At least 100,000 individuals experience first-episode psychosis (FEP) annually in the United States (
1,
2). Early intervention for FEP is associated with improved outcomes in symptoms and functioning (
3–
6); however, there is often a substantial delay between onset of psychosis and connection to appropriate care (
7,
8). For many, the onset of psychosis results in psychiatric hospital admission, often without subsequent engagement in outpatient treatment. After hospital discharge, individuals with psychotic illnesses may not engage in care for many reasons, including lack of knowledge about treatment resources and lack of resources to ensure that links are established between patients and community treatment and supports (
9,
10).
The New York City (NYC) Department of Health and Mental Hygiene (DOHMH) sought to improve timely connection to care among individuals hospitalized with FEP. Internal DOHMH analysis using Medicaid data showed that in 2011, only 59% of New York City residents ages 18–29 who had been hospitalized in NYC for a first inpatient admission with a diagnosis of schizophrenia or psychotic disorder not otherwise specified (NOS) attended at least one mental health appointment within 30 days after discharge. Lack of connection to care following FEP contributes to adverse outcomes, including psychiatric readmission, homelessness, violence, and suicide (
11). Indeed, DOHMH’s internal analysis of Medicaid data indicated that in 2011, nearly half (47%) of NYC residents ages 18–29 who had received psychiatric treatment in a NYC hospital and who had not had at least one outpatient mental health appointment within 30 days of discharge were readmitted for inpatient mental health treatment within 1 year. Although every individual in the analysis did not necessarily have FEP, facilitation of engagement in appropriate services can be particularly important for those with FEP. Research supports that early detection systems and development of mechanisms to improve treatment referral within health systems can have a positive impact in connecting individuals with FEP to care (
12).
DOHMH implemented a novel program in 2014 to improve outcomes and linkages to care for individuals experiencing a psychiatric admission for FEP. The NYC Board of Health amended the city’s health code to require that all 38 NYC hospitals that provide adult inpatient psychiatric services report to the DOHMH when a person ages 18–30 with a qualifying diagnosis is admitted for the first time since reaching age 18 (hereafter, FEP) (
13). Qualifying diagnoses are schizophrenia, psychotic disorder NOS, schizophreniform disorder, delusional disorder, schizoaffective disorder, brief psychotic disorder, shared psychotic disorder, other specified or unspecified schizophrenia spectrum disorder, and other psychotic disorder (
14). This change in the health code occurred following public hearings and consultation with client advocates and providers and was structured to address their concerns.
To respond to these notifications from hospitals, DOHMH created a specialized program designed to improve the connection to community-based care for individuals hospitalized in NYC for FEP. The NYC Supportive Transition and Recovery Team (NYC START) is composed of a program director, two clinically trained social work supervisors, nine licensed social workers, and four mental health peer specialists with lived experience of mental illness. As designed, the program model assumes that social workers would carry caseloads of approximately 12 active clients. Although social workers have the primary care coordination and treatment planning responsibilities for each client on their caseload, the program is designed for peer specialists to share caseload responsibilities with several SWs, act as consultants on peer-related goals, and work with active caseloads of 24 to 36 clients.
The team offers care coordination, psychoeducation, and support services to young adults who have been hospitalized for the first time with FEP and their families. For those who agree to receive NYC START services, beginning during hospital admission and for 3 months following hospital discharge, the team uses a critical time intervention (CTI) care coordination model and a shared decision-making approach to help ensure linkage to care, connect clients to specialized and recovery-oriented services, and support their transition back to the community. These services include care coordination; peer support services; family support; assistance with reducing substance use; assistance with finding housing or employment or with resuming education; and assistance with engaging with outpatient mental health treatment and primary care services. Staff are highly mobile, spending 3.5 days per week in the field performing community visits and 1.5 days in the office for staff meetings, clinical supervision, documentation, and care coordination activities that can be done from an office.
