Schizophrenia spectrum disorders (SSDs) are associated with an elevated risk of committing violent acts, especially assaults, or for being convicted for such acts.
1–9 For example, in a 26-year prospective study of a Finnish birth cohort including 12,058 subjects, persons with schizophrenia exhibited 7.0 times the community rate of commission of violent crime.
3 In a 44-year retrospective study of a Danish birth cohort of 358,180 persons, the diagnosis of schizophrenia was associated with 4.6 times the rate of arrest for violence among men, and 23.2 times the rate among women.
5 Some of this excess risk of aggression has been related to premorbid conduct disorder,
10,11 positive symptoms, especially paranoia,
12,13 or concomitant antisocial or psychopathic traits
14–17 with or without concomitant substance abuse.
2,7,18–23 Moderating factors aside, evidence from 1) studies of violence among psychiatric patients, 2) studies of the prevalence of SSDs among violent persons, or 3) studies of birth or population cohorts all support the conclusion that SSDs are a significant risk factor for interpersonal violence.
This finding is associated with multiple problematic consequences. Violence threatens the lives and well-being both of patients and of others in their immediate social surroundings.
24 Violent behavior is associated with noncompliance and complicates treatment.
6,25 Violence disrupts families that might offer a vital stabilizing force for the patients.
26 Violence increases the need for institutionalization, with its attendant costs and restriction of self-determination.
9 Violence by persons with SSDs contributes to the stigma that biases laypersons against not only all persons with schizophrenia but against all those with mental illness.
25,27,28 In so far as SSDs occur in roughly 1% of most populations, that subset of persons will contribute to society’s net burden of violence. Although the attributable risk is small—estimated to be on the order of 5% of total societal violence
6,29,30—SSD-associated violence has been estimated to account for 6%−28% of homicides
9 and sometimes causes even more catastrophic and widely publicized consequences, such as serial killings and mass murders. Some evidence suggests that treatment can reduce the risk of SSD-related violence.
31 Patients, their families, and the community would benefit from the identification of effective treatments to reduce persistent or recurrent hostility and the risk of overt aggression.
But what treatment? Evidence suggests that aggressive persons with schizophrenia, once identified, tend to be treated with long-term high-dose neuroleptics, “despite a lack of clear evidence that such treatment is effective” (
32 p 640).
Four reviews of the available scientific literature have addressed this question. Brieden et al.
33 conducted a review of articles discussing the pharmacological treatment of aggression among persons with SSDs published between 1980 and 2000. Based on a MEDLINE search, they identified “about ten articles” that directly addressed this issue. They consequently expanded their search to address treatment of aggression in all psychiatric disorders, and to include open label studies, cases series, and case reports. They included reports regarding emergency management, chronic treatment, inpatients, and outpatients, employing a variety of measures of hostility or aggression. While the authors acknowledge the importance of this early effort, the published data leaves important questions unresolved. They commented that there is “wide agreement” that clozapine is efficacious for the management of aggression and hostility in persons with schizophrenia, but did not cite a randomized controlled trial (RCT) supporting that statement. They cited two RCTs
34,35 that reported that risperidone was more efficacious than other antipsychotics. The first study failed to report the proportion of subjects who completed or the relative efficacy of different doses. Fewer than one-half of subjects completed the second study. The authors cited one RCT reporting that adjunctive carbamazepine was effective in persistently aggressive patients with schizophrenia,
36 but that study disappointingly did not report the impact of treatment on hostility or aggression. They also cited one RCT reporting the efficacy of citalopram.
37 They did not state whether the results of the cited studies might have been confounded by concomitant administration of other psychotropics, classify the quality of the cited studies, or examine the level of evidence supporting a recommendation. These authors concluded that atypical antipsychotics “with a preference for clozapine” should be used to manage repetitive aggression in patients with schizophrenia, but qualified their review: “There is an urgent need to refine the treatment of aggression on the basis of specific studies to be done in the future.”
A similar review was authored by Fazel and Topiwala.
38 These authors state that they searched MEDLINE, EMBASE, and PsycInfo from 2000 to March of 2010, using the search terms schizophren*, psychos* AND violen*, aggress* AND antipsychotic*, neuroleptic*, mood stabilizer*, medication*, “as well as specific drug names.” They did not provide the drug names or limit the review to articles reporting management of persons diagnosed with schizophrenia spectrum disorders. They state, “Publications were
largely selected from the past 5 years,” [emphasis added] although it is not clear on what basis older publications were excluded. They also searched the reference lists of the articles found in their automated search. These authors identified a total of 18 relevant studies. They concluded 1) “There is randomized controlled trial evidence in support of a specific anti-aggressive effect of clozapine,” 2) “Insufficient high-quality evidence has been published to recommend the use of atypical rather than typical antipsychotics in the management of violence in schizophrenia,” 3) “The evidence to support the efficacy of adjunctive mood stabilizers is inconsistent,” 4) “There is little evidence for the effectiveness of β-blockers in the management of aggressive patients, and these may be poorly tolerated,” and 5) Tricyclic antidepressants (desimpramine and imipramine) and anticraving agents (naltrexone) “may be of benefit in dual diagnosis patients.” These authors did not review trials of desimpramine, imipramine, or naltrexone for the management of aggression in persons with schizophrenia. Although the empirical basis for some of their conclusions and recommendations is underspecified, several of Fazel and Topiwala’s conclusions bear consideration: 1) that the currently available literature is both limited and scientifically weak, 2) that the phenomenology under scrutiny is heterogeneous, and 3) that “As pathways to violence become better elucidated, we anticipate that pharmacological therapy will target specific symptom profiles…”
A third review authored by Buckley et al.
