Cigarette smoking among individuals with behavioral health conditions (BHCs) is a critical public health problem. Persons with BHCs have higher prevalence of tobacco use disorders, more severe nicotine dependence, and greater difficulty quitting smoking compared with persons without BHCs (
1–
4). Spending up to 25% of their income on cigarettes (
5) and consuming 44% of purchased cigarettes in the United States (
6), adults with BHCs are affected disproportionately by tobacco-related diseases and die, on average, 25 years prematurely (
7–
11). Although overall smoking prevalence (
12) and severity of nicotine dependence among smokers have declined in recent decades (
13,
14), the decreases have been smaller or nonexistent among persons with BHCs (
14–
18). This suggests that smoking-related disparities between persons with and without BHCs may be increasing.
Lack of health insurance and reduced access to affordable smoking cessation treatments potentially contribute to elevated smoking prevalence among persons with BHCs (
19,
20). Tobacco cessation treatments, including brief advice to quit, behavioral counseling, and pharmacotherapy, are evidence based and cost-effective, and they decrease the likelihood of tobacco relapses (
21). Smokers with BHCs are equally as likely or more likely to want to quit smoking compared with smokers in general (
22). However, advice to quit and resources for quitting may be less accessible for those with BHCs, in part because of inequitable access to high-quality health care. Existing research on longitudinal disparities in smoking among adults with and without BHCs has primarily used data from national surveys (
14–
18). It is unknown whether smoking disparities also persist within an integrated health care delivery system with convenient and affordable access to smoking cessation interventions. This gap in the literature is noteworthy, given that access to affordable, integrated health care is expected to increase as a result of health reform. As a result, integrated health care delivery systems are increasingly important settings for connecting vulnerable subgroups of smokers with effective cessation treatments.
This study examined smoking trends in a large sample of participants with and without BHCs in an integrated health care delivery system. Using the electronic health record (EHR), we aimed to describe smoking prevalence from 2010 to 2013 among individuals with one or more of the five most prevalent BHCs and individuals without BHCs; evaluate whether patients with BHCs had higher odds of smoking over time compared with patients without BHCs, after the analyses were adjusted for covariates; and examine evidence for equitable access to treatment by testing for differences in tobacco cessation medication utilization in 2010 among a subset of matched pairs of smokers with and without BHCs.
Methods
Setting
Kaiser Permanente of Northern California (KPNC) is a nonprofit, integrated health care delivery system providing comprehensive health services to more than 3.4 million members in 2010, who comprise 44% of the commercially insured population in the region. KPNC provides integrated general medical and behavioral health treatment and is a recognized leader in establishing tobacco quality-of-care standards (
23). The membership is largely employed, working or middle class, and racially and socioeconomically diverse, and it is highly representative of the entire population of the geographic area.
Study Participants
We utilized EHR data from a retrospective study that identified all adults ages 18 or older with a KPNC visit in 2010 who had one or more of the five most prevalent BHCs on their diagnosis list (includes current and preexisting diagnoses of depressive disorders, anxiety disorders, substance use disorders other than tobacco use disorder, bipolar and related disorders, and attention-deficit hyperactivity disorder [ADHD]). The sample represented 11% of adult patients with a KPNC visit in 2010. [A list of the relevant ICD codes for the five most prevalent BHCs in KPNC in 2010 is available as an online supplement to this article.]
Each patient with one or more BHC was matched on sex, age, and medical facility to a patient without BHCs. Matching by medical facility accounted for any potential differences in services offered by geographic region (
24). Rates of BHCs are higher in Medicaid and Medicare populations, so individuals insured by public programs were excluded to prevent oversampling of these patients in the BHC group. Sample participants were required to be members of KPNC for at least 75% of the study period (
25).
The final analytical sample consisted of 311,466 individuals, including 155,733 individuals with at least one of the top five BHCs (depressive disorders [N=96,410], anxiety disorders [N=69,928], substance use disorders [N=22,259], bipolar and related disorders [N=8,357], and ADHD [N=6,611]), and 155,733 individuals with no BHCs. Institutional review board approval was obtained from the Kaiser Research Foundation Institute.
