Augmentation strategies in depression treatment are being increasingly explored, with a growing recognition that for many people with a depressive disorder, full remission is either short-lived or absent (
1). Even in cases of beneficial response, subsyndromal symptoms may still persist (
2). Augmentation and combination approaches are often applied in clinical practice to provide an enhanced mood-elevating effect (especially in cases of perceived treatment resistance [
3]), and this prescriptive approach may involve multiple agents with antidepressant activity (
4). The combining of two or more established antidepressants may target different neurochemical pathways, while augmentation approaches may involve agents that work synergistically with the antidepressant (
5). More novel approaches may target nonneurotransmitter pathways to provide adjuvant benefits that may ultimately improve mood (e.g., reduction of inflammation [
6]). Augmentation strategies can be initiated either at the start of treatment or later, if there is insufficient response to monotherapy. The coadministration of standardized pharmaceutical-grade nutrients, referred to as nutraceuticals, may provide an effective and safe approach to enhancing antidepressant effects, either by synergistically augmenting a particular activity of an antidepressant medication (e.g., enhancing reuptake inhibition of monoamines) or by providing a range of additional biological effects (
7).
While the pathophysiology of depression is complex (and still being unraveled), several key neurobiological mechanisms underpinning the disorder have been considered germane (monoamine impairment, neuroendocrinological changes, reduced neurogenesis, reduction-oxidation reaction [redox] and bioenergetics abnormalities, and cytokine alterations consistent with chronic inflammation) (
8,
9). Several nutrients are known to have critical involvement in brain function, and some, such as omega-3, zinc, and folate, have been shown to affect an array of neurobiological processes that may be implicated in depression (
10). By targeting these key neurobiological pathways through specific nutraceuticals, such adjunctive treatments have the potential to augment the response to antidepressants.
While the potential of antidepressant augmentation with nutraceuticals is compelling, only recently have enough clinical studies become available to permit a clearer determination of their effectiveness as augmentation agents. To our knowledge, to date there have been no comprehensive systematic reviews of this area or, where sufficient data exist, any specific meta-analysis of these adjunctive studies. Our intention is to provide a comprehensive and critical review of the literature, focusing specifically on the current evidence for adjunctive use of nutraceuticals with antidepressants for clinical depression, and to discuss their potential evidence-based application in clinical practice.
Method
Search Strategy
PubMed, CINAHL (Cumulative Index of Nursing and Allied Health Literature), Web of Science, and Cochrane Library databases were searched up to December 2015. We looked for human clinical trials by using the search terms “Depression,” “Major Depressive Disorder,” “Major Depression,” “Mood,” “Antidepressant,” and “SSRI” in combination with the search terms “Adjunct,” “Adjunctive,” “Adjuvant,” “Augmentation,” and “Add-on” in combination with a range of nutraceutical search terms and 14 individual nutrients known to be important for neurological function, e.g., omega-3, folic acid, amino acids, vitamins, and minerals. Clinical trial registers were searched for relevant studies to cross-reference with the literature review and to locate unpublished data. A forward search of the identified articles was subsequently performed by using a Web of Science cited reference search, in addition to hand-searching the literature and reference lists, contacting authors and academic personnel for studies in the area, and searching the Internet for “gray” literature (data, published or unpublished, that is not readily accessible through the main databases).
Study Inclusion Criteria
We reviewed studies that reported uncontrolled, controlled, or quasi-experimental human studies that used any adjunctive (i.e., combined with pharmacotherapy) nutrient-based intervention for either diagnosed major depressive disorder (primary diagnosis or comorbid with another condition, e.g., diabetes, cardiovascular disease, cancer) or ongoing depression (defined as current use of antidepressant medication and a moderate or above-threshold level of depressive symptoms according to a validated scale, e.g., a score above 17 on the Hamilton Depression Rating Scale [HAM-D]). Further, the depression had to be either clinician-diagnosed or a primary health issue (i.e., not depressive symptoms studied as a secondary outcome for any other primary medical condition). For a study to be considered an “adjunctive study,” more than 95% of the study participants must have been taking antidepressant medication. Studies that were open-label without a control (e.g., an antidepressant-only group or single-blind dose variation design) must have recruited participants with “nonresponsive” or “treatment-resistant” depression (defined as no response to current or additionally previous antidepressant medication used for that depressive episode). Use of a recognized depression assessment scale was required for the primary depression outcome. The studies were required to have a duration of treatment of at least 21 days and a total sample size of >10 per arm. Case studies were not included. Only English-language articles since 1960 were included. No criteria were set for gender, age, or ethnicity of participants. All articles that did not meet these criteria were excluded. Studies were selected for final inclusion by means of consensus within the research group.