39 does not report a search method. The majority of papers discussed in this review were reports of medication trials to manage emergency room agitation in populations whose diagnoses varied from unknown to 100% schizophrenia. This review identified one single report of a medication trial for the management of persistent aggression.
40 Rather than offering practice recommendations based on their review, these authors deferred to the expert consensus guidelines of Allen et al.
41 with respect to management of emergency agitation, and to the Schizophrenia Patient Outcomes Research Team (PORT) psychopharmacological treatment recommendations
42 with regard to management of persistent aggression.
The previously cited PORT study represents the fourth available review of this topic. The authors conducted a MEDLINE search from January 2002 through March of 2008, using the search terms “schizophrenia” and the names of individual drugs, limiting the search to clinical trials published in English. The authors identified five reports of the efficacy of clozapine for the management of aggression in schizophrenia
40,43–46 and six reports regarding the efficacy of other agents for this purpose.
47–52 Based on this review the PORT authors recommended, “A trial of clozapine should be offered to people with schizophrenia who present with persistent symptoms of hostility and/or display persistent violent behaviors” (
42 p. 80).
We undertook a more comprehensive systematic review of the English language literature, attempting to identify every peer-reviewed study reporting a test of the hypothesis that a medication reduced either hostility or overt interpersonal aggression among persons with SSDs. We classified every such report, and considered whether the level of evidence, in toto, supports a recommendation or a guideline for clinical management of this important behavioral complication of SSDs.
Methods
We employed four search strategies in an attempt to identify potentially relevant publications.
Search 1 was conducted in Ovid/Medline on August 10, 2009 using the following algorithm: [exp Schizophrenia/ OR schizophrenia.mp.] AND [[aggression.mp. OR exp Aggression/] OR [exp Violence/ OR violence.mp.] OR violent OR [hostility.mp. OR exp Hostility/]] AND [[exp Drug Therapy/ OR drug therapy.mp.] OR pharmacotherapy.mp. OR [clinical trial.mp. OR exp Clinical Trial/]]. This strategy yielded 314 citations.
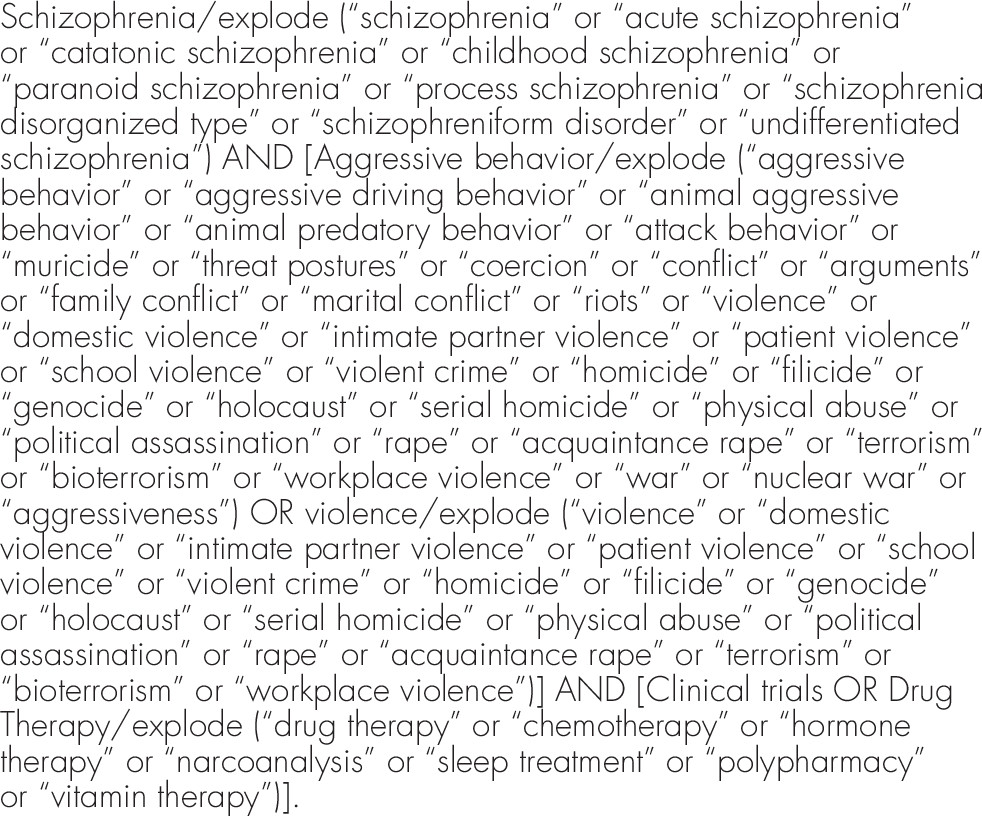
Search 2 was conducted in PsycINFO August 10, 2009 using an algorithm devised by a Ph.D. in Library Science (
Figure 1). This strategy yielded 115 citations.
Search 3 was conducted in Ovid/Medline on April 10, 2010 employing the Cochrane “Highly Sensitive Search Strategy for identifying randomized trials in MEDLINE: sensitivity-maximizing version (2008 revision); Ovid format” (
53 p. 138) (see
Figure 2). This strategy identified 417 citations.
