Case Report
“Ms. A” is a 50-year-old homeless woman who was brought in by her shelter staff with increasing erotomanic and persecutory delusions that began occurring over the preceding months. The patient’s medical history was significant for a left frontal lobe anaplastic oligoastrocytoma and oligodendroglioma status postsurgical resection and adjuvant radiotherapy, as well as posttraumatic stress disorder related to intimate partner abuse, but no known substance abuse.
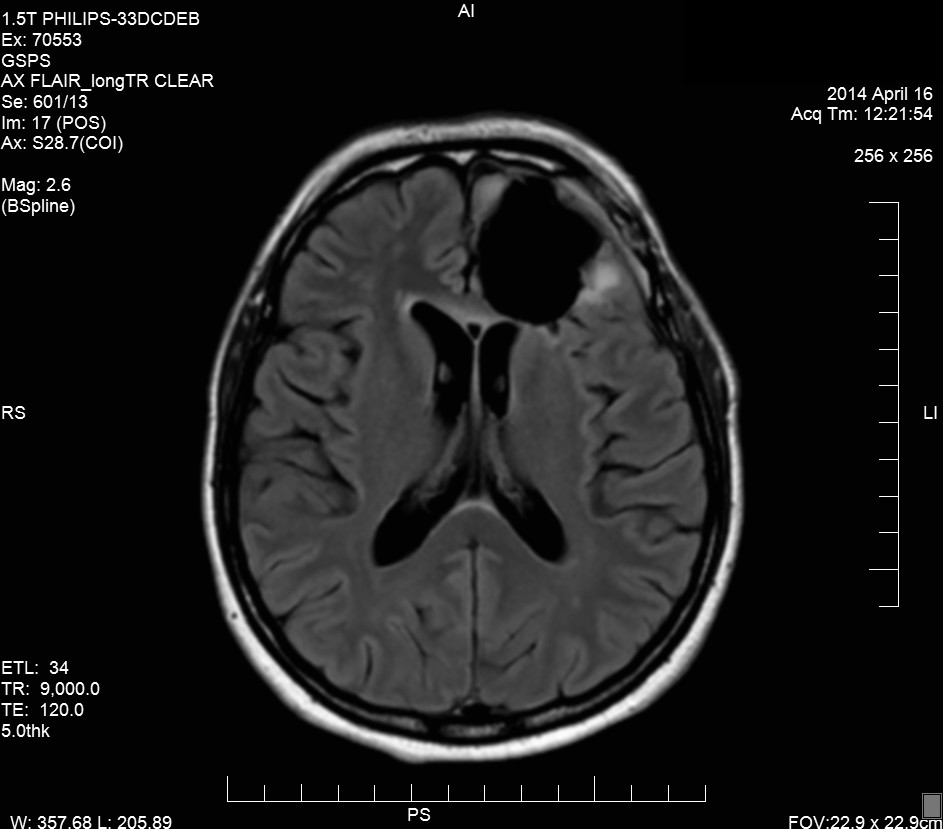
Her brain tumor was diagnosed 3 years before her psychiatric hospitalization when workup of her first and only known seizure revealed a left frontal lobe anaplastic astrocytoma. She was prescribed levetiracetam for seizure prophylaxis but was lost to follow-up until the following year, when repeat MRI showed a large frontal mass with edema and midline shift (
Figure 1). The tumor was resected in two pieces measuring 2.5×2.3×1 cm and 7×5.5×2 cm, identified as anaplastic oligoastrocytoma and oligodendroglioma, and treated with adjuvant radiotherapy over 2 months with successful resection demonstrated by posttreatment imaging (
Figure 2). Her first documented psychotic symptoms were at a follow-up appointment 1 month after her final radiotherapy treatment, when she reported thinking that her phones were tapped and that hospital staff had been putting lies in her chart, for instance, saying that she is a lesbian when she is not.
