Overview of Antidepressant Treatment of Bipolar Depression
Abstract
Introduction
Background
Status of Antidepressants for Bipolar Depression
Method
Results
| Trial | Bipolar types | Duration (wk) | Dropouts (%) | Antidepressant dose [mg/d (Imi-eq)] | Treatments | Responders/cases [n/N(%)] | |
|---|---|---|---|---|---|---|---|
| Antidepressant | Placebo | ||||||
| Cohn et al. (1989) | I + II | 6 | 53.9 | 50 (250) | Flx vs. Pbo ± Li | 26/30 (86.7%) | 11/29 (37.9%) |
| Cohn et al. (1989) | I + II | 6 | 53.9 | 188 (188) | Imi vs. Pbo ± Li | 17/30 (56.7%) | 11/29 (37.9%) |
| Nemeroff et al. (2001) | I + II | 10 | 23.3 | 33 (165) | Li ± ACs: + Prx vs. Pbo | 15/33 (45.5%) | 15/43 (34.9%) |
| Nemeroff et al. (2001) | I + II | 10 | 23.3 | 167(167) | Li ± ACs: + Imi vs. Pbo | 14/31 (45.2%) | 15/43 (34.9%) |
| Tohen et al. (2003) | I + II | 8 | 33.9 | 39 (195) | OFC vs. Pbo | 46/82 (56.1%) | 108/355 (30.4%) |
| Shelton and Stahl (2004) | I + II | 12 | 40.2 | 28 (140) | MS + Prx ± Rsp vs. Pbo ± Rsp | 5/20 (25.0%) | 3/10 (30.0%) |
| Agosti and Stewart (2007) | II | 6 | 6.0 | 255 (255) | Imi vs. Pbo | 13/23 (56.5%) | 5/22 (22.7%) |
| Agosti and Stewart (2007) | II | 6 | 6.0 | 65 (162) | Pnz vs. Pbo | 13/25 (52.0%) | 5/22 (22.7%) |
| Sachs et al. (2007) | I + II | 12 | 56.8 | 300 (165) or 30 (150) | Bup or Prx + MS vs. Pbo + MS | 42/179 (23.5%) | 51/187 (27.3%) |
| McElroy et al. (2010) | I + II | 8 | 33.9 | 20(100) | Prx vs. Pbo | 65/118 (55.1%) | 64/121 (52.9) |
| Overall (n = 10 trials) | I + II | 8.4 ± 2.5 | 34.2 ± 18.4 | 179 ± 47 (Imi-eq) | Antidepressants ± Others vs. Pbo | 256/571 (44.8%) | 288/861 (33.4%) |
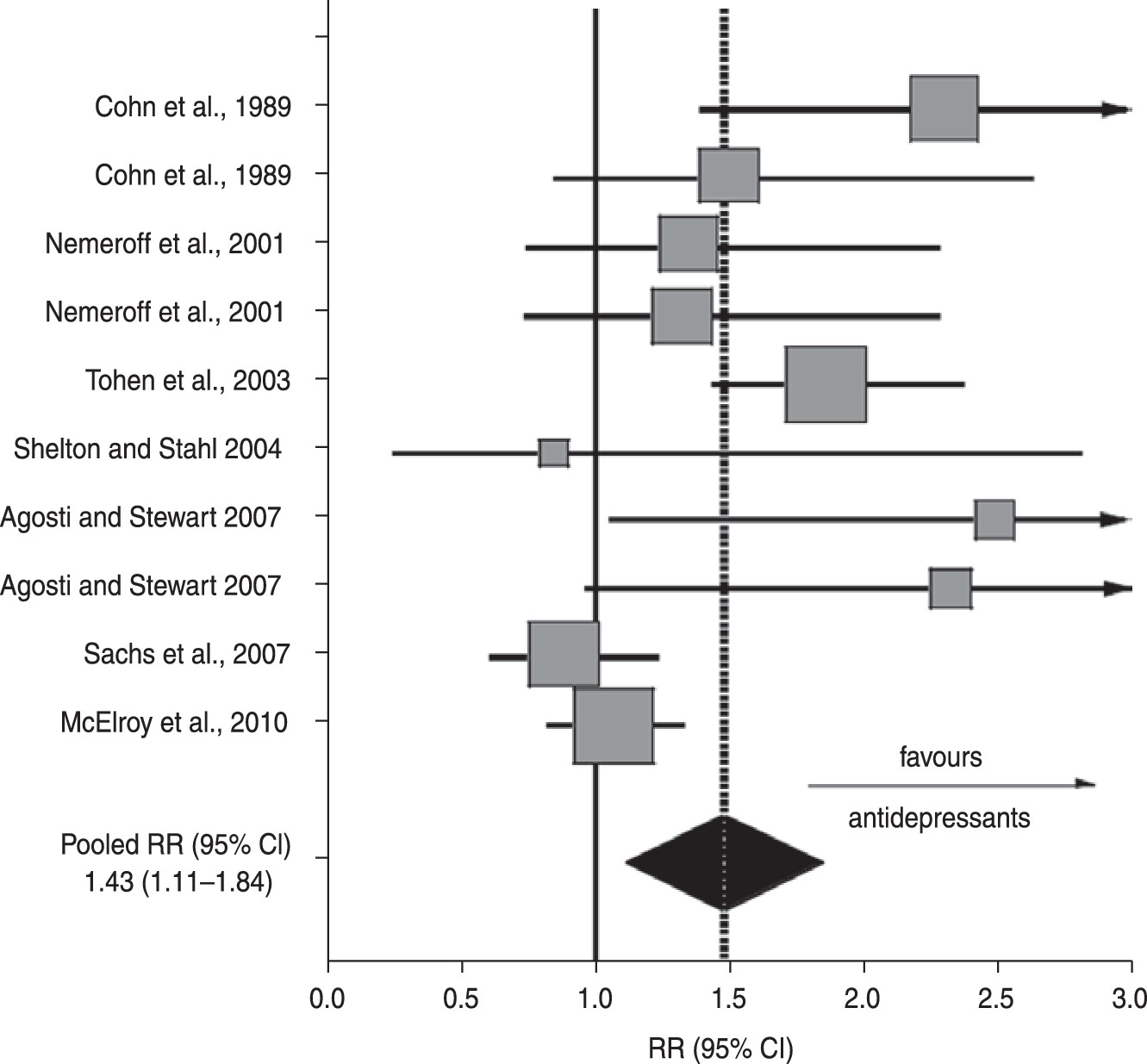
| Measure (95 %CI) | ||
|---|---|---|
| Measures | Bipolar | Unipolar |
| Trials | 10 | 142 |
| Antidepressant/control RR | 1.43 (1.11–1.84) | 1.42 (1.38–1.48) |
| Antidepressant/control RD | 0.164 (0.049–0.280) | 0.125 (0.111–0.141) |
| NNT | 6.2 (3.6–6.7) | 8.0 (7.1–9.1) |
Discussion
Antidepressant Responses
Risks of Mood ‘Switching’
| Agents | Indications in BD | Status for bipolar depression | References |
|---|---|---|---|
| Antidepressants | None for BD; indication for ‘major depression’ widely assumed to include bipolar depression | Clinically used | Amit and Weizman (2012), Sidor and MacQueen (2011, 2012) |
| Aripiprazole | Mania, mixed-states and recurrences | Mainly negative findings; not approved for bipolar depression | Thase et al. (2008); Cruz et al. (2010), De Fruyt et al. (2012) |
| Asenapine | Mania, mixed-states | Experimental; some evidence | Cruz et al. (2010), De Fruyt et al. (2012) |
| Carbamazepine | Mania or mixed-states | Not approved for bipolar depression | Reinares et al. (2012) |
| Deep brain stimulation | Treatment-resistant depression | Experimental; some evidence | Rizvi et al. (2011) |
| Dopamine agonistsa | Proposed for bipolar depression | Experimental; some evidence | Howland (2012) |
