Once thought to be relatively rare, obsessive-compulsive disorder (OCD) is now believed to be one of the more common psychiatric disorders, with an estimated lifetime prevalence of approximately 2% (
1–
4). Increased understanding of this disorder has led to a modification of the structure of the most recent version of the
DSM-5. In past editions of the
DSM, OCD was considered an anxiety disorder. Although anxiety is still considered a central feature, OCD—along with the related disorders of trichotillomania, skin picking, body dysmorphic disorder, and hoarding—has been given its own section in
DSM-5: Obsessive-Compulsive and Related Disorders (
5). This significant modification distinguishes OCD as a unique mental disorder and will hopefully result in increased clinical attention.
Diagnosis and Assessment
The diagnostic criteria for OCD in
DSM-5 remain largely the same as in
DSM-IV, requiring either obsessions or compulsions.
Obsessions are defined as 1) “recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress” and 2) “the individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some other thought or action (i.e., by performing a compulsion).”
Compulsions are defined as “repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly” that are “aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive.... The obsessions or compulsions are time-consuming, taking more than 1 hour per day, or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.” (
5) The major change in the
DSM-5 criteria for OCD is the addition of two specifiers for this diagnosis: insight and tic-related disorder.
The first specifier concerns the level of insight the patient possesses, defined as the degree to which individuals with OCD find their obsessions and related compulsions to be reasonable.
DSM-5 recognizes that patients with OCD may have varying degrees of insight, ranging from
absent insight/
delusional beliefs at one extreme, with the individual “completely convinced that [OCD] beliefs are true,” and
good or
fair insight, with the individual recognizing that OCD beliefs “are definitely or probably not true.”
DSM-5 also allows for the level of
poor insight, in which “the individual thinks [OCD] beliefs are probably true.” (
5) It has been recognized for some time that the degree of insight may vary during a single episode and across episodes (
6), yet the etiology underlying these variations is unclear. Although research findings are mixed, poor insight has been associated with earlier age of onset (
7,
8), longer illness duration (
7,
8), greater severity of symptoms (
9–
12), and an increased comorbidity with major depression (
8,
12).
The Yale-Brown Obsessive Compulsive Scale (YBOCS) (
13) remains the gold standard for the assessment of OCD symptom severity and contains an item on degree of insight, measured on a 0–4 scale, to aid clinicians with the often difficult task of assessing the strength of patients’ conviction regarding the necessity of their obsessive-compulsive behavior [available in print from Goodman et al. (
13)]. An additional assessment instrument, the Brown Assessment of Beliefs Scale (BABS), has been developed to provide a measure of insight (available for download at
www.rhodeislandhospital.org/services/body-dysmorphic-disorder-program/questionnaires.html) (
14). This semistructured interview includes seven items to assess the degree of conviction, perceptions of others’ views of the belief, degree of fixedness, and awareness that the obsessions and compulsions are caused by a mental disorder. The rating is on a 0–24 scale; only six items are used to calculate the total score. Using BABS, one study of 211 outpatients with OCD found 2.4% of these patients to have delusional beliefs (score >18) and 13.3% to have poor insight (score 13–17), whereas the remaining patients were approximately evenly split between fair (28.9%, score 8–12), good (26.5%, score 4–7), and excellent (28.9%, score 0–3) insight (
15).
As mentioned earlier, the
DSM-5 includes not one, but two new specifiers for OCD. The second specifier is for the presence of a tic disorder, which is coded as “tic-related” if “the individual has a current or past history of tic disorder.” (
5) One study estimated that 30%–50% of children with tic disorder will go on to have OCD (
16). Tic disorder and OCD appear to be genetically related disorders, as there is an increased incidence of tic disorder and OCD in first-degree relatives of patients with either of these disorders (
17,
18). It has been suggested that tic disorder may actually be an alternate expression of genetically transmitted OCD (
19). The addition of the tic specifier is useful, as the co-occurrence of OCD and tic disorder may have treatment implications. Patients with OCD and comorbid motor tics were less likely to respond to fluvoxamine in two studies (
20,
21). The presence of a tic disorder has not been found to reduce the efficacy of clomipramine (
22) or fluoxetine for OCD (
23). In patients with Tourette’s disorder, selective serotonin reuptake inhibitors (SSRIs) appear to have little if any effect on tic symptoms. In patients with OCD and tic disorder, antipsychotic augmentation is a reasonable strategy, as it may treat both disorders simultaneously (
24,
25).