Study Tabulation
Studies were tabulated in four separate groups: one-carbon cycle nutraceuticals, omega-3, tryptophan, and other nutraceuticals. These were evaluated for dose, age, sample size, method, coprescribed antidepressant medication, diagnostic criteria, percentage of female participants, completion rate, and whether the study revealed a significant effect in favor of treatment or control condition (full data appear in the supplement accompanying the online version of this article). In the tables presenting results, “+” is used to indicate a statistically significant reduction in depression rating scores in the treatment group compared with the control group at study endpoint, and “n.s.“ is used to indicate no significant difference in depression rating scores between the treatment and control groups at study endpoint. For open-label studies, “+” is employed if the treatment significantly reduced depression symptoms on the depression rating scale over the course of the trial compared with baseline, and “n.s.“ is used if the treatment did not significantly reduce depression symptoms on the depression rating scale over the duration of the trial compared to baseline. This information is also summarized in text.
Statistical Analysis
A review of the studies was employed to determine whether multiple studies with acceptable homogeneity and adequate data were available to apply a meta-analysis. Homogeneity sufficient for meta-analysis was defined as the availability of more than two randomized controlled trials studying a homogeneous isolated nutraceutical compound at a therapeutic dose for 21 days or more for the adjunctive treatment of major depressive disorder. Such trials were available only for omega-3 and folic acid. A random-effects model was used, as the directional effect of omega-3 and folic acid in depression has not yet been established. The model analyzed the standard mean difference between treatment and placebo in the change between baseline and endpoint, combining the effect size (Hedges g) data. Data were analyzed by means of Comprehensive Meta-Analysis software, version 3 (Biostat, Englewood, N.J., 2015). The pooled effect size was determined by using a 95% confidence interval, while significance was determined by z tests (significance was defined as a p value of <0.05). Sensitivity analyses were conducted by comparing the results in a fixed-effects model and by removing studies with lesser homogeneity. A homogeneity test (Higgins I
2) and a visual funnel plot analysis were conducted to ascertain whether the effect sizes came from a homogeneous source (
11), and a regression analysis was used to assess whether any relationship between sample size and results occurred.
Results
An initial search revealed 5,287 articles in the area, from which 571 were indexed as clinical trials. From subsequent hand-searching of the abstracts, 60 potential studies were revealed as being in the specific area of the systematic review. Analysis of the full texts revealed 40 studies that met the inclusion criteria (see Figure S1 in the online data supplement). Nine studies involved folic acid, methylfolate, folinic acid, or a combination of folic acid and vitamins B6 and B12; eight involved tryptophan (or 5-HTP); four involved
S-adenosylmethionine (SAMe); eight involved omega-3 (a combination of eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA], EPA alone, or ethyl-EPA); two studies each were found on zinc, inositol, vitamin C, and vitamin D; and isolated studies were found for creatine, B12, and an amino acid combination. Common trial lengths were 4, 6, and 8 weeks (range 3–52 weeks), with a mean sample size of 63 participants (SD=75; range 20–475) and a mean age of 44 years (SD=11 years). The tables present results separately for one-carbon cycle nutraceuticals (
Table 1), omega-3 (
Table 2), tryptophan (
Table 3), and other nutraceuticals (
Table 4); the expanded tables in the online data supplement provide additional study features. Over two-thirds of the participants were female (69%). Of the 40 studies reviewed, 31 were randomized, double-blind, and placebo-controlled trials. Four studies had a 100% completion rate, with a mean overall completion rate of 85%.
Most studies used the DSM-IV criteria for a diagnosis of major depressive disorder, with the HAM-D being used in 29 studies (most of the others used the Beck Depression Inventory or the Montgomery-Åsberg Depression Rating Scale). A variety of antidepressant pharmacotherapies were used in the studies, which primarily used open inclusion of all SSRIs or commonly specified prescription of fluoxetine, citalopram, or escitalopram at adequate doses and durations. A positive effect of the adjunctive intervention was revealed in 68% of the clinical trials (including six out of eight omega-3 studies).