| Divalproex | Mania | Not approved for bipolar depression | Reinares et al. (2012) |
| Electroconvulsive treatment | Major and bipolar depression; mania | Clinically used; FDA Class III medical device | Dierckx et al. (2012) |
| Gabapentin | None for BD | Not approved for bipolar depression | Reinares et al. (2012) |
| Glutamate NMDA-antagonistsb | Treatment-resistant & bipolar depression | Experimental; some evidence | Owen (2012), Zarate et al. (2012) |
| Lamotrigine | Recurrences (mainly vs. depression) | Not approved for bipolar depression | Reinares et al. (2012) |
| Levetiracetam | None for BD | Not approved for bipolar depression | Saricicek et al. (2011) |
| Light therapy (intensive) | Depression, seasonal affective depression | Experimental | Poon et al. (2012) |
| Lithium salts | Mania, recurrences | Not approved for bipolar depression | Baldessarini (2013) |
| Lurasidone | Mania | Not approved for bipolar depression | De Fruyt et al. (2012) |
| Modafinil, R-modafinil | None for BD | Experimental; some evidence | Frye et al. (2007); Calabrese et al. (2010) |
| Olanzapine | Mania, mixed-states, maintenance | Some evidence; approved in Japan | Cruz et al. (2010), De Fruyt et al. (2012), Tohen et al. (2012) |
| Olanzapine+Fluoxetine | Treatment-resistant and acute bipolar depression | FDA-approved | Cruz et al. 2010, De Fruyt et al. 2012 |
| Omega-3 fatty acids and other ‘nutriceuticals’ | Proposed for bipolar depression | Experimental; some evidence | Keck et al. (2006), Sarris et al. (2011), Torrey and Davis (2012) |
| Pregabalin | None for BD | Experimental; some evidence | Reinares et al. (2012) |
| Psychostimulantsc | Proposed adjuncts | Experimental | Parker and Brotchie (2010); Howland (2012) |
| Psychosocial interventions | Major depression; maintenance treatment | Clinically used | Fountoulakis (2010), Lolich et al. (2012) |
| Quetiapine | Mania, mixed-states, acute bipolar depression; long-term with lithium or valproate | FDA-approved | Cruz et al. (2010), De Fruyt et al. (2012) |
| Repeated transcranial magnetic stimulation | Major depression | Experimental | George et al. (2013) |
| Risperidone, Paliperidone | Mania, mixed-states, maintenace (risperidone) with lithium or valproate | Experimental; some evidence | Cruz et al. (2010), De Fruyt et al. (2012) |
| Sleep deprivation | Major depression | Experimental | (Poon et al. 2012) |
| Thyroid hormones | Proposed for bipolar depression | Experimental | Bauer et al. (2005a, b) |
| Topiramate | None for BD | Not approved for bipolar depression | Reinares et al. (2012) |
| Vagal nerve stimulation | Chronic or recurrent depression | FDA-approved | Rizvi et al. (2011) |
| Ziprasidone | Mania, mixed-states, maintenance with lithium or valproate | Experimental; some evidence; not recommended for bipolar depression | Cruz et al. (2010), De Fruyt et al. (2012), Yatham et al (2013) |
Conclusions
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).