Differentiating Symptoms of OCD From Those of Other Disorders
It is important to distinguish the absent insight and delusional beliefs of OCD from the delusions present in psychotic disorders, as OCD may closely resemble psychosis. The major feature distinguishing the absent insight/delusional beliefs of OCD from schizophrenia is that the OCD compulsion is performed in an effort to reduce anxiety provoked by a thought, image, or impulse. The presence of hallucinations, disorganized speech, and affective flattening should alert the clinician to the likelihood of schizophrenia rather than OCD. In addition, although patients with OCD may have difficulty fully verbalizing the phenomenology of their obsessions and compulsions, disorganized speech will not be present. There is some co-occurrence of OCD and schizophrenia, with one study estimating that approximately 12% of patients with schizophrenia have comorbid OCD (
26).
Given that OCD with poor insight and delusional beliefs may closely resemble schizophrenia, some work has been done to distinguish these two disorders. One study found that patients with OCD and poor insight (operationalized as high scores on the Overvalued Ideas Scale) displayed executive dysfunction intermediate between patients with schizophrenia and patients without poor insight (
27). A second study replicated these results, finding that patients with OCD and poor insight exhibited better performance compared with schizophrenia patients on some subscales of the Wisconsin Card Sorting Test and the Trail Making Test but exhibited worse performance compared with patients with OCD and fair or good insight. In addition, patients with OCD and poor insight exhibited worse performance on the verbal memory process than did patients without poor insight (
28).
Another disorder that is important to differentiate from OCD is obsessive-compulsive personality disorder (OCPD). The main symptoms that should allude to OCPD are the patient’s egosyntonic thoughts about perfectionism and rigidity in behavior. According to the
DSM-5 criteria, the OCPD individual is “1) preoccupied with details, rules, lists, order, organization, or schedules to the extent that the major point of the activity is lost, 2) shows perfectionism that interferes with task completion, 3) is excessively devoted to work and productivity to the exclusion of leisure activities and friendships, 4) is overconscientious, scrupulous, and inflexible about matters of morality, ethics, or values, 5) is unable to discard worn-out or worthless objects, even when they have no sentimental value, 6) is reluctant to delegate tasks or to work with others unless they submit to exactly their way of doing things, 7) adopts a miserly spending style toward both self and others, and 8) shows rigidity and stubbornness” (
5).
Although
DSM-5 indicates that social and occupational dysfunctions are necessary criteria for OCD, in contrast to OCPD, OCD does not include criteria specifically regarding the prominence of work in the self-identity of the patient with OCD. Lack of empathy and lack of intimacy are also not part of the criteria for OCD. However, OCD does appear to negatively affect romantic relationships, as it has been found to be more prevalent in divorced/separated individuals than in those who are married (
2). It is important to note that
DSM-5 no longer uses the five-axis diagnostic system; personality disorders are now considered a primary diagnosis.
A final disorder that should be differentiated from OCD is impulse control disorder. Patients with OCD do, by definition, have trouble controlling their compulsive behavior. In a study of 96 patients with OCD, 5.3% met criteria for compulsive gambling, 4.3% met criteria for intermittent explosive disorder, and 2.1% met criteria for pyromania (
29). The important distinction between OCD and impulse control disorders is that in OCD, the compulsive behavior in response to a thought, image, or impulse is considered
unacceptable to the patient. The thoughts, images, or impulses in impulse control disorder are
egosyntonic, whereas the thoughts, images, and impulses of OCD are
egodystonic (
30).
Pathophysiology
The pathophysiology of OCD from a genetic standpoint is discussed in this issue of
Focus by Drs. Sobell, Pato, Pato, and Knowles. Results of studies of genetic differences in individuals with OCD have most consistently implicated polymorphisms of the glutamate receptor gene, specifically the
SLC1A1 coding region located on chromosome 9 (
34,
35). The
SLC1A1 gene encodes the glutamate transporter known as the excitatory amino acid carrier 1, which is found in the cortex, thalamus, basal ganglia, hippocampus, and cerebellum (
36–
38).