On presentation, the patient described an ongoing romantic relationship with the famous lead singer of the band Coldplay, Chris Martin, and persecutory delusions regarding his ex-wife, the famous actress Gwyneth Paltrow. One year prior to presentation, the patient reported that she heard the song “Magic” by Coldplay and believed the song was meant for her. She claimed that Mr. Martin began meeting her in public and proposed to her. Her paranoia and psychosis prompted her to move herself and her daughter from her sister’s home to a nearby women’s shelter. Over the next few months, the patient became increasingly paranoid of her shelter staff, believing that she and her daughter were being spied on through holes in the walls, which prompted her hospitalization. Computed tomography, lumbar puncture, and electroencephalogram were unremarkable. MRI confirmed that she was status post left frontal craniotomy. There was no sign of acute infarction. She was then transferred to inpatient psychiatric care for management of her symptoms.
Prior to admission, the patient had been started on risperidone (1 mg) and a cross-taper to replace levetiracetam with divalproex. Throughout hospitalization, she was pleasant but remained frankly delusional and paranoid of staff, continuing to endorse her erotomanic and persecutory delusions, as well as ideas of reference regarding Coldplay songs. While her Montreal Cognitive Assessment score was 28/30, neuropsychological testing revealed gross cognitive functioning within the low-average range, borderline to severely impaired processing speed, severe impairment of cognitive flexibility, phonemic fluency, and confrontation naming and moderate impairment of noncontextual verbal learning, which taken together are consistent with left frontal lobe dysfunction.
Risperidone was eventually increased to 5 mg per day (3 mg in the morning and 2 mg in the afternoon), and while the patient became less paranoid of staff and less preoccupied with her delusions, she failed to develop insight into her condition, and her delusional system around Mr. Martin and Ms. Paltrow persisted. She refused long-acting risperidone injections on discharge but agreed to be compliant with her oral medications. She was discharged into the care of her sister, who agreed to help the patient manage her care and medications.
Discussion
The patient presented in this case represents, in many ways, a classical picture of erotomania.
1 The subject of her delusion was a famous celebrity and occurred within the context of a persecutory delusion and more general prodromal paranoia.
2 While her delusional system was fixed and poorly responsive to pharmacotherapy, it did gradually become less intrusive and the patient slightly less paranoid. This improvement was seen as medications took effect, and a therapeutic relationship developed with her mental health care providers, as might be expected with a primary delusional disorder. However, the etiology of the patient’s symptoms appears to be unique.
The etiology of delusional disorders as a whole remains poorly understood.
3 Neuroanatomical studies have linked asymmetry of temporal and frontal lobes to schizophrenia and delusional disorders
4 and have been shown to be attributable to many CNS pathologies,
5 but anatomical evidence for frontal lobe dysfunction in nonschizophrenia delusional patients is more limited.
The neuroanatomical functioning of the frontal lobe is divided into five tracts distinguished by their connections between the basal ganglia, thalamus, and frontal lobe and consist of motor, oculomotor, and three cognitive-affective circuits: the dorsolateral prefrontal (DLPF), the lateral orbitofrontal, and the cingulate circuits.
6 While the damage to the cingulate and orbitofrontal circuits are associated with functions such as impulsivity and amotivation not seen in Ms. A’s case, damage to the DLPF is associated with problems with cognitive rigidity, verbal fluency, and working memory. Given the impairment of cognitive flexibility, phonemic fluency, confrontation naming, and noncontextual verbal learning shown by Ms. A’s neuropsychological testing, it seems highly likely that sequelae of her tumor involve damage to the DLPF, which underlies the interplay between her delusions and cognitive deficits.
Interestingly, Ms. A’s cognitive deficits present a compelling link to those of other erotomanic patients seen in the literature. Fujii et al.’s presentation of two erotomanic patients with left frontal lobe dysfunction describes a similar clinical picture of erotomania superimposed on symptoms of paranoia with decreased frontal and temporal lobe functioning.
6 These two patients and Ms. A demonstrated decreased left frontal lobe functioning evidenced by considerable cognitive inflexibility and verbal learning, which is thought to contribute to the fixed nature of the observed delusional systems. However, these patients also showed evidence of temporal lobe dysfunction not observed in Ms. A, which may be due to the more focal nature of Ms. A’s brain tumor in precipitating her clinical presentation.
While Ms. A’s prognosis appears similar to other cases of delusional disorder, erotomanic and persecutory subtypes, her case contributes to the growing body of observed etiologies of this diagnosis and may be of use to clinicians forecasting treatment strategies and prognosis for patients with a similar clinical picture.