Search 4 was conducted in EMBASE on September 15, 2010 employing the Cochrane method (
53 p. 121–122): Free text terms: random$ ($ means truncation symbol), factorial$, crossover$, Cross over$, Cross-over$, placebo$, doubl$adj blind$, singl$ adj blind$. assign$, allocat$, volunteer$. Index terms (aka EMTREE terms): crossover-procedure, double-blind procedure, randomized controlled trial, single-blind procedure, and Other terms: schizophrenia, aggression, hostility. This strategy identified 324 citations.
Searches 1–4 were de-duplicated, yielding 804 unique citations. Searches 1–3 were repeated October 4, 2010. Four new abstracts were identified. All abstracts were reviewed; 264 of the 804 abstracts suggested that the corresponding full text articles possibly reported data regarding the efficacy of neuropharmacological agents for the management of either hostility, aggression, or violence in persons with SSDs. These 264 full text articles were obtained and reviewed. An additional 76 abstracts were obtained for all references in these 264 papers that appeared to represent empirical reports not otherwise captured by our search. Based on a review of those 76 abstracts, an additional 18 full text papers were obtained. One author (J.V.) reviewed the resulting total of 282 full text papers, identifying 179 articles that contained either data or statements regarding the efficacy of pharmacological agents for the management of hostility, aggression, or violence. Searches 1–3 were repeated June 16, 2012. After de-duplication, review of abstracts, review of full texts, and review of papers identified in the reference sections of the newly found papers, seven additional publications were identified that reported relevant data.
The preliminary review of these 186 full text articles revealed the considerable, and problematic, diversity of research designs. In addition to the typical variation in medication trial design such as subject number, age, gender, severity of illness, medical exclusion factors, agent, dose, duration, blindness, allocation method, assessment measures, statistical method, proportion of completers, and intent to treat analysis, there were also differences in 1) diagnosis—e.g., studies confined to schizophrenia versus those that included mixed populations with schizophrenia spectrum disorders versus those that included “psychotic disorders” as well as mood disorders, 2) dependent variable—e.g., studies that regarded efficacy for the management of hostility or aggression as a primary outcome measure versus those (the overwhelming majority) that reported subscale measures of hostility as a secondary, often incidental, result, 3) clinical site—e.g., studies with inpatients (which often employed various selection criteria either for a history of responsiveness to antipsychotics or for treatment resistance) versus studies with outpatients, 4) adjunctive treatment—e.g., studies that investigated single medications (usually antipsychotics) for dual effects on thought disorder and behavior versus studies of adjunctive medications for behavior management, 5) aggressivity—e.g., studies that preselected aggressive subjects versus those (the majority) that did not. A few studies also conducted multivariate analyses to control for akathisia. Almost all of the controlled or comparison studies permitted concomitant administration of other psychotropic agents, yet no studies controlled for this potentially confounding factor.
It is unclear how meaningful it would be to collapse the results from such different study designs in an effort to identify conclusions that would be generalizable to the broad spectrum of persons with schizophrenia and their many variations of clinical circumstances. Given this diversity of research designs, therefore, we organized the review to address four questions:
1.
Does evidence exist that any medication will reduce overt aggression in representative patients with SSDs that have not been preselected for exhibiting excessive aggression?
Corollary: Does evidence exist that one medication is more efficacious than another in reducing overt aggression in representative patients with schizophrenia spectrum disorders?
2.
Does evidence exist that any medication will reduce hostility in representative patients with schizophrenia spectrum disorders?
Corollary: Does evidence exist that one medication is more efficacious than another in reducing hostility in representative patients with schizophrenia spectrum disorders?
3.
Does evidence exist that any adjunctive medication will reduce overt aggression or hostility in persons with schizophrenia spectrum disorders?
4.
Does evidence exist that any medication will reduce overt aggression or hostility in persons with schizophrenia spectrum disorders preselected for clinically problematic aggression?
The 186 full text articles were classified according to which of these questions their data addressed. In several studies
52,54,55 agent 1 was compared with agent 2—which was regarded as an
active control for the purposes of assuring assay sensitivity—as well as with placebo. In such studies, despite the generation of potentially relevant data, the investigator’s stated intent was not to test the hypothesis that the active control agent 2 was efficacious of the treatment of schizophrenia, and the statistical analyses sometimes exclude results with respect to agent 2. For example:
The olanzapine group was included in the study in order to provide a concurrent active control group to confirm that the study as executed was adequate to detect a drug effect in the event of negative findings for paliperidone ER compared with placebo (i.e., assay sensitivity to detect a “failed trial”). The study was not designed to support statistical comparison of the paliperidone ER and olanzapine arms
52 (p. 150).
This reporting strategy with respect to the active control arm is traditionally acceptable on the grounds that the efficacy of that control agent to treat schizophrenia has been reliably and repeatedly demonstrated.
56 However, because the active control agent has typically
not been demonstrated to be efficacious for the management of hostility or aggression in SSDs, and because the statistical analysis of efficacy of the active control agent versus placebo is reported in several of these papers, we judged that readers may profit by examining published data reporting changes in hostility/aggression measures associated with such active control treatments and we include the reported results in this review. A few studies (e.g.
57) classified their subjects as being “violent” versus “non-violent.” The data were, therefore, judged relevant to more than one of our four questions, and their results are reported in more than one of our tables.
Using a standardized checklist, two investigators independently reviewed each article to extract data including the research design, clinical setting, number of subjects, proportion of completers, agents and doses compared, duration, outcome measure employed, concomitant psychotropics permitted, statistical method, and reported results. The investigators then compared the data they extracted and reconciled any differences—either in reportable data or in judgment regarding level of evidence—by consensus. The pair of investigators that reviewed each paper discussed and reached a consensus in regard to the applicable classification according to the American Academy of Neurology’s recommendations for Levels of Evidence.