Products of genes associated with OCD may affect specific brain regions. Despite the somewhat inconsistent findings of structural neuroimaging studies, it would appear that the brain regions most involved in OCD are those that assist with regulation of emotion and cognitive control, and the alterations in these structures potentially mediate the anxiety and misappraisal of threat exhibited by those with OCD. It remains to be determined whether these structural differences are the underlying cause of OCD symptoms or are products of persistent obsessive cognitions and compulsive behaviors. As noted below, the heterogeneity of OCD symptoms, as well as psychiatric illnesses comorbid with OCD, may mediate the discrepancies among the findings of the individual studies.
The neuroanatomy of OCD has been the focus of intense research. However, findings have been somewhat inconsistent, with studies reporting smaller (
39–
41), larger (
42–
44), or normal (
45–
47) volumes of overall, white, and gray matter in various regions of the brains of patients with OCD relative to control participants.
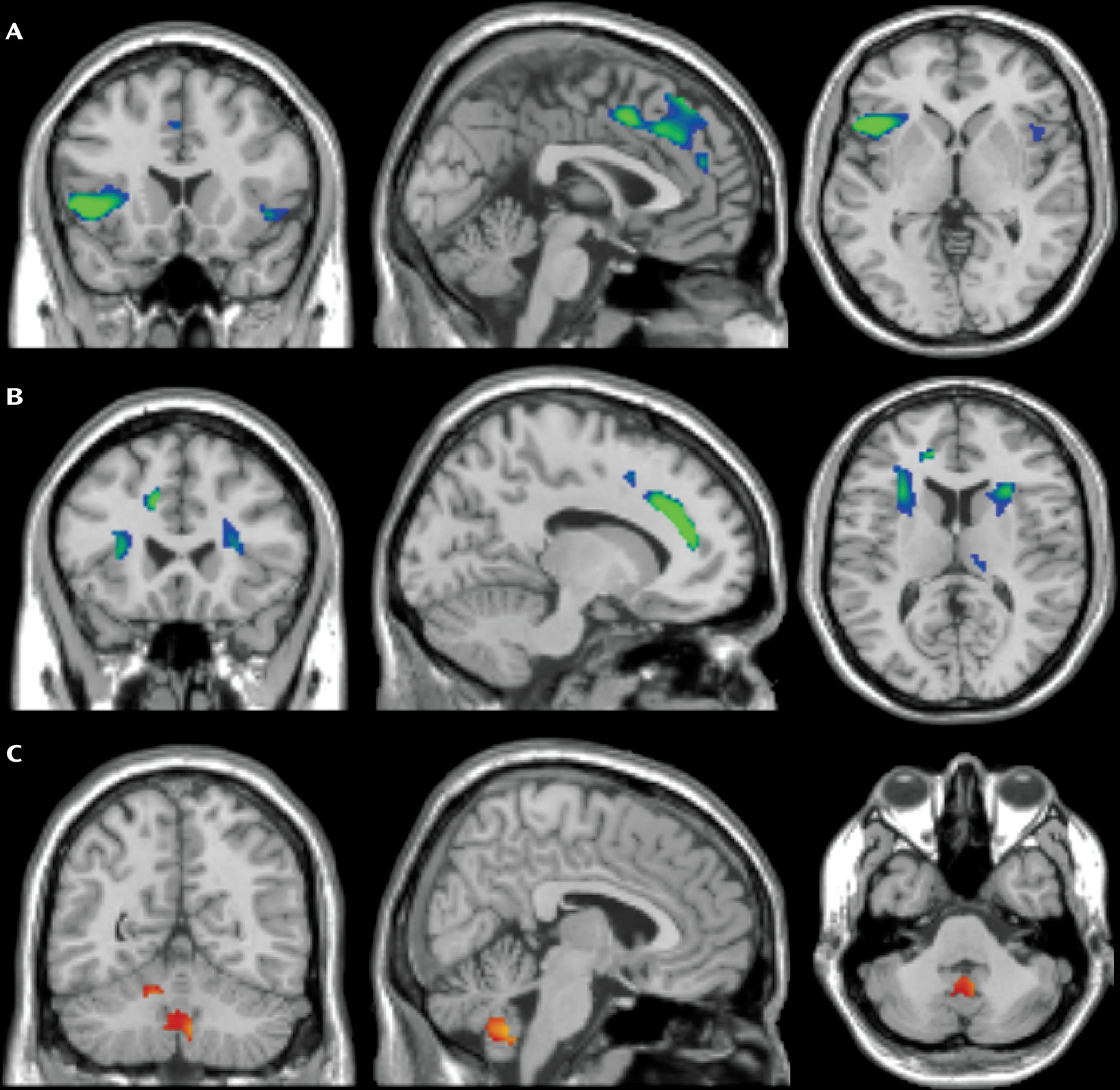
Meta-analytic research has synthesized the discrepant results, finding a smaller combined (white+gray matter) volume of the anterior cingulate cortex (ACC) (
48,
49) and orbitofrontal cortex (OFC) (
49), and an increased combined thalamic volume (
49) in patients with OCD relative to control participants. Although data are very limited, increased combined thalamic volume has been found to correlate with an increased severity of obsessions and compulsions (
49).