One-Carbon Cycle Nutraceuticals
Fifteen data sets in 14 studies were located concerning adjunctive use of nutrients involved in the one-carbon cycle: SAMe, folic acid (or related forms: folinic acid, methylfolate), B6, and B12 (
Table 1). Eight of these were double-blind randomized controlled trials, with seven studying open-label augmentation after nonresponse to antidepressant medication. Eight studies used DSM-IV criteria, two DSM-III, three ICD-10, and the study by Syed et al. (
25) made diagnoses according to depression level. Sample size ranged from 22 to 475, with the majority of studies having a primarily female sample (two folic acid studies had samples that were 85% [
17] and 100% [
19] female). Study lengths ranged from 6 to 52 weeks. Dosage variance was found among studies using oral SAMe (800 or 1600 mg/day) and methylfolate (15 or 30 mg/day). The HAM-D was used in all but four studies as the primary outcome measure. A range of antidepressants were used by participants, with fluoxetine being used solely in three studies. Ten out of the 15 trials revealed an effect in favor of this class of nutraceuticals, either over placebo or beyond baseline in nonresponsive depression.
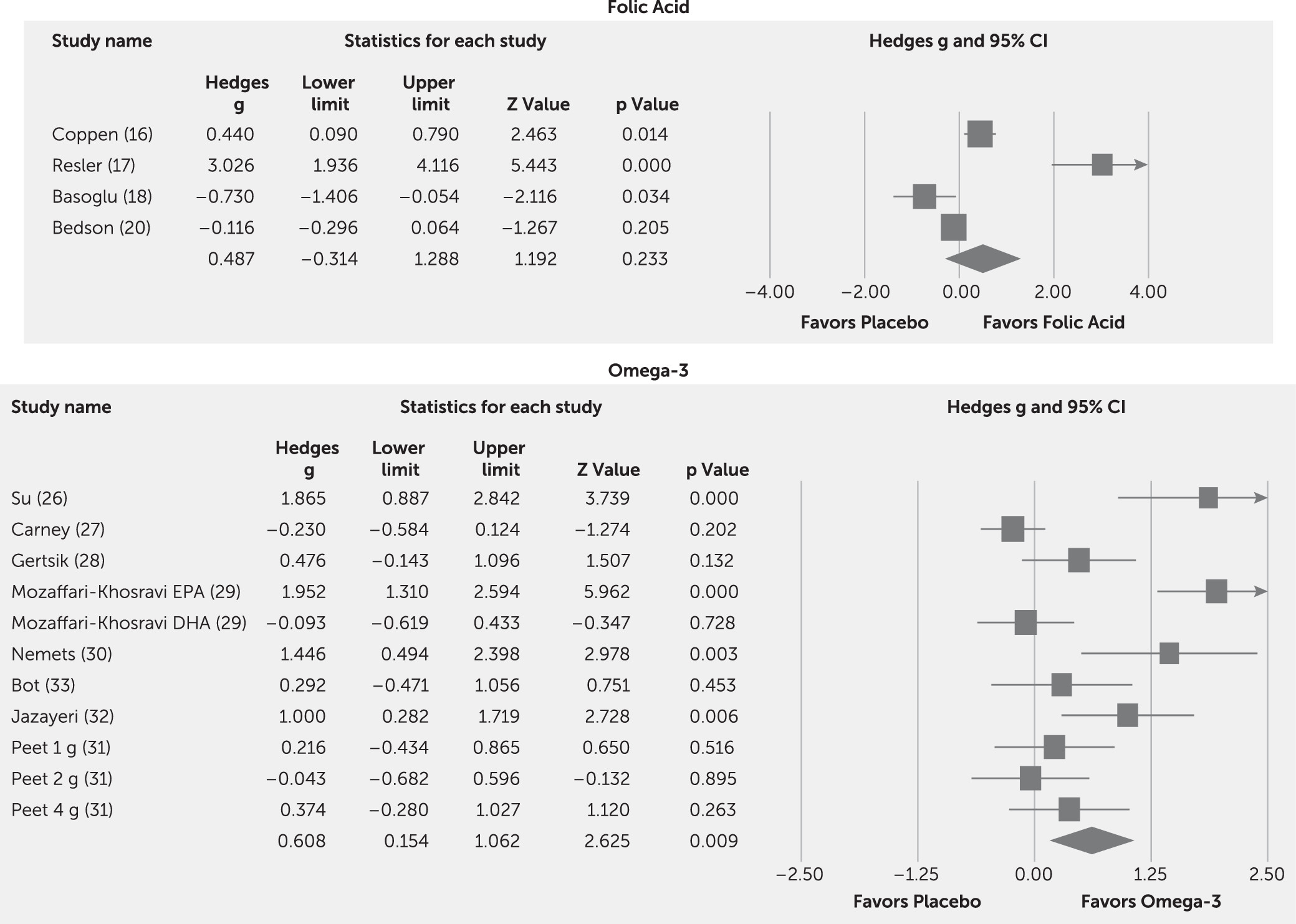
A sufficient number of folic acid studies were available to perform a meta-analysis. Four sets of data on folic acid (0.5 to 10 mg) were included in the meta-analysis. Two out of the four studies revealed a benefit in favor of folic acid; however, the largest study (Bedson et al. [
20]), with a robust sample of 475 subjects, revealed no significant difference from placebo. The pooled data in a random-effects meta-analytic model revealed a nonsignificant difference between folic acid and placebo (p=0.23; z=1.19, 95% confidence interval [CI], –0.31 to 1.29), with an inconsequential effect size (g) of 0.49 (
Figure 1). Sensitivity analyses revealed that when the disproportionately large study (
20) (N=475) was removed, the nonsignificant effect was maintained (p=0.29). When a fixed-effects model was adopted in place of a random-effects model, the significance of the results was also not altered (p=0.78). A Higgins test revealed substantial heterogeneity among folic acid depression studies (I
2=93%, p<0.001), with the funnel plot showing one marked outlier study (
17) (figure not shown); this reflects potential study bias. A regression analysis showed no relationship between sample size and the level of effect size (figure not shown). While heterogeneity may be produced when folic acid and methylfolate studies are combined, when the only methylfolate randomized controlled trial with available baseline and end-point data (Papakostas et al. [