Measures
Smoking status was obtained through standardized screening at all KPNC adult medicine appointments and recorded in the EHR. For each year, current smokers or those with a tobacco-dependence diagnosis were coded as smokers. Individuals who had never smoked and former smokers were coded as nonsmokers.
KPNC patient visits were classified into four categories: primary care, other outpatient (such as dermatology and psychiatry), inpatient, and emergency department. Because patients are more likely to be asked about their smoking status during certain types of visits, we controlled for the number of different types of visits received by each patient during each year. Categorical variables for each type of visit and a variable reflecting the sum of the number of different visit types (1–4 in 2010 or 0–4 in 2011–2013) were created for each year. The results of the models were the same regardless of whether they included individual visit indicators and a count of different visit types, so the count variables for each year were retained as covariates in all models.
Receipt of any tobacco cessation medications from a KPNC pharmacy during the year in which the cohort was created (2010) was obtained from the EHR. Tobacco cessation medications included nicotine patches, lozenges, gums, inhalers, and nasal spray; bupropion; and varenicline. Participants had coverage for all seven smoking cessation medications approved by the U.S. Food and Drug Administration; however, varenicline, nicotine inhalers, and nicotine nasal spray were nonformulary, and providers were required to use an exception code to indicate why those treatments were provided rather than a formulary treatment. We were unable to differentiate use of bupropion for the treatment of smoking versus depression, and any form of bupropion was counted as a tobacco cessation medication if the patient was a smoker.
Sex, age, and race-ethnicity were pulled from the EHR. Race-ethnicity was collapsed into five categories: white, black, Hispanic, Asian (including Native American and Hawaiian/Pacific Islander), and unknown or other. Median annual household income was geocoded on the basis of members’ addresses and reflected members’ neighborhoods; the results were dichotomized as 1 (≥$50,000) or 0 (<$50,000).
Analysis
Analyses were performed using SAS software, version 9.3. Frequencies and means were used to describe patient characteristics and smoking status over time between patients with versus without BHCs for each of the five BHCs examined. Differences in patient characteristics and smoking status by BHC status were examined using McNemar’s and paired t tests (
26). Cross-sectional multivariate logistic regression models were run to examine the odds of smoking during each year (2010–2013) among patients with BHCs compared with patients with no BHCs, by BHC type.
At KPNC smoking status has been documented in the EHR with increasing consistency in recent years, and the percentage of patients in our sample with missing smoking status data decreased significantly over time. However, among all smoking status data examined from 2010 to 2014, 23% of the data were missing. Missing smoking status data were associated with being male, younger, and Asian and having unknown or other race. To address missing data for smoking status across years and for median household income in 2010 (2%), we implemented standard multiple imputation methods using PROC MI and MIANALYZE in SAS (
27–
29). This technique created ten complete data sets, all with plausible values for each missing value. We used a repeated-measures, generalized estimating equation (GEE) framework, including time × BHC status (BHCs or no BHCs) interactions, to examine the odds of smoking over time among patients with or without BHCs. PROC MIANALYZE was used to combine the results from the ten data sets and generate valid estimates and adjusted standard errors for inference (
27,
29). All models adjusted for age, sex, race-ethnicity, median household income, and visit type count (
30). Although patients with and without BHCs were matched on age and sex, these variables were retained in the final models to allow for interpretation regarding smoker status (
30).
Finally, as a secondary aim, we examined prevalence of tobacco cessation medication use among a subset of matched pairs of smokers with and without BHCs in 2010 using logistic regression analyses. Multiple imputation was used to address missing income data, as described above.
Results
The sample was 64% women, 60% white, 16% Hispanic, 14% Asian, and 7% black; 3% reported unknown or other race-ethnicity. Participants’ mean±SD age was 50±15 years old, and 68% had a median household income of ≥$50,000. With the exception of adults with ADHD, fewer patients with BHCs had a median household income of ≥$50,000 compared with patients without BHCs (
Table 1). The percentage of white patients was higher and the percentage of Asian patients was lower among patients with BHCs compared with patients without BHCs (
Table 1). Co-occurring BHCs were common in the sample as a whole (
Table 2).