Gray matter density has been found in meta-analyses to be reduced in the dorsolateral prefrontal cortex (
50), OFC (
50), dorsomedial prefrontal cortex (DMPFC) (
48), and ACC (
48,
51) in patients with OCD relative to control participants. In contrast, gray matter density has been found to be greater in the putamen (
50), caudate (
51), and anterior prefrontal cortex (
50,
51) in patients with OCD relative to control participants. In addition to gray matter reductions, white matter density was found to be reduced in the DMPFC and ACC in a recent mega-analysis (reanalysis of a random sampling of previously collected data) (
48). Neuroimaging researchers have suggested that specific neuroimaging techniques may significantly affect study findings and may be partially responsible for discrepancies among studies (
52).
As a visual aid, neuroanatomy imaging from a recent mega-analysis (
48) is presented in
Figure 1. In addition,
Table 1 provides a summary of the findings from meta-analytic studies.
Perhaps more important than the brain volumetric correlates of OCD may be the functional connections between the implicated neuroanatomical areas, referred to as the
cortico-basal ganglia–thalamocortical circuitry and the
corticostriatal-thalamocortical circuitry. (Note: The striatum consists, in part, of the caudate and putamen, which are also areas contained within the basal ganglia.) Through the use of functional MRI, an increased degree of coordinated activity, known as
hyperconnectivity, has been demonstrated to occur between the ventral caudate/putamen/nucleus accumbens and the anterolateral and medial orbitofrontal cortices in patients with OCD, with the magnitude of coordinated activity predictive of symptom severity (
53–
58). Some evidence exists that serotonergic antiobsessional medications may improve OCD symptoms through a reduction of hyperconnectivity (
58).
Two neuroanatomical areas appear to be of particular importance from a functional neuroimaging standpoint. The degree of hyperactivity in the OFC is considered by many researchers to be predictive of OCD global symptom severity (
57–
64). In the ACC, functional neuroimaging studies have shown elevated metabolism in individuals with OCD at rest and during symptom provocation (
65–
67).
Although differences in imaging techniques may partially explain the discrepant findings of neuroimaging studies, it seems possible for neuroanatomical findings in OCD to differ depending on specific OCD symptom type. Some researchers believe that OCD neuroanatomy may be better understood if OCD is considered a clinically related group of symptom dimensions rather than as a simple construct of obsessions and compulsions (
68,
69). Consistent with this assessment, structural and functional neuroimaging studies have suggested that partially distinct neuroanatomy and neural pathways may be present depending on the specific OCD symptoms (
54,
70–
72).
Structural neuroimaging studies have suggested that reductions in temporolimbic (amygdala) volume may be associated with aggressive obsessions and checking compulsions (
39,
73). Alterations in volumes of gray matter and white matter of various other regions of the brain have been associated with varying categories of obsessions in individual studies, but these findings await further substantiation through replication (
74,
75). Somewhat more broadly, it has been suggested that the obsessional component of OCD may be associated with white matter reductions in the cingulate bundle and corpus callosum (
76).