58–60 Note: in these practice guidelines for classification of therapeutic articles, criterion “e” requires that studies of equivalence comparing two agents include a “standard treatment.” Because no standard treatment has been established for aggression in schizophrenia, it is not possible for any RCT comparing of two drugs, lacking placebo control, to be Class I. Studies comparing the efficacy of two agents without a placebo control were, therefore, rated as Class II if they met all other Class I criteria, or as Class III or IV, depending on how many other criteria (e.g., percent completers) were fulfilled. Guidelines for the classification of clinical benefit propose that Class C (possibly effective) requires at least one Class II or two consistent Class III studies. When agents were proven effective by one Class II as well as by one consistent Class III study, we also classified the evidence of clinical efficacy as Class C. Class IV studies did not impact classification of efficacy but were included to make the universe of data available.
Results
One hundred eighty-six peer-reviewed articles were identified that reported clinical effects of pharmacological agents on aggression or hostility in persons with SSDs, either as a primary outcome variable, a secondary outcome variable, the focus of post hoc analysis, or an incidental finding derivable from tabulated results. Of these, a consensus was reached that 92 articles provided sufficient methodological information (e.g., number of subjects, diagnosis, interventions, outcome measures, percent completers, statistical analysis) to regard the data as reportable.
Multiple measures of aggression or hostility were employed in the reviewed reports. Studies that addressed overt aggression primarily employed the inpatient observational Overt Aggression Scale (OAS
61), or the Modified Overt Aggression Scale (MOAS
62). Studies that addressed hostility primarily employed either individual items from the Positive and Negative Symptoms Scale (PANSS
63) or the Brief Psychiatric Rating Scale (BPRS
64), or factors comprised of clusters of related items from one of these two instruments. Note that the BPRS item content is wholly contained within the PANNS. Thus, commonly employed and somewhat related measures include
1.
The BPRS hostility item,
642.
The BPRS hostility factor, aka hostility/suspiciousness factor, aka Factor V, derived from the hostility, suspiciousness, uncooperativeness items,
65,663.
The PANNS hostility item,
634.
The PANSS uncontrolled excitement/hostility factor, derived from PANSS excitement and hostility items, aka “Marder factor 4,”
355.
The PANSS hostility factor, aka “hostility cluster,” derived from hostility, excitement, poor impulse control, and uncooperativeness items,
67–696.
The Aggression Risk Profile (derived from PANSS responses according to the violence potential assessment criteria in appendix 4 of the PANSS manual).
63Other measures that are perhaps similar were reportedly employed, but neither described nor identified by citation, such as the PANSS “supplemental anger item,”
70 the PANSS “aggression supplemental scale,”
71 and the “aggressiveness risk” score (perhaps referring to the Aggression Risk Profile).
72The measures employed were sometimes reported ambiguously, in which case the scale that seemed to most likely have been used in a study was decided by consensus. Other identifiable measures employed included the Buss-Durkee Hostility Inventory,
73 the Plutchik Impulsivity scale,
74 the Nurses’ Observation Scale for Inpatient Evaluation Irritability Scale,
75,76 the Aggression and Social Dysfunction Scale,
77 the MacArthur Community Violence Interview,
78,79 the Barratt Impulsiveness Scale (BIS
80,81), the aggression severity measure of the Clinical Global Impression scale (CGI
65), the Personal and Social Functioning Scale, item 4: disturbing and aggressive behaviors,
82,83 the Wittenborn Psychiatric Rating Scale Aggression item (WPRS
84), the anger item on the State-Trait Personality Inventory,
85 seclusion and restraint data, or
ad hoc rudimentary measures such as occurrence or nonoccurrence of any known aggressive behavior during an arbitrarily selected time period (e.g.,
57,
86,
87) or a “rough evaluation” of aggressiveness.
88For the purposes of this report, “hostility” refers to 1) The BPRS hostility item (no. 10), 2) the BPRS Marder hostility factor, 3) the BPRS Hostility/Suspiciousness factor score (mean of hostility, suspiciousness, and uncooperativeness items, 4) the PANSS hostility item, or 5) the PANSS uncontrolled hostility/excitement factor derived from the excitement, hostility, and impulse control items. The principal results are displayed in
Tables 1–
5 (to view the legend for these tables, see the
data supplement accompanying the online version of this article) The narrative details the subset of studies pertinent to determining levels of evidence.
1. Does evidence exist that any medication will reduce overt aggression or physical violence in patients With schizophrenia spectrum disorders?79,89
No Class I, II, or III RCTs were identified that tested this hypothesis. One large scale Class IV 2-year observational study (Swanson, et al., 2004a
89) compared the anti-aggressive impact of any conventional antipsychotic versus any atypical antipsychotic versus no treatment in 403 community dwelling persons with schizophrenia spectrum illness. Aggression was assessed by self-report, using the MacArthur Community Violence Interview,
79 as well as chart reviews and arrest records. In a time series analysis, atypical antipsychotics were significantly more likely to reduce violence than typical agents (p <0.05). Adherence to atypical antipsychotics was also associated with reduced risk of violence. This effect appeared to be mediated by 1) decreased psychosis, 2) decreased substance abuse, and 3) decreased adverse medication effects. One conclusion was that medication noncompliance is an independent risk factor for community violence among persons with these disorders, even controlling for substance abuse.
We conclude that the data are insufficient to fulfill criteria for formal practice guidelines. Given current knowledge, the benefit of pharmacological intervention for the management of overt aggression in persons with SSDs who have not been preselected for aggression is unproven (Level U).