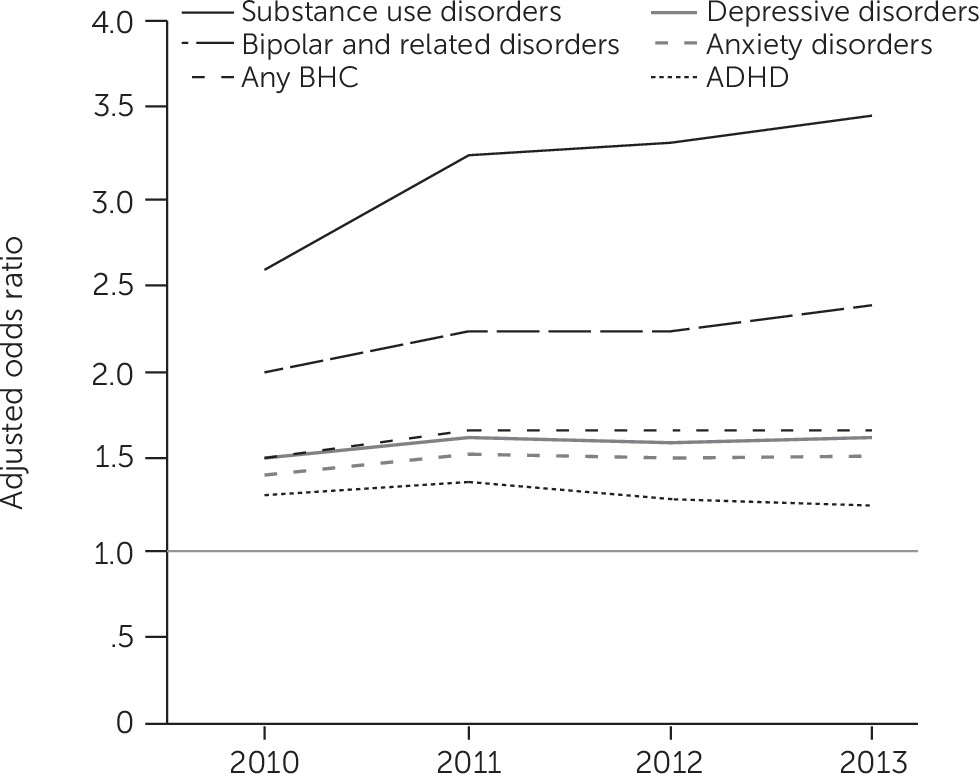
Patients with BHCs had significantly higher odds of smoking compared with patients without BHCs during each year (p<.001) (
Figure 1). Patients with substance use and bipolar disorders had the largest odds of smoking each year, and their odds of smoking increased over time relative to patients without BHCs. Odds ratios comparing the likelihood of smoking among patients with and without BHCs remained fairly stable over time for the other three BHCs examined.
Repeated-measures, multivariate logistic regression GEE models indicated that women, older adults, and patients with household incomes of ≥$50,000 had lower odds of smoking compared with men, younger adults, and patients with incomes under $50,000, respectively (
Table 3). Compared with white adults, black adults were more likely to smoke, and Asians, Hispanics, and adults of unknown or other race-ethnicity were less likely to smoke. Utilization of a greater number of visit types was associated with a greater likelihood of smoking. Patients with BHCs had higher odds of smoking compared with patients without BHCs. Time was significant in all models, indicating a declining trend in smoking over time for patients without BHCs. Significant BHC status × time interactions indicated that with the exception of ADHD, the odds of smoking decreased more slowly over time for those with BHCs versus without BHCs.