24] trial 1/phase 1: 7.5 mg; trial 2/phase 1: 15 mg) was added to the meta-analysis, a similar nonsignificant effect was revealed (p=0.25; z=1.15, 95% CI, –0.22 to 0.83).
Omega-3
We located eight studies that met the inclusion criteria. All studies were double-blind randomized controlled trials. The trials involved EPA and DHA combinations (N=3), ethyl-EPA (N=4), and EPA versus DHA (N=1) (
Table 2). The range of EPA varied between 930 mg and 4.4 g (commonly 1 to 2 g per day, which is a therapeutic dose). The sample sizes of the study arms were generally modest (full sample size range, 20–122), and all but one study (
27) had a majority of female participants. Study lengths ranged from 4 to 12 weeks, with a variety of antidepressants used by the participants. All studies diagnosed the depression by means of DSM-IV criteria, except the study by Peet et al. (
31), who studied physician-diagnosed depression treated with antidepressants.
Eleven sets of data were included in the meta-analysis (including the four-arm Peet et al. study [
31] and the three-arm Jazayeri et al. study [
32]). Seven out of the 11 data sets revealed a benefit in favor of omega-3, but only six were statistically significant. The pooled data in a random-effects meta-analytic model revealed an effect size (Hedges g) of 0.61 (z=2.63, 95% CI, 0.15 to 1.06), which was highly statistically significant (p=0.009;
Figure 1). Sensitivity analyses revealed that when meta-analysis of the data was restricted to EPA-inclusive studies (removing the DHA-only arm of the Mozaffari-Khosravi et al. study [
29]), this effect was slightly strengthened (g=0.69, p=0.007). When a fixed-effects model was adopted in place of a random-effects model, the significance of the results was p<0.001. Aside from the methodological limitations of the generally small samples and the samples defined by diabetes and coronary heart disease in the studies by Bot et al. (
33) and Carney et al. (
27), respectively, most of the other study elements were reasonably consistent. A Higgins test, however, revealed substantial data heterogeneity among the omega-3 depression studies (I
2=82%, p<0.001), with the funnel plot showing three outlier studies (figure not shown); this reflects potential study bias. A regression analysis showed no relationship between sample size and the level of effect size (data not shown).