Corollary: Does evidence exist that one medication is more efficacious than another in reducing overt aggression or physical violence in patients with schizophrenia spectrum disorders? 45, 46, 57, 87, 89–102 (Table 1)
Eighteen articles were identified that reported relevant data. No Class I studies were identified that tested this hypothesis. Two Class III studies reported evidence that clozapine was superior to haloperidol in reducing OAS measures in inpatients with SSDs.
45,90 The first study permitted concomitant administration of benzodiazepines. The second permitted administration of lorazepam, diphenhydramine, and chloral hydrate. Neither study controlled for coadministration of these psychotropic medications. One Class III study reported that perphenazine was superior to quetiapine in reducing aggression assessed with the MacArthur Community Violence Interview.
46 One Class III study reported no difference in a comparison of chlorpromazine with thioridazine.
91We conclude that the clozapine is possibly superior to haloperidol for the management of overt aggression among inpatients with SSDs who have not been selected for aggression and who may be receiving other psychotropic medications (Level C). Given current knowledge, the comparative benefit of other pharmacological interventions is unproven (Level U).
2. Does evidence exist that any medication will reduce hostility in patients With schizophrenia spectrum disorders?34,48,49,51,52,54,55,103–113 ( Table 2)
Eighteen articles were identified that reported relevant data. No Class I studies were identified that tested this hypothesis. Four Class II studies
52,104,105,107 and one Class III study
55 reported that paliperidone ER treatment was associated with greater reduction in measures of hostility than placebo among inpatients with SSDs. All five studies permitted concomitant administration of other psychotropics including benzodiazepines, antidepressants, barbiturates, pyrazolopyrimidine sedative/hypnotics, and anticholinergic agents. None controlled for this factor. Two Class II studies
51,103 and one Class III study
108 reported tests of the efficacy of quetiapine versus placebo among inpatients. None of these controlled for concomitant psychotropics. One Class II study and the Class III study reported that quetiapine was associated with greater reduction in measures of hostility than placebo, but the second Class II study reported no difference at the endpoint. A single Class II study reported that olanzapine treatment was associated with significantly greater reduction in hostility than placebo.
106 That study did not control for concomitant administration of other psychotropics. We conclude that the paliperidone ER treatment is
probably effective for the reduction of hostility among inpatients with SSDs who have not been selected for aggression and who may be receiving other psychotropic medications (Level B). Quetiapine is
possibly effective for this indication. Given current knowledge, the benefit of other pharmacological interventions for the management of hostility is unproven (Level U).
Corollary: Does evidence exist that one medication is more efficacious than another in reducing hostility in patients with schizophrenia spectrum disorders? 44,47, 50, 108, 114–131 (Table 3)
Twenty-five articles were identified that reported relevant data. One of these
101 was also reported in
Table 1 because overt violence was an outcome measure. Two papers
34,109 were also reported in
Table 2 because they include placebo arms. No Class I studies were identified that tested this hypothesis.
Two Class II and two Class III studies reported tests of the relative efficacy of clozapine versus other antipsychotics. One Class II inpatient study
119 found that clozapine was significantly superior to chlorpromazine. The other Class II inpatient study
115 did not find a statistically significant difference in efficacy. Both of the Class III studies comparing these agents reported that clozapine was superior to haloperidol—one among inpatients,
43 the other among outpatients.
121 None of these studies controlled for the concomitant administration of other psychotropics. One Class II inpatient study
34 and one Class III outpatient study
47 reported evidence that risperidone was associated with significantly greater reduction in hostility versus haloperidol,
34 although another Class II
114 study (including both in- and outpatients) reported no difference in efficacy for this indication. One Class II
115 and one Class III study
119 both reported that clozapine was more effective than chlorpromazine. Two Class III studies reported that clozapine was more effective than haloperidol.
43,121 Single Class III studies reported the relative superiorities of haloperidol versus thiothixene,
118 haloperidol versus risperidone,
50 clozapine versus risperidone,
43 risperidone versus perphenazine,
120 and amisulpride versus haloperidol.
123We conclude that the clozapine treatment is
possibly more effective than chlorpromazine, and risperidone is
possibly more effective than haloperidol for the management of hostility among inpatients with SSDs who have not been selected for aggression and who may be receiving other psychotropic medications (Level C). The relative efficacy of clozapine versus haloperidol would qualify for Level B if one disregarded the difference between in- and outpatients, but that seems to violate the requirement for at least two
consistent Class II studies.
58–60 Given current knowledge, the comparative efficacy of other pharmacological interventions for the management of hostility among in- or outpatients is unproven (Level U).
3. Does evidence exist that any adjunctive medication will reduce overt aggression or hostility in persons with schizophrenia spectrum disorders?70–72,88,132–142 (Table 4)
Fifteen articles were identified that reported relevant data. One paper
137 was also reported in
Table 5 because the subjects were preselected for aggressiveness. Two Class I inpatient studies
132,133 and one Class II inpatient study
136 reported evidence that adjunctive propranolol, 160–640 mg/day (the majority receiving>240 mg/day) combined with neuroleptic medications reduced anger,
132 nurses’ observations of irritability,
133 or overt violence.
136 A single Class III study
137 reported a benefit from adjunctive pindolol 15 mg/day. One Class II inpatient study
135 and one Class III inpatient study
70 reported reductions in measures of impulse control or anger with adjunctive valproate. The former added valproate to risperidone; the latter added valproate to either risperidone or olanzapine. However, a third study of adjunctive valproate reported no significant benefit.