CTI is an evidence-based, time-limited model originally developed to address recurrent homelessness and other adverse outcomes among individuals with severe mental health conditions in the NYC shelter system (
15,
16). The model has successfully been adapted as a short-term intervention to support individuals who are adjusting to a critical time of transition in their lives, including the transition from psychiatric hospital admission to outpatient treatment (
17). In creating NYC START, DOHMH adapted the CTI model to provide 3 months of care coordination services for individuals hospitalized with FEP, with a focus on connecting these individuals to coordinated specialty care programs and other formal and informal community support services (
1). Following the CTI model, the intensity of visits and other contacts is expected to be highest in the 30 days after hospital discharge, averaging about once a week, and decreasing to once every 2 weeks as clients negotiate the transition to the community. In the event that a client experiences a crisis or decompensates at any time during program involvement, service intensity can be increased to meet the client’s needs (i.e., “stepping in and stepping out”). The program also is designed to offer flexibility in the type of supports offered, such as face-to-face, telephone, or text communication, based on the client’s clinical needs and personal preferences, and is tailored to the situation, such as whether a client is returning to work or school, returning to live with family, or needing help with housing.
This study examined the degree to which NYC START was implemented as intended by reviewing program activity in 2016 from two perspectives: services received by program participants and work performed by program staff. The study also examined rates of connection with outpatient clinical services after hospitalization. (A logic model for the program is available in an online supplement to this article.)
Methods
All notifications received by DOHMH of a hospital admission with an admission diagnosis of FEP and with case activity by NYC START in 2016 were reviewed. Demographic characteristics (age, gender, insurance type, and diagnosis) were compared between individuals who accepted and did not accept NYC START services. Service logs completed by program staff were summarized to determine the number of contacts per week received by clients over time, type of services provided by program social workers and peer specialists, time from program acceptance to discharge from NYC START, and connection rates with community mental health services. We examined the volume of services received by each client, noting date, type of service, and the staff member providing the service.
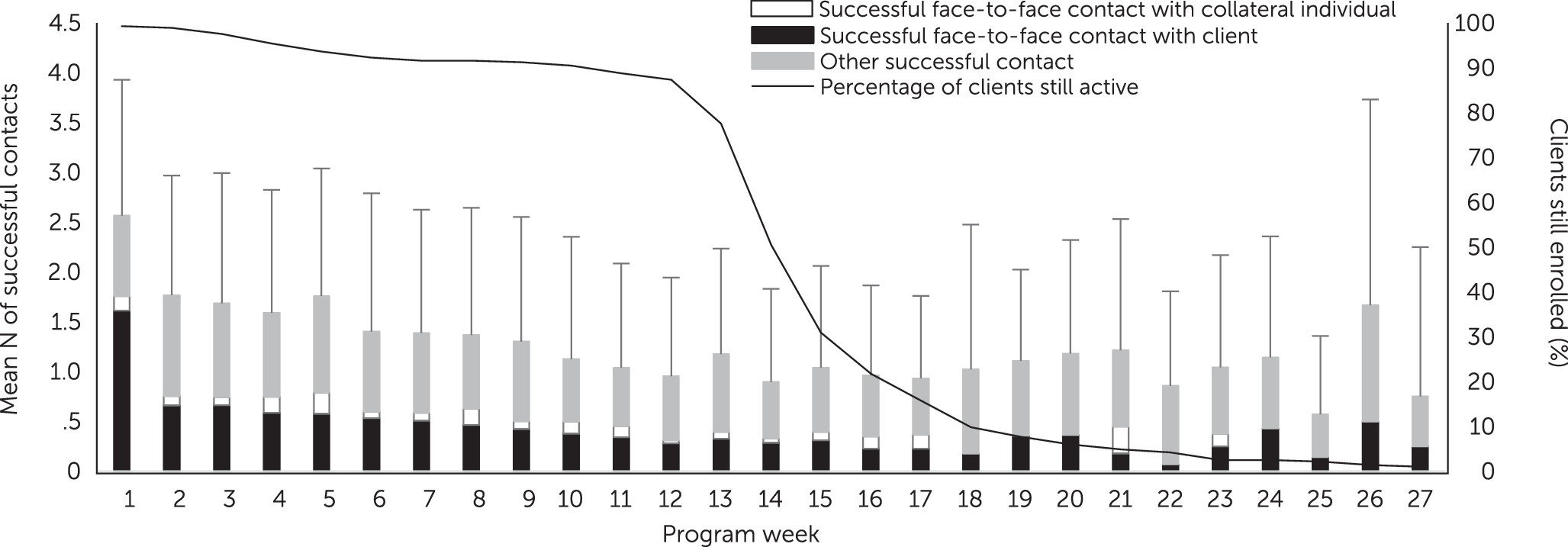
To characterize clients’ interactions with NYC START staff, we examined the mean number of services received by a client and how those services were distributed over the period of enrollment. For these analyses from the perspective of the client, we included all services provided by NYC START staff directly to clients as well as to collateral individuals (e.g., family members) or to community service providers (all “successful” contacts were included; any no-shows or unanswered calls were eliminated). These contacts included telephone calls, e-mails, texts, and faxes, as well as face-to-face contacts with the client. To observe clients’ patterns of interacting with program staff over time, we determined the mean number of contacts received by a client or collateral individual in each successive week of enrollment, beginning in week 1 with the client’s first acceptance of NYC START services. We used a Kaplan-Meier survival analysis to model clients’ length of enrollment.