Among the subset of 2,858 matched pairs of smokers in 2010, 6.2% of persons with BHCs and 3.6% of persons without BHCs used any tobacco cessation medications that year (p<.001). Together, the matched pairs used the nicotine patch most commonly (70%), followed by varenicline (28%), nicotine gum (7%), nicotine lozenges (3%), nicotine inhaler (1%), nicotine nasal spray (.5%) and bupropion (.5%). The patch was used more frequently by patients with BHCs compared with patients without BHCs (4.5% and 2.3%, respectively, p<.001); utilization of other medications did not differ significantly by BHC status.
With the exception of patients with ADHD, patients with BHCs had significantly higher odds of using any tobacco cessation medications compared with patients without BHCs (
Table 4). Among smokers with anxiety and substance use disorders, whites had greater odds of using any tobacco cessation medications compared with Hispanics. Among smokers with depression, whites had greater odds of using any tobacco cessation medications compared with Asians. Overall, older patients had higher odds of using tobacco cessation medications compared with younger patients. Tobacco cessation medication use did not significantly differ by sex or income (data not shown).
Discussion
To our knowledge, this study was the first to compare smoking status over four years between individuals with and without BHCs in a large, integrated health care delivery system with easy access to tobacco treatment. Lack of health insurance and reduced access to affordable smoking cessation treatments have been suggested as potentially modifiable factors that contribute to disparities in smoking rates among persons with BHCs (
19,
31). However, results from this study indicate that smoking disparities may be increasing among persons with BHCs, even within a largely employment-based health care delivery system. In 2010, 20.1% of patients with BHCs were current smokers compared with 10.4% of patients without BHCs. Smoking prevalence dropped significantly for both groups from 2010 to 2013, but the declines were more gradual among adults with BHCs.
The greatest disparities in the decline in smoking rates were among patients with substance use and bipolar and related disorders; 33.4% of patients with a substance use disorder continued to smoke in 2013 compared with 9.2% of matched adults with no BHCs. Among patients with bipolar and related disorders, 22.0% continued to smoke in 2013, compared with 8.7% of matched adults with no BHCs. By comparison, 12.5% of adults overall in California smoked in 2013 (
32). Notably, rates of smoking among adults with ADHD did not differ from rates among adults without ADHD over the four-year period. Smoking prevalence among matched patients without BHCs was highest in the comparison groups for substance use disorders and ADHD, likely because of the higher percentage of males in these groups and the higher prevalence of younger adults among patients with ADHD.
Notably, adults with BHCs (with the exception of ADHD) were more likely than those without BHCs to utilize tobacco cessation medications. These findings are consistent with research suggesting that greater psychiatric symptoms are associated with greater motivation to quit smoking and greater use of pharmacotherapy (
33,
34). They complement national findings that the odds of using cessation medications among smokers who are actively trying to quit are higher among those who saw a mental health professional in the past year compared with those who did not (
35). Yet, regardless of behavioral health status, few smokers used cessation medications, highlighting an important missed opportunity to connect smokers with effective cessation treatments. These findings are consistent with data from the U.S. Department of Veterans Affairs indicating that only approximately 7% of smokers utilized tobacco cessation medications in 1999–2002 (
36). However, it is difficult to make national comparisons, given that most studies that evaluate tobacco cessation medication utilization are limited to smokers who are actively trying to quit smoking (
37).
Among the subset of smokers who utilized any tobacco cessation medication in 2010, the nicotine patch was the most commonly used. Notably, use of bupropion was very low and did not differ significantly by BHC status. Greater receipt of tobacco cessation medications in more recent years was likely due in part to system-level changes that reduced barriers to treatment access. For example, beginning in 2012, KPNC patients were no longer required to participate in smoking cessation counseling in order to receive tobacco cessation medications.