138 These studies collectively permitted concomitant administration of benzodiazepines, propranolol, chloral hydrate, benztropine and zolpidem and did not control for this factor. One Class II study
72 reported that perphenazine combined with famotidine was superior to perphenazine alone in reducing the PANSS aggressiveness risk score. One class II study
134 reported that antipsychotics plus s-adenyl methionine (SAM-e) was superior to antipsychotics alone in reducing OAS scores in a subset of patients carrying the low activity catechol-O-methyltransferase COMT codon 158 polymorphism—an effect the authors speculated might relate to SAM-e’s reported enhancement of COMT activity.
We conclude that the adjunctive propranolol at doses of 160–640 mg/day is possibly effective in mitigating irritability and/or anger in inpatients who have not been selected for aggression (Level B). Our caution (demoting the level of confidence from probable to possible despite two Class I and one Class II supportive studies) stems from the fact that the relevant studies were not consistent in either the concomitant antipsychotic agent or the measures of outcome, which technically requires demoting confidence in the evidence by at least one Class. A single positive replication study would shift the level of confidence to “probable.” We also conclude that adjunctive valproate combined with risperidone is possibly effective, acknowledging that one of the two supportive studies monitored impulsivity and the other monitored anger (Level C). Adjunctive famotidine plus perphenazine is possibly effective for reducing impulsivity among such patients (Level C). Adjunctive SAM-e, combined with antipsychotics, is possibly effective for reducing aggression risk among the subset of such patients with the low activity COMT polymorphism (Level C). Given current knowledge, the efficacy of other adjunctive medications interventions is unproven (Level U).
4. Does evidence exist that any medication will reduce overt aggression or hostility in persons with schizophrenia spectrum disorders preselected for clinically problematic aggression?36,40,57,86,93,143–159 ( Table 5)
Twenty-three articles were identified that reported relevant data. Two of these
57,93 were also reported in
Table 1 because the studies included some nonviolent patients. (That is, Buckley et al., 1995
57 investigated the impact of clozapine on seclusion and restraint occurrence among 19 “non-violent” and 11 “violent” patients.
Table 5 reports the findings with regard to the “violent” subgroup. Carney, 1984
93 investigated the impact of clopenthixol decanoate on 23 patients who exhibited a range of aggressive behavior with a mean of 1.71 on a four point scale. It was not possible to disaggregate the reduction in aggression observed among the more versus less aggressive subjects.) One study
137 was also reported in
Table 2 because this was an adjunctive therapy trial. No Class I or II studies were identified that tested this hypothesis. Two Class III reports
40,147 of what appears to have been a single RCT found evidence that, among physically assaultive inpatients, clozapine treatment was associated with greater reductions in MOAS scores compared with olanzapine or haloperidol. This study did not control for coadministration of multiple other psychotropic agents. Single Class III studies reported benefits of depot zuclopenthixol,
143 loxapine,
146 and adjunctive pindolol.
137We tentatively conclude that the clozapine is
possibly more effective than olanzapine or haloperidol for reducing aggression among physically assaultive inpatients (Level C). Our caution is related to the fact that it is not clear whether the two supportive publications
40,147 are reporting a single study. Given current knowledge, the efficacy of other medications for the management of hostility or aggression among persons with SSDs preselected for clinically problematic aggression is unproven (Level U).
Discussion
The available evidence supports several conclusions relevant to clinical practice:
1.
Paliperidone ER is probably effective for the management of hostility among inpatients with SSDs who have not been preselected for aggression (Level B).
2.
Clozapine is possibly more effective than haloperidol for the management of overt aggression and possibly more effective than chlorpromazine for the management of hostility among inpatients with SSDs who have not been selected for aggression (Level C).
3.
Clozapine is possibly more effective than olanzapine or haloperidol for reducing aggression among physically assaultive inpatients with SSDs (Level C).
4.
Adjunctive propranolol, valproic acid, and famotidine are possibly effective for reducing aspects of hostility or aggression among inpatients with SSDs (Level C).
To the best of our knowledge, this systematic review provides the first comprehensive investigation determining what is known about the efficacy of medications to manage aggression and/or violence among persons with SSDs. Even though most of the available peer-reviewed studies addressed hostility rather than overt aggression, evidence exists that verbal aggression or hostility correlate with physical aggression.
160 Moreover, in a study exploring the relationship between emotional status, cognitive capacity, and aggressive behavior among persons with SSDs, the best model for aggression behavior was a path from “anger emotion to aggressive behavior.”
161 Therefore, agents that were found to be probably or possibly effective for the management of hostility among persons with SSDs may also prove possibly effective for reducing the more serious social and public health problem of violence. We believe that the present findings offer the strongest available evidence-based guidance regarding pharmacological interventions to reduce anger, hostility, aggression, and violence among persons with schizophrenia spectrum disorders.
That having been said, at least three categories of limitations mandate caution in the interpretation of the results. First, our investigation is not the most comprehensive possible review. We elected to employ multiple search strategies and sieve multiple databases. Yet we did not pursue 1) foreign language literature, 2) abstracts, 3) gray literature, or 4) findings in the possession of the original scholars that they may not have reported. Nor did we request original data with a view toward reanalysis (e.g., controlling for concomitant administration of other psychotropic medications) or reconciliation of methodology to facilitate meta-analysis. The 804 citations and 92 qualifying publications we identified are, thus, a subset of the extant scholarly record.
