 15 received sham treatment applied over 5 consecutive days with MADRS assessment at 4 weeks after treatment as the primary outcome measure. Daily treatment consisted of 10 sessions per day with 50 minutes between sessions delivering a total of 18,000 pulses per day. Prior to treatment, resting state fMRI data was acquired to determine a specific target region within the left dlPFC for iTBS administration. For each individual, the target area within the left dlPFC was identified by finding the specific dlPFC region in which the temporal pattern of the blood-oxygen-level-dependent (BOLD) signal was most inversely correlated with the temporal pattern of the BOLD signal in subgenual anterior cingulate cortex (Area 25). This pattern of connectivity was selected for targeting as it is based on data from various sources implicating Area 25 in the pathophysiology and treatment of depression and the dlPFC as providing regulatory input to Area 25. The trial was stopped after the interim analysis as the results showed a large positive effect size. Specifically, the findings demonstrated that at 4 weeks posttreatment the active group had a 52.5% reduction from baseline in MADRS scores compared with a 11.1% reduction in the sham treatment group. Furthermore, significant reductions in the MADRS scores in the active group were observed at the earlier 1–3-week time points. At the 4-week follow-up period, the active group had at a remission rate of 46.2% and a response rate of 69.2% compared with the sham group with a remission rate at 4 weeks of 0% and a response rate of 7.1%. Overall, the active treatment was well tolerated; an increase in headaches (57%) compared with the sham treatment (13%) was reported. In their editorial (
12), Drs. Cory Weissman and Jeff Daskalis from the University of California at San Diego discuss the importance of this finding as a “significant therapeutic innovation” and comment on the possible mechanisms by which iTBS may alter neuroplasticity. They also raise some issues related to the generalizability of the findings and the feasibility of using functional imaging targeting for larger scale use.
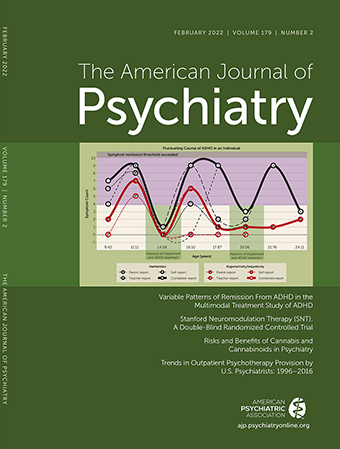
Longitudinal Course of ADHD Symptoms and Remission Into Early Adulthood
A longitudinal ADHD study by Sibley and colleagues (
13) provides valuable insights into the trajectory of ADHD symptoms and their patterns of remission from childhood into adulthood. While numerous cross-sectional studies have been performed characterizing ADHD symptoms, this study using a portion of the Mulitmodal Treatment Study of ADHD sample (N=558) followed children diagnosed with DSM-IV ADHD, combined type, for up to 16 years. Follow-up occurred after ADHD children between 7 and 9.9 years of age were entered into a 14-month treatment study (
14). In addition to the longitudinal design that followed children to the mean age of 25 years, an important aspect of the current study was the focus on patterns of remission. Overall, the results demonstrated considerable fluctuations in symptoms and patterns of partial and full remission. Full remission was defined as symptoms below a specified threshold, no clinically significant impairment, and no ADHD interventions for at least the prior month. Over the eight 2-year assessment periods that occurred over the 16 years of follow-up, 31.4% of individuals were deemed to be in full remission for at least one of the follow-up periods whereas the remainder of the patients never achieved full remission status. Recovery, defined as full remission of ADHD for at least two consecutive assessment points and persisting until the end of the study, occurred in only 9.1% of ADHD individuals. In most of these individuals (76.5%), the onset of their recovery began at 18 years of age or older. At the other end of the spectrum, 10.8% of ADHD individuals had persistent ADHD across all of the time points. In addition, 63.8% of individuals demonstrated a fluctuating course across the study period, characterized by periods of persistence, partial, and full remission, never meeting criteria for recovery. Taken together, these data provide clarity regarding the long-term variable course of symptoms and illness in ADHD patients. In an editorial, Dr. Philip Shaw from National Genome Research Institute comments on the importance of the data from this study and emphasizes the value of future work aimed at an even more in-depth longitudinal assessment of specific ADHD symptom trajectories and their fluctuating severity (
15).
Ketamine Infusions Combined With a Mindfullness Intervention for Alcohol Use Disorder
The use of subanesthetic doses of ketamine has been explored not only in relation to the treatment refractory depression but also as a treatment for substance use disorders (
16,
17). Grabski et al. (
18) add to the substance abuse literature by performing a double-blind ketamine study in individuals attempting to recover from alcohol use disorder. An additional goal of this study was to assess the extent to which ketamine infusions augment the efficacy of mindfulness-based relapse prevention therapy in reducing alcohol use. Ninety-six patients with severe alcohol use disorder that were abstinent for at least 1 day were randomized to one of four conditions: three ketamine intravenous infusions (0.8 mg/kg) with mindfulness-based relapse prevention therapy, three ketamine infusions with alcohol education as a control for psychotherapy, three saline infusions with mindfulness therapy, and three saline infusions with education. Patients received an initial therapy or education session that was followed by six additional sessions that were temporally linked to the infusions; therapy or education sessions immediately preceded and 24 hours later followed the infusion of ketamine or saline. The length of the treatment period for individuals in the study averaged 17.1 days, and patients were followed for approximately 6 months. The findings revealed an overall effect of the ketamine infusions regardless of the addition of psychotherapy as the individuals treated with ketamine demonstrated a 10.1% increase in days abstinent compared with the saline-infused group. However, ketamine infusions were not found to significantly reduce the number of relapses associated with heavy drinking that occurred over the 6-month study period. Compared with the educational sessions, the addition of mindfulness-based relapse prevention therapy did not significantly impact the ketamine-related outcomes. Overall, the findings provide further support for the use of ketamine as an adjunctive treatment for alcohol use disorder and demonstrate relatively long-term, but modest, effects on reducing drinking. Because the sample used for this study met stringent study criteria, additional studies are needed to confirm the generalizability of the findings. Furthermore, while the authors suggest that the combination of ketamine infusions with mindfulness-based relapse prevention therapy may be an optimal treatment approach, at the present time the data from this relatively small study do not provide sufficient evidence for this conclusion.
Conclusions
We are always striving to improve outcomes in our patients, and the papers presented in this issue provide new data and perspectives that are focused on reaching this goal. Take home points include: 1) the importance of considering evidence-based psychotherapeutic interventions in defining and treating treatment-resistant depression; 2) the necessity of understanding the effects of structural racism in formulating an understanding of our patients and their treatment; 3) evidence that esmethadone, an NMDA antagonist and weak mu agonist, may have rapid antidepressant effects when added to ongoing antidepressant therapy; 4) the possibility that accelerated high-dose iTBS, combined with functional imaging targeting, can result in more efficient and effective responses in patients with treatment resistant depression; 5) the importance of longitudinally following children with ADHD into adulthood based on the observation that most individuals with ADHD have long-term fluctuating illness trajectories; and 6) the possibility that ketamine could be used as an adjunctive therapy for reducing drinking behavior in individuals treated for alcohol use disorder.
Psychiatry, perhaps more than any other discipline in medicine, has embraced the integrated use of complementary psychosocial and biological interventions, the range of which are reflected in the papers that contribute to this issue. The new findings presented here provide data and hope for translating the results and concepts of these scientific advances to the clinic.