Tryptophan
Eight studies investigating the various forms of tryptophan (including one 5-HTP study) were reviewed (
Table 3). Many of the earlier studies (six studies before 1990) used
dl-tryptophan, which is potentially less effective than
l-tryptophan, as the D isomer is inactive. One study used
l-5-HTP, the active precursor of serotonin and a derivative of tryptophan, in conjunction with a tricyclic antidepressant. The majority of studies (N=7) were published before 1985 and used the diagnosis of “endogenous depression” (N=4) or “affective disorder” (N=2). The HAM-D was used by most studies to asses depression symptoms (N=5), and two studies used the Cronholm-Ottosson Depression Scale. Because most of the studies reviewed were conducted between 1969 and 1983, predominately tricyclic antidepressants (N=4) and monoamine oxidase inhibitors (N=2) were prescribed in conjunction with tryptophan (or 5-HTP). Four out of the seven tryptophan studies and the one L-5-HTP study found a positive effect of the adjunctive treatment, relative to placebo and/or a control condition. We considered undertaking a meta-analysis of tryptophan but were unable to perform one because of missing raw data in many of the early studies.
Other Nutraceuticals
Ten other studies involving a range of nutraceuticals were located, but there were too few on specific nutraceuticals for us to perform a meta-analysis (
Table 4). Two studies each tested zinc, vitamin C, vitamin D, and inositol; one study used a mixture of amino acids, and one tested creatine. All studies except one (
47) were double-blind randomized controlled trials ranging from 4 to 26 weeks. All studies used DSM-IV to establish the depression diagnosis, and all but two studies used the HAM-D for assessment. A range of antidepressants were coprescribed, with the most common being fluoxetine (N=3). In all but one study (
44), the majority of participants were female. The individual study findings demonstrated positive and significant results for vitamin D (a separate negative community-based, nonclinical trial notwithstanding [
52]), creatine, and an amino acid combination; mixed results for zinc and vitamin C; and no significant benefit over placebo for inositol.
Safety
All the nutraceuticals were generally well tolerated; gastrointestinal symptoms (e.g., constipation, stomach upset, and diarrhea) were the most commonly reported adverse events across all nutraceutical groups (omega-3, one-carbon cycle, and tryptophan). Across all studies, the rates of dropouts due to side effects were very low (less than 2% of the samples), further supporting tolerability.
Despite the mild nature of the adverse effects reported in the included studies, nutraceuticals are not without risk or serious safety concerns when used at high doses, over long periods of time, and/or when combined with certain medications. Potential carcinogenicity should be considered regarding supplements containing folic acid, as higher folate blood levels are linked to increased risk of prostate cancer (
53,
54). While meta-analyses have not revealed definitive evidence for the association between folic acid supplementation and a range of cancers (
55), and adequate folate consumption from vegetables and whole grains has potential cancer-protective properties, high dosages of folic acid may not be advised in people with cancer, since it increases cell proliferation (
56). Folic acid has also been implicated in accelerating cognitive decline with age and reducing the efficacy of particular antifolate drugs, such as immunosuppressants (
57).
Omega-3 also should be prescribed with caution in people with prostate cancer, since a meta-analysis showed that certain fatty acids may have an association with prostate cancer risk (
58). It should be noted that this association was weak and further larger epidemiological studies are required to assess this comprehensively. Higher-dose omega-3 supplementation has also been suspected to increase bleeding, impair immune function, increase lipid peroxidation, and impair lipid and glucose metabolism (
59). There is also evidence that omega-3 likely increases LDL cholesterol concentrations, but only when dosages of DHA and combined EPA/DHA are over 2 g/day (
59).
SAMe has been associated with an increased risk of hypomania or manic switching in depressed patients. However, the switching has primarily been reported in patients with a diagnosed bipolar disorder and with intravenous or intramuscular administrations of SAMe (
60,
61). The phenomenon has not been observed in clinical trials of oral administration of SAMe (
62). Tryptophan and 5-HTP, when used in conjunction with other serotonergic agents (such as antidepressants, opioid pain medications), may cause a toxic state, serotonin syndrome, due to an excess of serotonin in the brain (
63). Hypercalcemia and vascular calcification may occur when vitamin D is used at high doses (≥275 µg/day) (
64), while high doses of zinc (>25 mg/day) can lead to copper deficiency (
65). At doses above 1000 mg/day, vitamin C has been linked to an increased risk of kidney stones in men due to its conversion to oxalate and excretion in urine (
66). Caution is warranted when reviewing the safety data on nutraceuticals, and many of the suggested potential risks have not been revealed in randomized controlled trials or meta-analyses.