Results from this study highlight that large disparities in smoking remain between persons with and without BHCs. These findings suggest that access to health care does not necessarily equate to provision or utilization of tobacco cessation treatments and indicate that attempts to reduce smoking disparities will need to go beyond improving health care access. Behavioral health professionals are well positioned to deliver tobacco treatments, and patients with BHCs would be served by embedding tobacco cessation treatment within substance use and psychiatry specialty clinics. Research has found that integrating tobacco treatments into mental health care and substance use treatment results in higher quit rates compared with stand-alone tobacco treatments (
22,
38). Patients see behavioral health providers more frequently compared with other providers, thereby increasing opportunities to reinforce tobacco treatment, and even brief advice to quit smoking from a health care provider improves the likelihood that smokers will quit smoking (
21).
Quitting smoking is associated with long-term reductions in depression, anxiety, and stress and with improvements in well-being—outcomes that are similar in magnitude to the effectiveness of antidepressant medications, according to a consistent and growing body of evidence (
39). Evidence-based guidelines recommend that smokers be given advice to quit and pharmacotherapy at every health care encounter. Yet, historically, behavioral health professionals have neglected to treat tobacco dependence, and smoking cessation is rarely prioritized and infrequently addressed in behavioral health settings (
40). Systemic factors, including targeted tobacco industry marketing to persons with mental illness (
41) and a lack of education for behavioral health professionals in treating tobacco dependence (
42), have contributed to the problem. The structural and individual barriers that impede treating smoking in psychiatry and chemical dependency specialty clinics must be addressed to increase the likelihood that these interventions are provided for these patients at every encounter. The American Psychiatric Association has recognized tobacco as a national priority area for mental health care and has formed a tobacco use disorders work group to better disseminate evidence for tobacco treatment and best practices. Health care systems could benefit greatly by disseminating these recommendations widely to behavioral health professionals.
This study had several limitations. The prevalence of BHCs in the EHR may be underestimated, given that some patients with BHCs do not seek treatment and therefore their conditions would not be documented. Furthermore, 23% of patients were missing data on smoking status at some time during the study period. Patient were included in the study if they had any KPNC visit in 2010, and it is assumed that patients are more likely to be asked about their smoking status during a primary care appointment compared with other types of visits. However, among those with missing smoking status data at study intake (2010), 82% had a primary care visit during that year (patients may have had other types of visits as well). Although the study was limited by the data available, we addressed missing data through valid multiple imputation methods. Analyses of tobacco cessation medication use were limited to medication fills within KPNC pharmacies among the subset of matched pairs of smokers in 2010 with and without BHCs, and results should be interpreted with some caution. Nicotine replacement therapy is available over the counter, and this study may underestimate use of these products.
Our sample is representative of primarily employed adults who receive care in an integrated health care delivery system and may not reflect all smokers with BHCs, who are underrepresented in the health care system. Although smoking disparities were clear from this study, the gap may be even wider when persons with other serious mental illnesses, such as schizophrenia, and persons with public insurance are considered. Finally, future studies should also examine patterns of changes in smoking status and diagnosis of BHCs over time as well as provider advice to quit and provider prescription patterns.
Conclusions
A multifaceted approach to reducing tobacco use disorders, including regular advice to quit smoking, has contributed to large reductions in smoking prevalence overall among the members of this health system (
23). However, there is a great deal of room for improvement: findings highlight the need to address growing disparities in smoking among adults with BHCs. In particular, results draw attention to the high odds of smoking over time among adults with substance use and bipolar disorders compared with adults without BHCs.
Equally troubling is the low use of tobacco cessation medications among patients with BHCs. Although virtually all patients with BHCs had at least one visit to a health care provider each year, few utilized smoking cessation medications, signaling a clear need for health systems to better link smokers with BHCs to effective tobacco treatments. Public health objectives, such as improvement and implementation of effective prevention interventions for BHCs, are also needed. The passage of health care reform, including comprehensive coverage of tobacco cessation medications, has provided a new opportunity to connect individuals with BHCs and effective tobacco cessation treatments; however, the public health impact of the new legislation will be limited if these products are not provided to priority populations for tobacco control. It would behoove health care systems to prioritize smoking cessation for members with BHCs and, if needed, modify organizational policies and clinical practices to better facilitate access to, and use of, appropriate and effective tobacco cessation medications as part of standard behavioral health treatment.