Second, a limited volume of high-quality RCTs have been completed that rigorously address the efficacy of pharmacological agents for the management of aggression, especially among persons with SSDs. The limited number of publications satisfying all criteria for the highest ratings of scientific quality is perhaps a product of multiple challenges. One could fault past studies for methodological weaknesses, but we prefer to emphasize the ambitious efforts that clinical scholars have made to gather useful data under the most trying circumstances. For instance, although concomitant administration of agents such as sedative-hypnotics, antidepressants, and anxiolytics introduces a problematic confound, it is understandable that clinical researchers typically continued administering such habitual agents to hospitalized (and presumably quite ill) persons suffering from SSDs. Similarly, although dedicated aggression scholars strongly encourage distinctions between types of aggression and ideal clinical studies would investigate the efficacy of an agent on a specific aggression type, clinical psychiatric researchers are not usually trained to discriminate these nosological nuances, classification is not always easy, and it is understandable that the studies on acutely mentally ill persons may include a spectrum of semiologies under the rubric “aggression.” Ideal studies might also have tested inter-rater reliability for measures of aggression/hostility, stratified results according to subtypes of SSDs, controlled for nonspecific sedative effects, and attempted to control for many possible mediating or moderating variables such as age, age of onset, socioeconomic background, education, etc. The methodological imperfections across this literature mandate considerable caution in generalizing from the results. Yet, we honor the extraordinary efforts of those who have contributed studies in this field to date—especially the elite cohort of scholars who have done most of the heavy lifting.
As Citrome
162 pointed out, multiple structural barriers frustrate well-meaning attempts to study this issue. Definitions of aggression vary, both in the literature and according to institutional culture. Aggressive events are relatively rare, such that researcher are either obliged to default to the proxy measure, hostility, or to conduct very large trials with long baselines and study periods. There is a risk of selection bias because hostile patients are perhaps less likely to agree to (or be competent to) sign informed consents. Few clinics or hospitals are equipped to treat the most aggressive psychiatric patients. Outpatient aggression is difficult to monitor or quantify. Compliance issues frustrate both the effort to help and to study these patients. Studies that might otherwise have qualified for Class I status were demoted because of rates of completion below 80%, yet low completion rates are typical in RCTs of treatments for schizophrenia.
163 Equally problematic: pharmaceutical companies may not be motivated to attempt demonstrating that their proprietary agents qualify for FDA approval for the indication of controlling aggression. This hugely limits the potential research funding pool. Considering these challenges, it is impressive that so many investigators have carried their studies from conceptualization through publication.
Third, and perhaps the most important caveat regarding the clinical application of our findings, because of the fact that the available data were derived from studies on clinically heterogeneous subject pools, it is not possible to predict to what extent our conclusions will apply to individual patients. Again, factors including age, age of onset, multiple demographic factors, diagnostic subtype, severity, relative predominance of positive versus negative symptoms—in addition to genetic and epigenetic variation—plausibly influence the likelihood that a given treatment will benefit a given patient, yet it would require much larger studies to include representative samples of the broad spectrum of SSDs, meaningfully control for the many potential confounds, and then statistically control for multiple comparisons.
For practical reasons, some studies confined recruitment to patients previously shown to be responsive to antipsychotic medications, whereas others only recruited treatment resistant patients—each type of study applying various definitions of responsiveness or treatment resistance. Few studies employed formal typologies of aggression, such that reported measures of efficacy usually represents an average benefit (or lack thereof) in a mixed population of patients (see e.g.,
17,164), among which might be found patients exhibiting such diverse problems as 1) indiscriminate agitation, 2) impulsive aggression, 3) persistence of conduct disorder, 4) psychopathy-associated instrumental aggression, 5) chronic hostility, 6) aggression precipitated by substance abuse, 7) violence in response to specific threatening or control-override delusions, or 8) any combination of the above. It is possible (one ventures to say probable) that the efficacy of any agent is different among persons with different developmental and neurobiological pathways to, and types of, aggression.
Evidence exists that a subset of persons with SSDs exhibits cognitive impairment, variably associated with motor skills impairment, eye movement abnormalities, and cerebral atrophy—a syndrome sometimes discussed under the rubric of “deficit schizophrenia.”
165–168 Aggression among those with SSDs who exhibit neurological deficits may have a different neurobiological basis than among those who seem neurologically intact
169 and, thus, respond to different agents. Aggression among actively psychotic persons may have different determinants and medication responsiveness than aggression among persons with SSDs whose psychosis is controlled.
13 Aggression among persons with SSDs and comorbid antisocial traits is possibly associated with somewhat different neurobiological correlates
170 and may require a significantly different therapeutic approach (see
171). Aggression successfully managed by a medication among inpatients may not be efficacious among outpatients.
29 Gender or hormonal status may impact both the phenomenology and the responsiveness of SSD-related aggression.
172 Some evidence suggests that compliance is a key factor in determining the efficacy of medications for the control of aggression in SSDs.
173,174 Indeed, one paper in our review
143 explicitly demonstrated an association between compliance and efficacy. However, measures of compliance were not reported in the overwhelming majority of outpatient trials, confounding an attempt to determine whether relative efficacy was more plausibly attributable to the type of medication versus the rate of adherence.
An additional limiting factor seemed to be the rigidity of the standard method for classification of evidence. In many cases, reports were demoted from Class I to Class II only because the rate of completion was below 80%–an historically hard-to-reach criterion in studies of persons with schizophrenia. In some cases (e.g.
46), reviewers felt constrained by the strict adherence to one or more rules that required demotion from Class II, despite seemingly strong evidence of efficacy. In some cases (e.g.
