Positive childhood experiences—such as feeling safe and supported by one’s family and/or having supportive adults other than parents—appear to modulate or even outweigh the effects of adverse childhood experiences on adult mental health, according to a report in JAMA Pediatrics.
Moreover, the effect of positive childhood experiences on adult depression or poor mental health appears to be dose related: The more positive childhood experiences one recalls, even in the presence of adverse childhood experiences, the less likely he or she is to report depression or poor mental health.
“PCEs [positive childhood experiences] may have lifelong consequences for mental and relational health despite co-occurring adversities such as ACEs [adverse childhood experiences],” wrote Christina Bethell, Ph.D., M.B.A., M.P.H., a professor in the Department of Population, Family, and Reproductive Health at Johns Hopkins Bloomberg School of Public Health, and colleagues. “Even as society continues to address remediable causes of childhood adversities ..., attention should be given to the creation of those positive experiences that both reflect and generate resilience within children, families, and communities.”
Bethell and colleagues analyzed data on more than 6,000 adults responding to the 2015 Wisconsin Behavioral Risk Factor Survey, a telephone survey of noninstitutionalized Wisconsin adults 18 years and older. The survey, which is coordinated by the Centers for Disease Control and Prevention and carried out in all 50 states, collects information about residents’ health, use of preventive services, and more.
The survey measured positive childhood experiences by asking respondents to report how often or how much as a child they experienced the following:
•
Being able to talk to their family about feelings.
•
Feeling their family stood by them during difficult times.
•
Participating in community traditions.
•
Feeling a sense of belonging in high school.
•
Feeling supported by friends.
•
The presence of at least two nonparent adults who took genuine interest in them.
•
Feeling safe and protected by an adult in their home.
The survey respondents were also asked how often they experienced the following as children:
•
Physical or emotional abuse or neglect.
•
Household dysfunctions such as substance abuse, parental incarceration, and divorce.
Adult depression and poor mental health were assessed two ways: respondents were asked whether a physician or other health professional ever told them they have a depressive disorder; they were also asked how many days during the previous 30 days their mental health was “not good.” (A score of 14 or more on the latter question indicated poor mental health.)
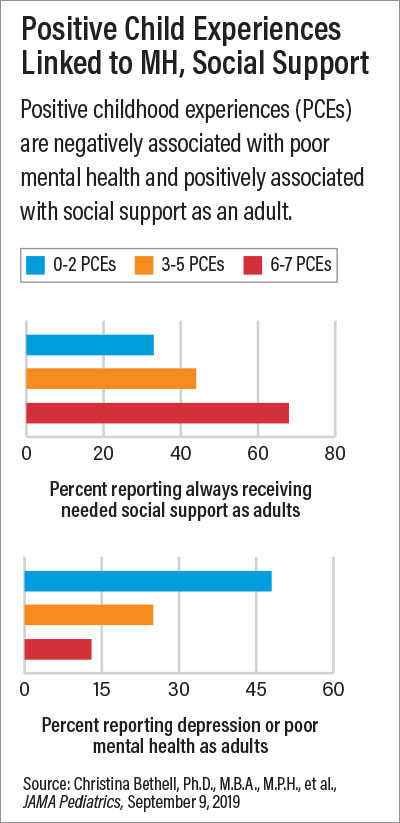
Finally, the survey assessed adult social and emotional support with the following question: “How often do you get the social and emotional support you need?” Bethell and colleagues found 52.3% of respondents reported six to seven positive childhood experiences; 56.7% reported at least one adverse childhood experience, and 13.7% reported four to eight adverse childhood experiences. A total of 21.2% met criteria for depression or poor mental health, and 55.1% reported “always” getting the social and emotional support they need.
Compared with those reporting six to seven positive childhood experiences, adults reporting two or less positive childhood experiences had nearly four times higher prevalence of depression/poor mental health (48.2% versus 12.6%). Those with fewer positive childhood experiences were also less likely to report “always” getting the social and emotional support they needed.
The JAMA Pediatrics report builds on accumulating evidence demonstrating that adverse childhood experiences do not have to be determinative of future mental health.
“[These] results hold promise for national, state, and community efforts to achieve positive child and adult health and well-being by promoting the largely untapped potential to promote positive experiences and flourishing despite adversity,” Bethell and colleagues wrote.
APA Past President Dilip Jeste, M.D., in comments to Psychiatric News, said the finding that positive childhood experiences reduce the risk of depression and poor mental health, even after controlling for adverse childhood experiences, has major implications. Jeste, a distinguished professor of psychiatry and neuroscience, and director of the Sam and Rose Stein Institute for Research on Aging at the University of California, San Diego (UCSD), has pioneered research on positive psychiatry.
In a study published last year in the Journal of Clinical Psychiatry, Jeste and colleagues found that among patients with schizophrenia as well as healthy subjects, childhood adversity was associated with worse physical, cognitive, and mental health and worse biomarkers of insulin resistance. Yet for subjects in the study who scored high on measures of resilience, the reverse was true. (The lead author on the study was Ellen Lee, M.D., a postdoctoral fellow in geriatric mental health in the Department of Psychiatry at the UCSD).
“The most interesting finding was that resilience seemed to counteract the effects of childhood adversity in both the groups,” Jeste said. “That is, people with a history of childhood adversity but high resilience did as well as or even slightly better than those who did not have childhood adversity but had low levels of resilience.”
In another study led by Lee and Jeste, appearing in the December 2018 International Psychogeriatrics, they found that higher scores on measures of wisdom in older people appeared to negate the adverse effects of loneliness on physical, cognitive, and mental health.
“Both these studies were cross-sectional [as is the JAMA Pediatrics survey] and thus cannot establish a causal relationship,” Jeste said. “Nevertheless, they support the results of the paper by Bethell and colleagues that positive psychosocial factors may overcome or at least neutralize the adverse impact of negative life events or traits on health. These findings point to the role of positive psychiatry in individuals’ health and well-being.”
The study by Bethell and colleagues was funded in part by the Robert Wood Johnson Foundation, the Health Resources and Services Administration, and the National Center for Advancing Translational Sciences. ■
“Positive Childhood Experiences and Adult Mental and Relational Health in a Statewide Sample: Associations Across Adverse Childhood Experiences Levels” is posted
here. “The Protective Role of Resilience in Mental and Physical Health and Metabolic Markers” is posted
here. “High Prevalence and Adverse Health Effects of Loneliness in Community-Dwelling Adults Across the Lifespan: Role of Wisdom as a Protective Factor” is posted
here.