Discussion
The overall findings revealed a substantive number of human clinical trials testing adjunctive nutraceuticals to augment antidepressant activity in depression. Primarily positive results in replicated studies were found for SAMe, methylfolate, omega-3 (EPA or ethyl-EPA specifically), and vitamin D. Due to positive isolated studies, tentative consideration may also be extended to creatine and an amino acid combination. Further research is needed to clarify whether zinc, vitamin C, or tryptophan (or more specifically 5-HTP, the active precursor of serotonin) may be of value, while inositol is unlikely to have any utility as an adjunctive antidepressant agent. It should be noted, however, that previous findings suggest that inositol may have an antidepressant effect as a monotherapy agent rather than an adjunctive agent for depression (
67,
68).
The finding from the omega-3 meta-analysis demonstrates that this augmentation approach significantly reduces depressive symptoms beyond placebo and thus has potential clinical and public health significance. As detailed in a recent general meta-analysis, it is advised that EPA or ethyl-EPA dominant formulas be used, as DHA may not be effective (
69). In summation, EPA-rich omega-3 fish oil may be recommended for the adjunctive treatment of major depressive disorder. In respect to folic acid and methylfolate, results are less clear. As the meta-analysis revealed, folic acid cannot be firmly recommended; however, the “active” forms of methylfolate and folinic acid can be tentatively recommended. It should be noted that while the review included various formulations (folic acid, folinic acid, methylfolate), the latter is a patented derivative that has been the subject of several large-scale commercially sponsored clinical trials. There is a potential concern that commercially sponsored trials may be biased toward positive results. For example, a review by Perlis et al. (
70) found that industry-funded randomized controlled trials with a reported conflict of interest were 4.9 times more likely to report positive results. Regardless, the vast majority of efficacy-focused biological medicine studies have commercial sponsorship, and while there is the potential for inherent bias, the methodology of these studies was rigorous.
All of the nutraceuticals reviewed in this article have mechanistic antidepressant activity underpinning their use. The one-carbon cycle agents (SAMe, folic acid/methylfolate, B6/B12) are critical in the methylation processes of monoamines (
71). In particular, SAMe may improve depressed mood through enhanced methylation of catecholamines and increased serotonin turnover, reuptake inhibition of norepinephrine, enhanced dopaminergic activity, decreased prolactin secretion, and increased phosphatidylcholine conversion (
72). Omega-3 (in particular, EPA) exerts antidepressant activity potentially through modulation of norepinephrine, dopamine, and serotonin reuptake, degradation, synthesis, and receptor binding; through enhancement of glutathione antioxidant capacity (
73); and through enhancement of cell membrane fluidity (
74).
Another possible explanation for the antidepressant efficacy of these compounds may reside with their anti-inflammatory properties, which are well demonstrated with SAMe (
75) and EPA (
76,
77). A recent double-blind monotherapy randomized controlled trial (N=155) showed that patients with major depressive disorder who have biomarkers of increased inflammation (e.g., interleukins or C-reactive protein) may benefit from EPA over both placebo and DHA, compared with those with low levels of inflammation biomarkers (
78). Zinc is one of the most prevalent trace elements in the amygdala, hippocampus, and neocortex, and aside from having anti-inflammatory and immunological-modulating properties, it is involved with hippocampal neurogenesis through up-regulation of brain-derived neurotrophic factor (BDNF), while also modifying
N-methyl-
d-aspartate (NMDA) and glutamate activity (
79,
80).
Amino acids are essential precursors of all proteins involved in the manufacture of neurochemicals. In particular, tryptophan (and particularly its derivative 5-HTP) is an essential monoamine precursor required for the synthesis of serotonin (
81). Creatine plays a pivotal role in brain energy homeostasis, and altered cerebral energy metabolism at a cellular level may be involved in the pathophysiology of depression (
51). Oral creatine supplementation may modify brain high-energy phosphate metabolism in people with depression. Inositol is incorporated into neuronal cell membranes as inositol phospholipids, and it is the key metabolic precursor in the phosphoinositide (PI) intracellular secondary messenger cycle (
82). The PI cycle is involved with a broad range of neurotransmitter systems, including adrenergic, serotonergic, dopaminergic, glutaminergic, and cholinergic receptor types (
83). The potential exists that both inositol and SSRIs converge on the same mechanism of action, as 5-HT
2 receptors are linked to the PI cycle signal transduction pathway (
84). Regardless of this preclinical activity, as reviewed above, this effect was not manifested in adjunctive treatment studies. However, as discussed above, inositol may have a greater therapeutic effect as a monotherapy agent for depression (
67,
68) or for panic disorder (
85).