48), reviewers felt compelled to demote a report because some simple piece of information was missing, perhaps due to oversight that could perhaps have been readily overcome by the investigators. In essence, coauthors of the present manuscript expressed concern that a strict application of the AAN classification scheme–e.g., requiring for Class I that only the impact on primary outcome measures be considered and that at least 80% of enrolled subjects completed the study–might sometimes be at odds with the realities of clinical psychiatric research, and sometimes lead to a failure to capitalize on valuable data.
One difficult-to-quantify trend seemed to emerge from this review: several investigators noted that most or all of the benefit for the management of hostility or aggression was apparent early in the course of the trial. In Chiles et al.,
87 for example, all the improvement apparently occurred between weeks 2 and 4 of treatment. In Dalal et al.
94 the reduction in violence occurred only in the early phase. One might tentatively conclude that, while the anti-aggressive benefit may not emerge immediately, an empirical trial of perhaps one month should be sufficient to gauge the likelihood of response to an antipsychotic medication. Moreover, some evidence suggests the possibility that mood stabilizers may produce whatever benefit they will within one week.
138 If confirmed, this suggestion would both clarify the required duration of future short-term inpatient studies and conceivably enhance the clinical appeal of agents shown to have a quicker onset of efficacy.
The association between SSDs, aggression, and substance abuse deserves special comment. Evidence shows that person with schizophrenia who also exhibit alcohol dependence or other substance abuse are significantly more likely to commit violent acts (e.g., see references
2,6,20,175). It is possible that comorbid stimulant abuse is especially dangerous.
176 Yet, the overwhelming majority of the empirical research on the efficacy of interventions fails to 1) report having assessed substance abuse systematically and 2) fail to stratify results between patients with and without comorbid substance abuse. As challenging as the research would be, one must urge accounting for dual diagnosis in future trials.
Considering the manifold barriers to definitive scholarship in this field, it would be imprudent to propose a unitary pharmacological algorithm. It would require a massive multicenter RCT, stratifying for multiple demographic, clinical, and biological variables, to provide practice parameters meeting the new Institute of Medicine requirements for the development of a practice parameter,
177 let alone to provide reliable recommendations regarding the optimum intervention for a given patient. That having been said, based on a rigorous analysis of the available data, the authors provisionally recommend that clinicians consider a trial of paliperidone for the management of persistent hostility among persons with SSDs.
Aggression and violence committed by persons with SSDs causes both personal and public tragedies. Several recent notable mass murders have been attributed to persons suspected of having schizophrenia.
178–181 We cannot opine regarding any individual case, especially when diagnostic information is only available from the popular media. However, given the multiplicity of public and private tragedies attributable to schizophrenia-related aggression, the neuropsychiatric community may wish to rethink the research strategy most likely to generate clinically useful results.
Based on the present review–and acknowledging the extraordinary practical barriers to funding and conducting a definitive trial–we propose that a state-of-the-art study of neuropharmacological management of aggressive and violent behavior among persons with SSDs would ideally contain the following elements:
1.
To mitigate the confounding variable of diagnostic heterogeneity, all subjects should share a single, relatively unitary DSM diagnosis, such as Schizophrenia.
2.
The study should control for or exclude subjects with concomitant psychopathy or antisocial traits.
3.
An ideal research design might begin with an inpatient phase to (a) permit comprehensive baseline assessment, (b) rule out conflating neurological/medical issues, and (c) achieve stabilization under conditions of known compliance. However, given the relatively high rate of noncompliance with drug therapy among outpatients with schizophrenia (e.g.
182), and grossly different situational factors in in- versus out-patient settings in regard to potential triggers of or opportunities for aggression, measures of efficacy based on inpatient studies cannot be presumed to have ecological validity. The efficacy of an agent for reducing the risk of community aggression can best be tested via follow-on outpatient studies.
4.
Given the intermittent nature of overt aggressive episodes, a 2- to 3-year duration should be required.
5.
Subjects should be able to tolerate treatment with a single psychotropic medication. That is, either no concomitant medications should be administered, or perhaps all patients should receive the same low dose of an anti-Parkinsonian agent.
6.
To mitigate the serious confounding factor of compliance, antipsychotics should be administered in depot form.
7.
Given preliminary evidence of the efficacy of antipsychotic medications and the impracticality of a placebo controlled study, the design should either (a) compare of two or more depot antipsychotic medications or (b) assess the efficacy of an adjunctive agent among subjects all of whom are receiving the same depot antipsychotic.
8.
The design should control for nonspecific sedation.
9.
To significantly enhance the validity of measurement and to help control for the heterogeneity of type of aggression, none of the items or combinations of items from the PANSS/BPRS should serve as the independent variable. Instead, investigator should ideally employ at least two normed, validated, reliable measures of aggression.
183 A promising design would perhaps combine an established self-rated instrument such as the Aggression Questionnaire
184 with an observer-rated instrument that can be adapted for outpatient use such as the Social Dysfunction and Aggression Scale
77 or a recent revision of the OAS that offers improved assessment of precipitants, the Overt Aggression Scale—Modified for Neurorehabilitation.
185In the meantime, one is obliged to synthesize what is known, identify the research gaps and the most promising interventions, and utilize the limited available knowledge in clinical practice while working toward a better understanding of the bio-psycho-social determinants of SSD-related aggression.
Acknowledgments
The authors thank Janice Adelman, Ph.D., Claremont Graduate University; Patricia Erwin, M.L.S., Mayo Clinic Library; and Evans Whittaker, M.D., Ph.D., Norris Medical Library.