In terms of functional neuroimaging, aggressive obsessions have been positively associated with greater connectivity between the ventral caudate and ventral medial frontal cortex, whereas sexual and religious obsessions have been associated with greater connectivity between the ventral caudate connectivity and the mid- and anterobasal insular cortex (
53).
Another variable that may mediate the discrepant neuroimaging findings is that of frequent comorbidity of OCD with other psychiatric disorders. Patients with OCD and comorbid disorders are sometimes the intended focus of research (
77,
78), but inadvertent inclusion of individuals with comorbidities, or difficulty in parceling out the independent effects of comorbidities, may lead to the discrepancies among neuroimaging studies. For example, major depressive disorder shares many neuroanatomical findings with OCD (
79,
80). However, neuroanatomical concordance of these disorders is likely less than complete, and inclusion of depressed patients in OCD imaging studies may be a variable leading to difficulty in the interpretation of results of many neuroimaging studies. Functional neuroimaging has been useful in distinguishing OCD from commonly comorbid major depressive disorder, finding that although both disorders share decreased activation of the prefrontal cortex during a task-switching exercise, only patients with OCD exhibited increased activation of the caudate, ACC, and insula (
81).
Surgical Treatment
Several treatment strategies based on neuroanatomical correlates of OCD have been developed for patients whose condition is refractory to multiple trials of pharmacotherapy and psychotherapy. The first neurosurgical procedure specifically designed for OCD symptoms refractory to psychotropic medication and psychotherapy was stereotactic anterior cingulotomy, which was developed at Massachusetts General Hospital in the 1960s (
82). This procedure continues to be an effective treatment (
83,
84) and has been shown recently to have long-lasting positive effects, with a 35% reduction of YBOCS in 47% of patients at approximately 5 years in a recent study (
85). Other surgical treatments of OCD include anterior capsulotomy, subcaudate tractotomy, and a combination of these two procedures known as
limbic leukotomy (
85). However, such procedures are invasive and irreversible. Gamma knife radiosurgery, also known as
radioablative surgery, is a procedure that has been used since 1953 for the treatment of OCD, with mixed results (
86). Until recently, the data on this procedure consisted of case reports, case series, and retrospective methods. However, a small randomized placebo-controlled trial of 16 patients recently found benefit of ventral capsulotomy with the gamma knife procedure (
87).
A newer surgical treatment option that has yielded promising results thus far is stereotactic deep brain stimulation (DBS) (
88–
91), which was approved by the U.S. Food and Drug Administration (FDA) in 2008 for the treatment of OCD. The procedure involves the use of MRI to determine the location, the drilling of a small burr hole in the skull, and advancement of an electrode 1.27 mm in diameter (the approximate size of 7 strands of human hair) into the targeted structure (
92). Studies have placed the electrode in various neuroanatomical locations, including the internal capsule/ventral striatum, nucleus accumbens, subthalamic nucleus, or inferior thalamic peduncle. All of these neuroanatomical placements have been associated with significant reductions of OCD symptoms (
92). No single optimal location has yet been identified. This is, at least in part, because of the relatively small amount of data on the use of this procedure for OCD. It is estimated that DBS outcomes have been reported in the literature for only approximately 90 patients with OCD (
92). It is possible that certain locations may be more or less effective for specific OCD symptoms. DBS for OCD appears to possess efficacy similar to that of ablative procedures, such as anterior cingulotomy (
85). Effects of DBS appear to be long-lasting, with gains maintained at 2–3 years (
84,
93).
DBS possesses the advantage of reversibility, by the ability to turn on and then turn off electrical stimulation. This reversibility provides an opportunity to study the neuroanatomical functioning of individuals with OCD with DBS “off” and “on,” allowing for demonstration of the efficacy of DBS in the subthalamic nucleus in double-blinded conditions (
94). Positron emission tomography has shown a reduction of activity in the left cingulate gyrus and left frontal medial gyrus relative to baseline in patients with OCD when DBS is in the “on” mode. A decrease in metabolism in the prefrontal cortex, specifically the OFC, correlated with a decrease in YBOCS scores (
95). DBS appears to be a very promising option for treatment-resistant patients. Given the invasive nature of DBS, this procedure is reserved for patients whose condition has failed adequate trials of cognitive-behavioral therapy (CBT) and at least three medication trials.