To characterize the typical weekly volume of services provided by the social workers and peer specialists, we examined the mean number of staff activities per week in 2016 across all clients based on their caseload. The services were categorized as successful face-to-face contacts, attempted face-to-face contacts, other contact activity, and outreach activity to engage newly eligible individuals reported to DOHMH after a hospital admission. To avoid the biases in estimating service delivery volume that could be introduced by new or exiting employees, when quantifying service provision by staff we included data only from staff who had been employed for the entire quarter being summarized. For example, a staff member employed from January through April of 2016 contributed data to quarter 1 but not to quarter 2. These analyses characterizing staff activities included all services logged by staff on behalf of clients, independent of whether the contact was successful (i.e., including no-shows and other attempted contacts), and all outreach activity to clients prior to enrollment.
The primary outcome examined was connection of clients to services after hospitalization, defined as attendance at an initial mental health appointment at any point following hospital discharge. As a secondary outcome, we examined timely connection to services, defined as attending the initial mental health appointment within 30 days of hospital discharge.
All analyses were conducted with SAS, version 9.4, and MS Office 2013 Excel. The DOHMH Institutional Review Board determined that this activity was exempt from the federal regulations under 45 CFR §46.101 (b) (4) because it was research involving existing information (e.g., records) that will be recorded in a manner in which subjects cannot be identified, either directly or through identifiers linked to the subjects.
Results
In 2016, a total of 36 hospitals notified DOHMH of 447 individuals with an admission diagnosis of FEP (four of these hospitals were located outside NYC and contacted DOHMH regarding a NYC resident). Among the 447 individuals, 29 (6%) were determined ineligible for NYC START services: 19 (4%) had their diagnosis subsequently changed to a non-FEP diagnosis, and ten (2%) would not be residing in the NYC area after hospital discharge. The remaining 418 individuals (94%) were deemed by NYC START to be eligible for its services. Fourteen eligible individuals were discharged from the hospital before NYC START staff completed an outreach visit to offer services, and the team was subsequently unable to locate them in the community. Of the 404 eligible individuals who were approached and offered admission to the NYC START program, 285 (71%) agreed to receive services. Demographic and clinical characteristic of those who did and did not enroll in NYC START are described in
Table 1. Among the 285 who enrolled, 67% were male, 48% were black, and 60% had Medicaid. Differences between those who enrolled and those who did not were not significant.
Among the 285 individuals who accepted services, 222 (78%) continued receiving services for at least 3 months and 63 (22%) terminated services prior to 3 months, including 26 (9%) who were discharged at their request, 20 (7%) who were unable to be located, and 17 (6%) who had another reason for not completing the program—including moving out of NYC, transferring to long-term hospitalization, and being jailed or incarcerated. Half of the terminations by the client occurred within the first 6 weeks of the program. As shown in the survival curve in
Figure 1, about half of all clients were discharged from NYC START by 3 months, with 31% of clients (N=88) still enrolled by the end of week 15.
Figure 1 shows the mean number of successful contacts with NYC START staff received by clients per week. During their first week in the program, clients had a mean±SD of 2.5±1.4 contacts, 1.9 of which were with social workers and 0.5 of which were with peer specialists. Most contacts were face to face during the first week of the program, and in subsequent weeks most contacts were by other means, such as phone, text, and e-mail, with the likelihood of receiving a face-to-face contact remaining at about 0.5 per client per week for as long as the client was enrolled.