Vitamin D can be considered a neurosteroid, with vitamin D receptors being identified in areas involved with depression, such as the prefrontal cortex, hypothalamus, and substantia nigra (
86). Vitamin D has been revealed to increase the expression of genes encoding for tyrosine hydroxylase (precursor of dopamine and norepinephrine) (
86). Further, a major dopamine metabolite in the striatum and accumbens has been found in methamphetamine-treated animals administered vitamin D (
87). Vitamin C is an essential vitamin involved in various neuroendocrine activities and is needed for the production of neurotransmitters, such as serotonin (
88). An animal study showed that the coadministration of vitamin C (1 mg/kg p.o.) potentiated the action of subeffective doses of fluoxetine (1 mg/kg), thus providing a synergistic antidepressant-like effect with an SSRI (
89).
The methodology of this review has several limitations, and general cautions regarding the findings need to be considered. First, our search criteria were modestly restrictive, and several excluded studies (i.e., case studies and trials with non-English-speaking patients or those with general depressive symptoms) were not included, and thus a more expansive perspective might have been reached with their inclusion. Because much of the early literature on SAMe is in Italian, it is not covered by this review. Readers are advised to additionally consult the Italian literature on this nutraceutical. Caution also needs to be extended to the findings of some of the nutraceuticals (aside from omega-3, SAMe, and folic acid/methylfolate) due to a limited number of studies and the small sample sizes of the studies reviewed. Potential publication bias was also revealed in the folic acid and omega-3 meta-analyses (from funnel plot analysis), as well as heterogeneity among studies (in respect to I2 analysis and marked differences in medications used, study lengths, nutraceutical dosages, and participant characteristics). Several studies of treatment-resistant depression were also open label, and while any effect beyond baseline is of merit, the lack of placebo cautions interpretation of the results. Lastly, the older studies did not provide comprehensive details of the methodology or the raw statistics, and thus a more thorough assessment could not be achieved. Caveats regarding the prescription of the nutraceuticals relate to the quality of nutrient products (especially with SAMe, though current formulations have potentially more stable shelf-lives) and the correct formulation and dosage (especially with omega-3). Expense may also be an issue in the case of SAMe and methylfolate.
Nutraceutical applications in psychiatry are advancing, as reflected in recent international collaborative consensus and position statements discussing the potential of nutraceutical use in psychiatry (
10,
90) As noted, much more work is needed, and while an evolving body of research is strengthening the potential of nutraceuticals (and dietary considerations) as an important element in modern psychiatric practice, we are only beginning to study their potential applications. A major barrier to this field is the often unpatentable nature of these compounds, and large-scale randomized controlled trials may be unfeasible due to a potential lack of financial incentive. Despite the challenges of soliciting non-industry-sponsored funding, randomized controlled trials with robust sample sizes and the application of pharmacogenomic and neuroimaging technologies to determine biomarkers of response are now required. Finally, while the current studies (whether as first-line therapy or in treatment-resistant depression) were pooled in the present article, as the database of this research expands, future subanalyses potentially can be conducted assessing these individual nutraceuticals as first-line agents.
Another area of potential interest is the use of combination nutraceuticals. Our research group is currently testing an adjunctive nutraceutical formulation in the treatment of major depressive disorder not responsive to stable antidepressant medication (
7). Nutrients commonly work in concert, and as detailed above, a range of nutraceuticals modulate several key pathways involved with the pathogenesis of depression. The formulation currently being tested (involving SAMe, ethyl-EPA, zinc, folinic acid, and 5-HTP and relevant cofactors) may provide an array of antidepressant action beyond that of isolated approaches. In conclusion, as detailed above, several nutraceuticals may hold a potential clinical application to enhance the antidepressant effect of medications. Further, the integration of nutraceuticals into clinical practice guidelines should be considered, especially in circumstances where the risk-benefit ratio may not justify the use of pharmacological treatment (such as in mild symptom presentations and in the treatment of children, adolescents, and pregnant women [if the nutraceuticals are established as safe]). While future research needs to determine how this is applied to the individual (and whether it is more pertinent in cases of nutrient deficiencies), many nutraceuticals are low-cost options that are worthy of clinical consideration.