Coding of self-harm or possible suicidal behavior changed significantly with the transition from ICD-9-CM to ICD-10-CM. Health systems that use diagnosis codes to monitor rates of suicide attempts should consider the impact of this change to distinguish real trends from coding artifacts. We used data from ten health systems in the Mental Health Research Network (MHRN) to track rates of injury or poisoning diagnoses, classified as either self-inflicted or of undetermined intent, across the October 2015 transition.
In ICD-9-CM, self-harm was indicated by recording additional cause-of-injury diagnoses in the range E950–E958 (definitely self-inflicted) or E980–E988 (unknown if accidental or self-inflicted). For example, intentional benzodiazepine overdose was indicated by a primary diagnosis of 969.4 and an additional diagnosis of E950.0. In ICD-10-CM, self-harm is indicated within the primary diagnosis by a required cause-of-injury code, typically found in the fifth or sixth position. For example, T42.4X2 indicates intentional benzodiazepine overdose, whereas T42.4X4 indicates overdose of undetermined intent.
Diagnoses were extracted from federated data warehouses containing electronic medical record and insurance claims data (
1) from April 2014 through March 2016 at each participating site: Group Health Cooperative (Washington), HealthPartners (Minnesota), Essentia Health (Wisconsin), Henry Ford Health System (Michigan), and five Kaiser Permanente regions (Colorado, Georgia, Hawaii, Southern California, and Oregon). Monthly rates of persons receiving a diagnosis of interest were calculated relative to total monthly enrollment.
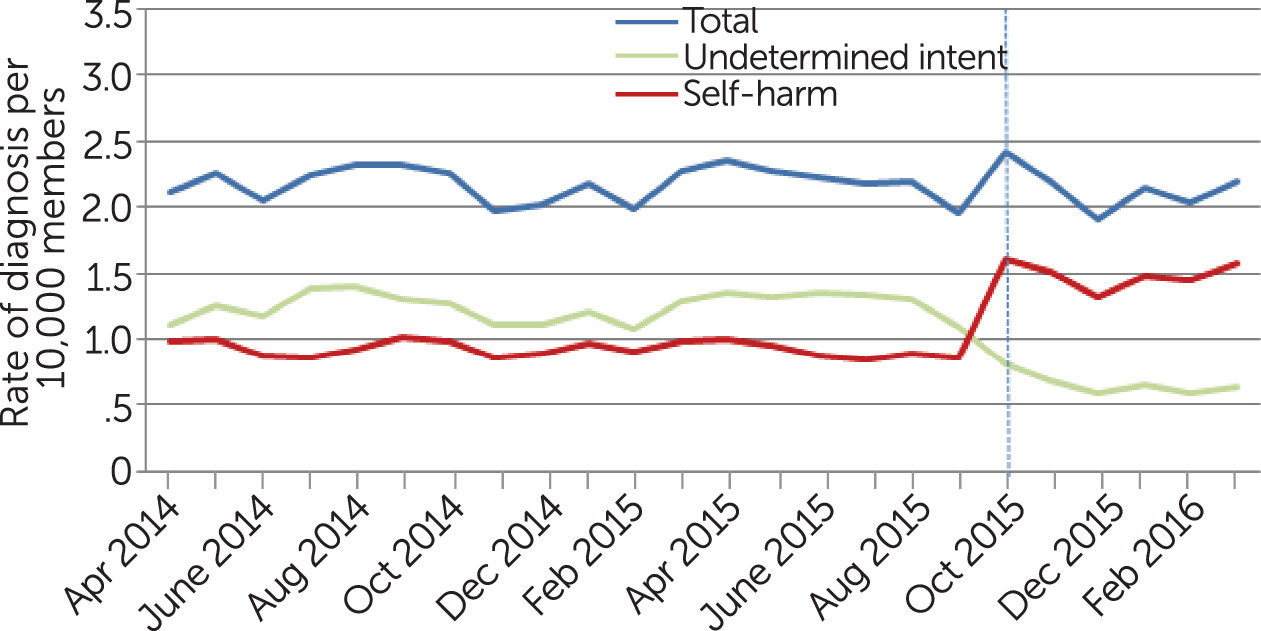
Figure 1 shows monthly rates of injury or poisoning per 10,000 enrolled members by whether the injury or poisoning was intentionally self-inflicted or of undetermined intent. Diagnoses of self-inflicted injury or poisoning appeared to increase abruptly with the coding transition, and this pattern was consistent across health systems [see
online appendix]. Diagnoses of injury or poisoning of undetermined intent appeared to decrease with the coding transition, but this pattern varied considerably across health care systems [see
online appendix].
Marked changes in coding of intent for injuries and poisonings during the fall of 2015 almost certainly represent artifacts of coding changes rather than true changes in suicidal behavior. Therefore, the transition from ICD-9-CM to ICD-10-CM may affect research, surveillance, and quality improvement related to preventing suicidal behavior and should be considered when interpreting trends during this period.
Effects of coding changes may vary across electronic health records systems or with different terminology mapping implemented in those systems. Across the ten MHRN health systems, we observed similar patterns for diagnoses of injury or poisoning with intentional self-harm and variable patterns for diagnoses of injury or poisoning of undetermined intent. Our specific findings may not generalize to other health systems, but they underline the importance of close attention to coding changes in all U.S. health care settings.