Examining the workload from the perspective of program staff,
Figure 2 shows the mean number of staff activities per week in 2016. Social workers provided a mean of 17.3±4.4 client-specific activities per week, and the mean for peer specialists was 8.5±3.5 (t=−3.55, df=11, p<0.01). Of the client-specific activities per week, social workers provided a mean of 4.0±1.0 successful face-to-face contacts and peer specialists provided a mean of 3.6±0.8, a nonsignificant difference. During this period, the mean caseloads for social workers and for peer specialists were 11.7±2.0 and 22.3±7.6 clients, respectively (t=4.08, df=11, p<0.01).
After hospital discharge, 249 (87%) clients attended an initial outpatient mental health appointment while participating in NYC START, and 226 (79%) attended the initial outpatient mental health appointment within 30 days of hospital discharge.
Discussion
The analyses indicated that as intended, the NYC START program model was implemented as a CTI and that for most clients, it lasted about 3 months, was most intensive at the beginning of the program, involved contacts with collateral participants as well as clients, and used remote and face-to-face contacts. Clients participating in the NYC START program had very high rates of connecting with mental health services, with 79% attending an outpatient mental health appointment within 30 days of hospital discharge. The distribution of services across clients and across time suggests that the program titrated services according to clients’ needs, as indicated by the great variability in the number of contacts received per client per week and by the lack of a rigid cutoff in program services once the expected duration of 3 months was reached (
Figure 1). Once enrolled, few individuals (7%) were lost to follow-up, suggesting that NYC START staff provided services that were welcomed by a large majority of eligible individuals.
By design, social workers conducted most of the outreach to individuals hospitalized for FEP in order to describe NYC START and offer enrollment. Although there was great variability across program staff, most staff averaged three or four face-to-face encounters per week with clients or their collaterals. The mean number of face-to-face contacts provided by social workers and peer specialists was similar, even though, on average, social work staff logged significantly more activities per week than did peer specialists. In addition to the face-to-face contacts, social workers are responsible for outreach in response to notifications from hospitals of qualifying admissions and have a greater degree of overall case management responsibility. Some of the difference in volume of activities may also reflect the fact that peer specialists more often engaged in tasks of longer duration, such as accompanying a client to an appointment or assisting with entitlement applications. The caseload of 11.7 clients per social worker was as anticipated; however, the caseload of 22.3 clients for peer specialists fell somewhat short of the 24–36 clients anticipated when the program was designed. These service utilization data have begun to be shared with staff as part of discussions about how best to manage time-consuming client activities, improve workload expectations, and program performance.
This study had several limitations. Although NYC START serves a very large city, it is only a single program with a small number of staff; therefore, the findings about workload may not be generalizable to other settings. Furthermore, staff may have failed to complete some service logs, resulting in an underestimate of client-related activities. Most staff used public transportation for face-to-face contacts and outreach, and clients were not assigned to staff on the basis of geography, resulting in some lengthy travel times and fewer contacts. Travel time was not logged, which may also contribute to the apparent variability in the volume of activities completed across staff. This was a study of program implementation and, as such, had no comparison group. Therefore, we could not estimate how many people would have connected to services after hospitalization without NYC START services. However, the NYC START 30-day connection rate of 79% is promising in that it is higher than the rate observed in the DOHMH Medicaid analysis, which showed that only 59% of NYC young adults had attended a mental health appointment within 30 days after discharge from a psychiatric hospitalization. Other local governments may wish to fund such specialized coordination services and enact regulations requiring hospitals to notify the specialized services when someone is hospitalized with FEP to enhance the likelihood that people hospitalized with FEP are connected with the most appropriate types of community support available.
Conclusions
The enactment of regulations in NYC requiring hospitals to alert the DOHMH when a young adult is hospitalized with FEP has allowed the city’s NYC START initiative to act as a CTI to connect individuals hospitalized with FEP with relevant services. The program has been well received by clients, as evidenced by high enrollment rates, with the vast majority of those who enroll continuing in mental health services before discharge from NYC START.