Pharmacological Treatment
Pharmacological treatment of OCD continues to involve SSRIs and clomipramine as mainstays (
96,
97). APA has developed practice guidelines for OCD. At this time, five FDA-approved medications are available for treatment of OCD in adults: sertraline, fluoxetine, fluvoxamine, paroxetine, and clomipramine. A meta-analysis reports equal efficacy across the FDA-approved SSRIs (
98). A new controlled-release formulation of fluvoxamine appears to allow a quicker dose titration than the immediate-release formulation (
99).
Citalopram, although not approved by the FDA for the treatment of OCD, was found to have an efficacy equal to that of the FDA-approved SSRIs in a meta-analysis (
98). Escitalopram, the
S-enantiomer of citalopram, has shown efficacy in recent open-label trials (
100,
101) as well as in randomized placebo-controlled trials (
102,
103). The efficacy of escitalopram has been noted to be equal to that of paroxetine, with fewer medication side effects (
102). On the basis of these findings, the APA practice guideline for OCD includes citalopram and escitalopram as potential first-line medications for the treatment of OCD (
97). Because of concerns for QTc prolongation, the FDA maximal recommended dose of citalopram has been lowered to 40 mg/day (20 mg/day in those >60 years of age). However, recent research has challenged this recommendation, noting that the QTc prolongation associated with citalopram may be no worse than that seen with other SSRIs (
104). Escitalopram does not carry the same warning regarding QTc prolongation in the United States, but the drug regulatory administration in the United Kingdom has applied this warning (
105). The maximal FDA-recommended daily dose of escitalopram is not more than 20 mg.
Discontinuation rates because of undesirable side effects appear to be higher with clomipramine than with SSRIs (
106–
109), with weight gain from clomipramine being one of the main side effects (
110). Therefore, treatment guidelines recommend a trial of the FDA-approved SSRIs before the use of clomipramine (
96,
97). Although meta-analyses suggest that clomipramine may be superior to the SSRIs (
111–
117), direct-comparison trials of clomipramine and SSRIs indicate equal efficacy (
109,
118,
119).
Patients with OCD have been found to often require medication doses beyond the maximum approved by the FDA (
96,
97,
120), and it is recommended that the duration of a given medication trial be 8–12 weeks total, with 4–6 weeks at the maximal tolerable dose (
96,
97,
101,
121,
122). In the case of symptom remission, current treatment guidelines recommend continuation of medications for 1–2 years before initiation of a taper during several months to discontinuation (
96).
Although serotonergic/noradrenergic medications are an effective treatment for some patients, many individuals remain refractory to treatment, with some estimates as high as 50%−60% (
96,
123). Before modifying therapy, it may be prudent to inquire about medication compliance and to consider whether a patient may possess CYP enzymes that rapidly metabolize medications. Before testing for CYP enzyme activity, the clinician can consider a trial of medication metabolized through an alternate CYP pathway.
We discussed the degree of patients’ insight earlier in this article. The prognostic value of insight is unclear at this time and requires more research. Some studies have found poorer insight to be associated with poorer treatment response to medication and psychotherapy [Matsunaga et al. (
7), Ravi Kishore et al. (
8), Jakubovski et al. (
10), Erzegovesi et al. (
124), Eisen et al. (
125), Alonso et al. (
126)]. This is potentially mediated by the degree of interest in, involvement in, and adherence to treatment. The clinician may be required to exert additional efforts to determine interest and involvement in pharmacological and psychotherapeutic treatment plans and adherence to medication recommendations when working with patients with absent insight or delusional beliefs. It is also worth noting that insight may vary in repeated episodes of illness. There has not been systematic study of the interplay between medication response and the degree of insight across multiple episodes. (See articles in this issue of
Focus on body dysmorphic disorder, hoarding, and skin picking and trichotillomania for discussion of the role of insight and treatment response.)
