The opioid epidemic has triggered a need for more interventions for individuals with chronic pain receiving long-term opioid therapy. On the basis of CDC guidelines published in 2016 (
1), opioid prescribers changed their prescribing practices for patients on long-term opioid therapy. Many patients were left to manage chronic pain with either lower doses of opioids or alternative ways of managing pain that can put them at high risk for detrimental consequences. Several studies have shown that individuals on long-term opioid therapy who discontinued opioids, either abruptly or following a dose reduction, had significantly higher odds of suicide and overdose than individuals who remained on opioids (
2,
3). Furthermore, increased dosage and longer duration of opioid therapy has been associated with development of an opioid use disorder (
4). The more recent 2022 guidelines emphasize that patients and prescribers should collaboratively explore both pharmacological and nonpharmacological approaches to treatment and discuss multimodal options for the management of pain that are acceptable, available, and accessible (
5).
Chronic pain, substance misuse and substance use disorder, and other stress-related comorbid psychiatric disorders commonly occur together in a complex combination that is difficult to treat. Negative affect and cognitions, anxiety sensitivity, distress tolerance, and emotion regulation difficulties are common transdiagnostic factors in all these disorders. Novel interventions to address factors that intersect these disorders are urgently needed.
A higher percentage of U.S. veterans report experiencing chronic pain than nonveterans (32% and 20%, respectively) (
6). Veterans are also more likely than nonveterans to report poor health, disability, and co-occurring mental health problems, all of which are risk factors for opioid or other substance use disorders and subsequently higher overdose rates (
7,
8).
In this issue of the
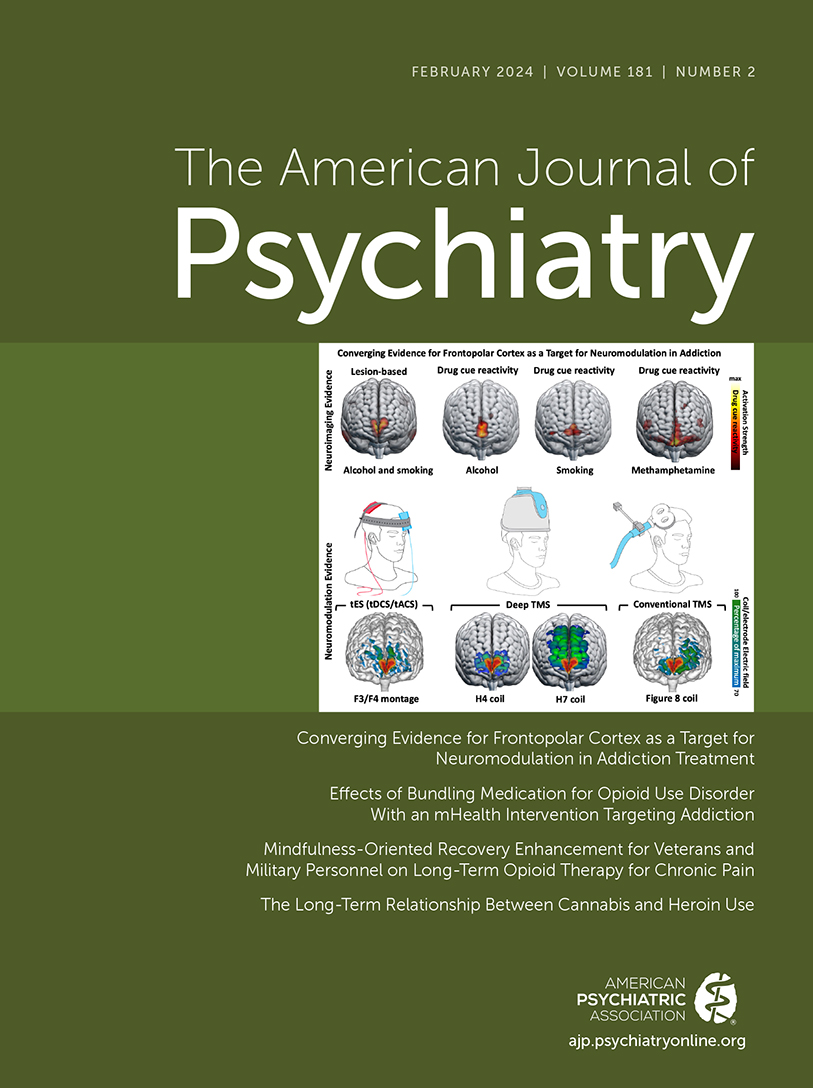
Journal, Garland et al. (
9) present a timely and relevant study targeting veterans and active-duty military personnel with chronic pain who were receiving opioid medications. This randomized controlled trial compared two psychosocial therapies, Mindfulness-Oriented Recovery Enhancement (MORE) and supportive group psychotherapy, adjunctive with opioid medication for chronic pain. This was a well-designed study with a number of strengths, including an ample sample size, a good comparator intervention, assessments conducted by staff blinded to the interventions, state-of-the-art assessments including ecological momentary assessment for opioid craving, intervention fidelity monitoring, and a relatively long follow-up of 8 months. The study has important implications for the use of this intervention with veterans with chronic pain who may be trying to reduce their use of medication without increasing pain severity. In this study, 34% of the enrolled veterans receiving long-term opioid therapy for chronic pain were diagnosed with an opioid use disorder. Veterans in this study had been receiving long-term opioid therapy for an average duration of 10–11 years and received average daily morphine equivalent doses over 100 mg, both of which are indictive of increased risk of opioid misuse or opioid use disorder. Session attendance (participants attended a mean of 5.5 MORE sessions and 5.7 supportive therapy sessions) for the two groups were similar and in line with group attendance in other mindfulness programs delivered remotely (
10). In this study, results showed that MORE outperformed supportive therapy, with statistically significant reductions in pain interference, pain severity, and opioid use. A recent meta-analysis of randomized controlled trials exploring the efficacy of MORE found small to moderate effect sizes favoring MORE in relation to addictive behaviors, craving, opioid dose reduction, chronic pain, and psychiatric symptoms (
11).
Negative emotional states and stressors can adversely affect pain perception, and individuals experiencing chronic pain have difficulty regulating emotional states, possibly because of a lack of interoceptive awareness capabilities. Individuals practicing mindfulness can enhance awareness of bodily sensations and stimuli through a process of reappraisal. Reappraisal and reinterpreting painful stimuli, stress, and craving through mindfulness practice result in improved self-regulatory processes and less emotional reactivity, while savoring natural positive rewarding experiences (
12). Interoceptive awareness, self-regulation, and adaptive reappraisal result in experiencing pain perception and stress in a more meaningful way. In another study comparing MORE to supportive therapy in a group of individuals with chronic pain receiving long-term opioid therapy, Roberts and colleagues (
13) found that improvements in reappraisal are mediated by interoceptive self-regulation and improvements in distress tolerance. The process variables explored in the Garland et al. study replicated the reappraisal and distress tolerance findings associated with MORE, which produced significant increases in mindful reinterpretation of pain sensations, nonreactivity to distressing thoughts and emotions, cognitive reappraisal, savoring or attending to pleasant natural reward stimuli, and attention to positive information. A subsample of veterans in the study participated in a natural reward stimuli task, before and after the intervention, in which physiological measurements were collected. Changes in EEG and skin conductance level measurements revealed that there was a greater positive response to natural reward stimuli in the MORE condition than in the supportive therapy condition. Furthermore, increased late positive potential on the EEG was associated with greater attention to savoring and decreased anhedonia (
14). It is not uncommon for veterans with chronic pain and mental health conditions, such as depression and posttraumatic stress disorder (PTSD), to be preoccupied with pain, depression, and traumatic experiences. Attention and focus on present-moment experiences and developing skills to reappraise pain sensory stimuli can raise pain tolerance and decrease pain perception, thereby reducing opioid use. As the authors state, veterans practicing mindfulness can reinstate natural reward circuits that have been adversely affected by long-term opioid therapy. This conclusion was validated by greater improvements in the secondary outcome factors (positive affect, anhedonia, savoring, and attention to positive information) that identify pathways to better clinical outcomes in veterans receiving MORE compared with those receiving supportive therapy. An earlier study comparing MORE to supportive therapy conducted in a primary care population of civilians (
15) validated the outcome variables studied by Garland et al. Considering that veterans often have clinically complex profiles, this finding has important implications for implementation in veterans and military populations who suffer from chronic pain and stress-related disorders. Mindfulness-based interventions similar to MORE are increasingly being integrated into the care of individuals with these disorders (
16). From 2012 to 2017, meditation practice among U.S. adults increased from 1.4% to 14.2% (
17).
Mindfulness interventions such as MORE, which are rooted in cognitive and behavioral psychology, use a present-moment, nonjudgmental approach that fosters awareness of both pleasant and unpleasant triggers, observing them for what they are and making well-informed responses. Mindfulness interventions are delivered in a group format with group members engaging in mindfulness meditation exercises, thereby experiencing and practicing the skill within the session, rather than being advised what skill may be helpful in a given triggering situation. In the context of mental health treatment, patients view mindfulness practice as useful and less stigmatizing than traditional therapies (
18). Mindfulness has also been shown to reduce self-stigma and shame, which are commonly experienced in veteran populations. A recent meta-analysis found that compassion-focused mindfulness interventions outperformed standard treatment and some active control interventions in reducing self-stigma (
19). In another study, mindfulness was shown to be negatively associated with self-stigma via reductions in PTSD symptom severity in a sample of U.S. veterans (
20). Moreover, self-compassion is also associated with reductions in functional disability (
21). Mindfulness meditation, a practice that promotes well-being and health, is appropriate for all individuals, but it can be particularly useful in patients with chronic pain on long-term opioid therapy and other stress-related disorders.
The authors have accumulated sufficient research findings favoring MORE that have implications for dissemination of this intervention into chronic pain clinics, opioid use disorder clinics, other substance use disorder treatment programs, and mental health programs where veterans commonly seek treatment. The scope of opioid misuse, opioid use disorder, and opioid overdose warrants novel effective treatments that can be delivered adjunctively with long-term opioid therapy. The addition or inclusion of mindfulness practices to various forms of psychotherapy, for example, dialectical behavior therapy and mindfulness-based cognitive therapy, have become established evidence-based interventions for a host of psychiatric disorders, and MORE promises to be a powerful tool in the fight against opioid misuse, opioid use disorder, and associated chronic pain.