OCD Refractory to Initial Pharmacological Management
The APA practice guidelines provide additional treatment strategies based on the response to the initial medication trial. For those with moderate response, defined as a clinically significant, but inadequate, response after a 12-week trial of the initial medication, augmentation with a second-generation antipsychotic drug is recommended. This recommendation is supported by meta-analytic data (
127,
128), and approximately one-third to one-half of patients will respond to this augmentation strategy (
25,
128). It is recommended that the length of a trial of augmentation with an atypical antipsychotic drug be in the range of 2–8 weeks.
Currently, insufficient data are available to determine which member of this class of medications possesses superior efficacy, although at least one randomized controlled trial (RCT) has shown efficacy for haloperidol, risperidone, quetiapine, olanzapine, and aripiprazole (
129). No RCTs exist that have examined the efficacy of ziprasidone. Of the newer atypical antipsychotic drugs asenapine, lurasidone, iloperidone, and paliperidone, only paliperidone has been examined in a double-blind, placebo-controlled trial, with a nonsignificant trend toward improvement in OCD symptoms (
130).
Head-to-head comparator studies are few, but quetiapine was found to be superior to ziprasidone in a study of 24 patients (
131). Risperidone and haloperidol appear to have equal efficacy; however, haloperidol may be more useful in the presence of a comorbid tic disorder (
20), whereas risperidone may be more useful in patients with comorbid depression (
132). Risperidone was found to be superior to aripiprazole in a study of 41 patients (
133) and to have an efficacy equal to that of olanzapine in a study of 50 patients (
134).
The pharmacological mechanism through which the atypical antipsychotic drugs exert their anti-OCD effect is unclear but may be related to 5-hydroxytryptamine 1A (5-HT
1A) partial agonism, which results in increased levels of serotonin. Given the efficacy of haloperidol, which has no serotonin receptor affinity, it is possible that dopamine blockade also mediates the efficacy of the antipsychotic medications. Some meta-analytic evidence supports this notion in that risperidone, the second-generation antipsychotic drug with the most potent D
2 receptor blockade, may be the most efficacious of the class (
127). It is possible that patients with OCD and absent insight or delusional beliefs may particularly benefit from augmentation with antipsychotic medication. However, this is a speculative assessment, and more research is thus needed to support it.
If little or no response is evident with the initial SSRI, recommended options are to conduct a trial with 1) an alternate SSRI, mirtazapine, venlafaxine, or clomipramine as monotherapy or 2) second-generation antipsychotic drugs in augmentation of the initial SSRI. Mirtazapine has been found to accelerate the response to citalopram in a single-blind randomized augmentation study (
135) and showed some efficacy in a discontinuation trial (
136). Venlafaxine has shown mixed results, with no difference from placebo in one double-blind, placebo-controlled study (
137), yet its efficacy was relatively equal to that of paroxetine (
138,
139) and clomipramine (
140) in double-blind comparator studies.
Should the aforementioned treatment strategies result in an inadequate reduction of symptoms, the APA practice guidelines recommend a trial of augmentation with an alternate second-generation antipsychotic drug, a monotherapy trial of an alternate serotonin reuptake inhibitor, or augmentation with clomipramine, although clomipramine has limited supporting evidence.
Before concluding that a trial of clomipramine has been ineffective in monotherapy or in augmentation, the clinician can obtain a plasma level to determine that dosing is adequate. The clinician should be cognizant of the potential for cardiac complications when coadministering clomipramine with potent CYP 2D6 inhibitors, such as fluoxetine, paroxetine, and bupropion, as serum levels of clomipramine can become supratherapeutic, resulting in QTc prolongation. Thus, monitoring plasma levels of clomipramine is of considerable importance when such a strategy is implemented.
Additional Treatment Strategies
Once a practitioner has exhausted the previously discussed treatment strategies, options with less empirical evidence can be tested in trials. These options and supporting evidence are reviewed below.
Other medications exerting effects through 5-HT
1A antagonism that may be useful as augmentation strategies in the treatment of OCD are buspirone and pindolol. Results of a double-blind, RCT found buspirone monotherapy to have an efficacy equal to that of clomipramine (
141). However, studies have found poor efficacy of buspirone as an augmenting agent (
21,
142,
143). Few studies of pindolol, a medication with potent presynaptic 5-HT
1A antagonism, have been performed, but we found some evidence for efficacy in a recent meta-analysis (
144). Although the overall results of this meta-analysis were statistically significant, results were equivocal when only placebo-controlled trials were examined (
144).
In recent years, and parallel to the finding of a likely genetic influence of glutamate transporter polymorphisms, medications operating through the glutamate system have received increasing attention. One theory to explain the reduced volumes of cortical and subcortical structures reported on neuroimaging of OCD is that hypofunctioning glutamate transporters lead to increased extracellular glutamate concentrations, which in turn cause excitotoxicity and cell death in adjacent neurons (
145,
146). Memantine is the best studied of the medications involving the glutamate system. To date, three observational studies (
147–
149) and one randomized placebo-controlled trial (
150) have examined memantine for the treatment of OCD, all with positive results. Although its mechanism of action is not yet completely understood but likely reduces presynaptic release of glutamate (
151), riluzole has shown promise in two open-label case studies (
152,
153).
N-acetylcysteine, an amino acid compound with complex actions via the glutamate neurotransmitter system, has shown some promise as a treatment of trichotillomania, and a recent case report suggests that this agent may be useful in OCD as well (
154). Ketamine, a noncompetitive
N-methyl-
d-aspartic acid (NMDA) glutamate receptor antagonist, was associated with a small reduction of OCD symptoms in an open-label trial (
155). Three studies have examined
d-cycloserine, a partial agonist at the glycine unit of the NMDA receptor, as an agent to hasten response to ERP therapy (
156–
158). One of these studies found a positive effect, although this effect was not sustained to the end of therapy (
158). Glycine itself was shown to have efficacy in a randomized, double-blind, placebo-controlled trial; however, it appeared to be poorly tolerated because of nausea and/or aversive taste (
159). A full discussion of glutamate and glycine is beyond the scope of this article, and we refer the reader to chapters 2, 3, and 4 of Stahl (
160) for a review.
Monoamine oxidase inhibitors have not been studied extensively as a treatment of OCD. Phenelzine was found to be effective in an open-label case series of patients with OCD and comorbid phobia and anxiety (
161), yet it was shown to be inferior to fluoxetine in a randomized placebo-controlled study (
162). An earlier double-blind study found equal efficacy for clomipramine and phenelzine (
163).
Ondansetron, a 5-HT
3 antagonist, showed some efficacy in a randomized, placebo-controlled trial of fluoxetine augmentation (
164) and in an open-label study (
165). However, as noted in the update of the APA practice guidelines (
97), the result of a placebo-controlled trial sponsored by the manufacturer of ondansetron was negative. Ondansetron may be particularly useful as an augmentation strategy when nausea associated with serotonergic medication is present.
Many additional treatment strategies have been attempted. In brief, lamotrigine (
166), topiramate (
167,
168), oral morphine (
169), tramadol (
170), inositol (
171),
d-amphetamine (
172), and caffeine (
173,
174) are agents notable in having shown some amount of efficacy over placebo or active control in RCTs. Duloxetine has not been studied extensively but was found to reduce OCD symptoms in a case series of four patients whose condition had failed treatment with serotonin reuptake inhibitors (
175). Bupropion also has not been studied extensively in OCD; however, an open-label trial did not find this medication to be effective (
176).
Also in This Issue
As mentioned earlier, OCD and related disorders have been given a separate chapter in DSM-5. One of the goals of this issue of Focus is to compare and contrast these disorders in order to assist clinicians with accurate diagnosis and treatment. Drs. Steketee and Bratiotis discuss hoarding, Dr. Phillips discusses body dysmorphic disorder, and Drs. Grant and Chamberlain discuss skin picking and trichotillomania.
The genetic effects underlying mental disorders have received increasing focus. In this issue, Drs. Sobell, Pato, Pato, and Knowles discuss intriguing findings from genetic studies of OCD.
Psychotherapy remains an important component of OCD treatment. This topic is given attention in this issue with a review of CBT as an effective singular treatment or in combination with pharmacotherapy. Psychoeducation is an important component of the psychotherapeutic process. Educational resources for patients and families are provided in the box at the end of this article.